
Abstract
Carcinosarcoma ex pleomorphic adenoma (CCPA), also known as true mixed malignant tumor, is an extremely rare high-grade aggressive tumor. The histopathologic examination is the gold standard for diagnosis and radiologic imaging also plays an important role. CCPA should be considered in the differential diagnosis of salivary gland tumors when there are findings suggestive of malignancy such as necrosis and diffusion limitation on imaging.
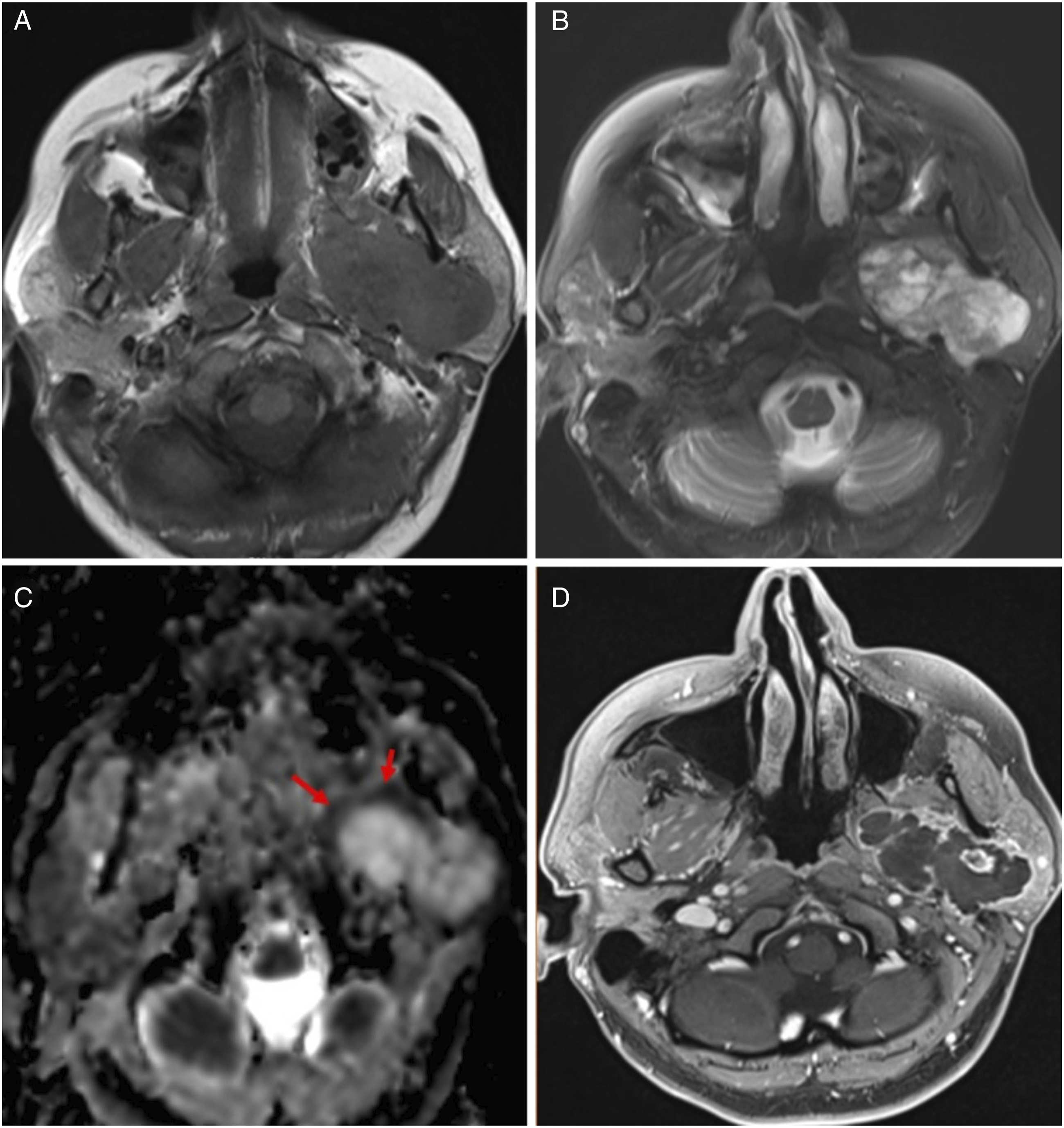
We present two extremely rare case of CCPA. In the first case, a 41-year-old female patient was admitted to our center with dysphagia, facial pain, and swelling on the left side of the face. Contrast-enhanced computed tomography (CT) images revealed a relatively well-circumscribed mass in the deep lobe of the left parotid gland that was not clearly distinguishable from the masticator space. The mass was 5x4x4 cm in size, contained cystic-necrotic areas, and had peripheral, septal contrast enhancement (Figure 1). Magnetic resonance imaging (MRI) showed a multiloculated cystic mass lesion that was hypointense on T1-weighted images and hyperintense on T2-weighted images (Figures 2A and 2B). The lesion had peripheral and locally internal diffusion restriction and was markedly contracted in these areas (Figures 2C-2D). Fine niddle aspiration was performed and the histopathