
Abstract
Osteomas are benign bone tumors commonly involving paranasal sinus walls. They are divided into three groups as ivory, mature, and mixed form. We reported demonstrative radiological features of an unusual case of giant osteoma presenting with proptosis and diplopia.
Significance Statement
Osteomas are benign bone tumors commonly involving paranasal sinus walls. They are divided into 3 groups as ivory, mature, and mixed form. We reported demonstrative radiological features of an unusual case of giant osteoma presenting with proptosis and diplopia.
Introduction
Osteomas are rare benign bone tumors. They are usually seen in the craniofacial region, particularly in the paranasal sinuses. Incidence of paranasal sinus osteomas in the general population is 0.43%. 1 They are more common in male and require surgery if they cause symptoms. 2 Osteomas are generally asymptomatic due to their slow growing nature and they are noticed incidentally on radiological examinations performed for other reasons. Clinical manifestations of sinonasal osteomas are usually localized headache, rhinosinusitis, and facial disfigurement. Computed tomography (CT) views are quite typical and it is rather easy to diagnose radiologically with this appearance: a sharply defined, lobulated, homogeneously dense calcified tumor that grows by taking the shape of the sinus of origin. If the tumor is large enough, it may extend to the neighboring structures and therefore, complications such as proptosis, diplopia, cerebrospinal fluid rhinorrhea, brain abscess, pneumatocele, and meningitis can develop. In this article, we report an unusual case of giant osteoma presenting with proptosis and diplopia.
Case Presentation
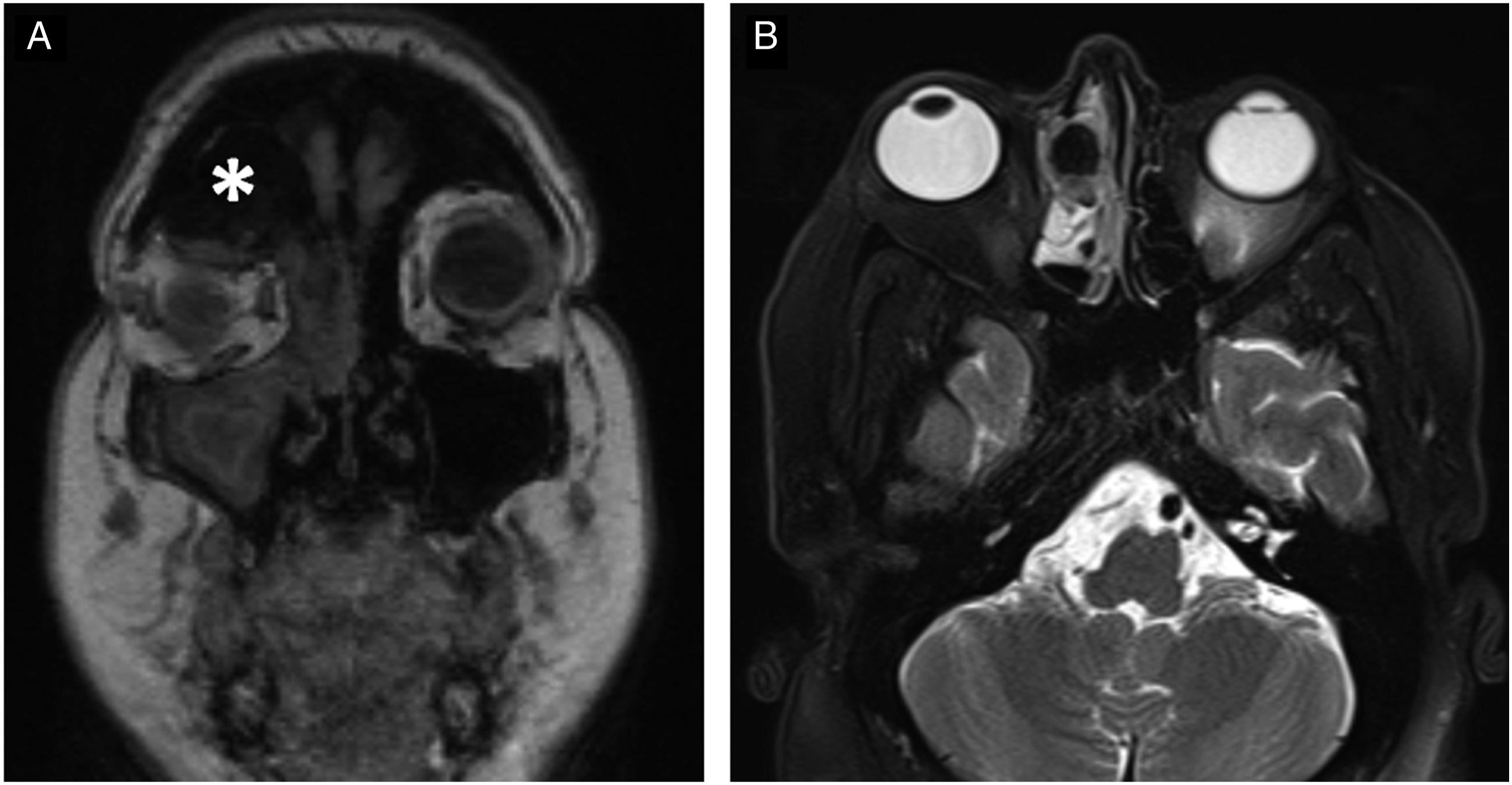
A 64-year-old female referred to the ophthalmology department with complaint of diplopia, frontal headache, and proptosis in the right eye. On examination, there was hard swelling on the right anterior frontal region, a facial asymmetry and a right proptosis. Computed tomography scan revealed a lobulated, sharply defined, homogeneously dense calcified mass measuring approximately 35 × 53 × 65 mm arising from the right frontal sinus with extension into the right ethmoid sinus and medial wall of the orbit (Figure 1A-B). Magnetic resonance (MR) imaging was performed for differential diagnosis and to reveal its association with anatomic structures adjacent to the lesion. On MR images, the lesion was hypointense in all sequences, and there was no enhancement in post-contrast T1-weighted MR images (Figure 2A). MR images also showed right ocular proptosis (Figure 2B). According to the radiological and clinical features, we thought that the lesion was osteoma. At the 5-year follow-up, we did not see any significant change in its size and nature. So we didn't suspect any malignant process. The differential diagnosis could include another benign lesion, a fibrous dysplasia. However, there was no “ground glass appearance” in CT scans. The lesion was very dense on CT. (A) Anterior view bone reconstruction volume rendering cranial CT shows supra-orbital and frontal osseous mass (asterisk). (B) Coronal CT scan reveals a hyperdense osteoma (asterisk) protruding into the right fronto-ethmoid sinuses. (A) Post-contrast coronal T1-weighted MR image shows a hypointense non-enhanced frontal lesion (asterisk). (B) Axial T2-weighted orbital MR image reveals right ocular proptosis.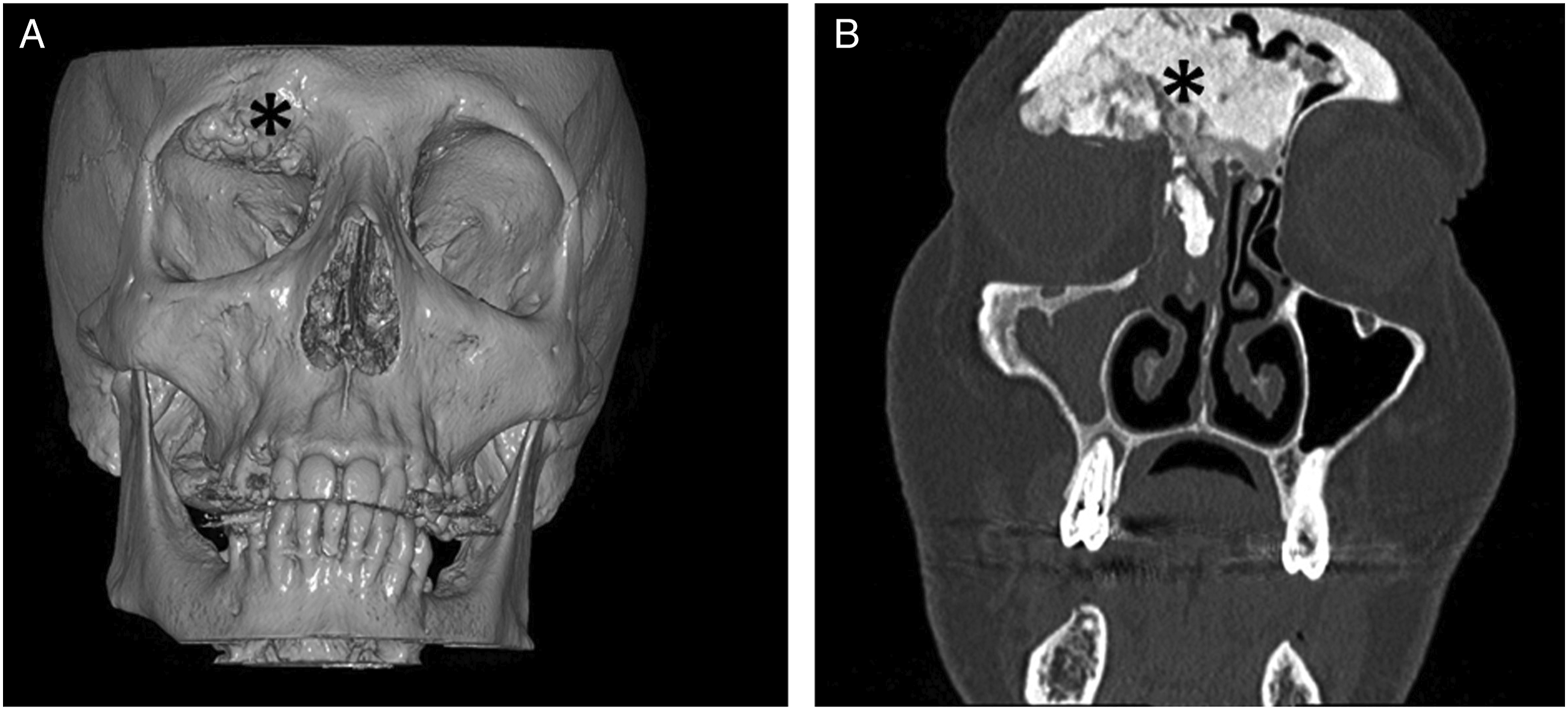
Conclusion
Giant osteomas are defined as osteomas greater than 3 cm in size are very rare tumors. Frontal sinus is the most commonly affected area and is followed by ethmoid, maxillary and sphenoid sinuses. Even though etiology is not yet clear; traumatic, inflammatory and embryologic hypotheses, or a combination of these factors are nowadays accepted as possible etiologies.
Because of nonspecific symptoms, the diagnosis may be delayed. 2 -4 Meningitis, brain abscess, pneumatocele, or cerebrospinal fluid leakage may occur, if osteomas grow into the anterior cranial fossa. 2,5,6 Secondary orbital invasion is not a frequent finding and is usually seen in frontal, fronto-ethmoid, and ethmoid located osteomas. In its orbital extension, eyeball displacement with diplopia and proptosis and eventually a limitation of extraocular movements may be seen. Orbital emphysema, cerebrospinal fluid rhinorrhea and amaurosis are relatively rare events.
Computed tomography scan demonstrates a sharply defined, lobulated, homogeneously dense ossified tumor that grows by taking the shape of the sinus of origin. On MR images, ivory osteomas and mature osteomas have low signal intensity in all sequences. However mature osteomas may show similar signal intensities to bone marrow unfrequently. Differential diagnosis can include osteoblastoma, fibrous dysplasia, osteoid osteoma, chondroma, and ossifying fibroma.
In conclusion, giant size osteomas of the maxillofacial region are rare tumors and can be cause of serious complications. CT and MR images clearly show eventual extension and association to adjacent structures to the lesion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.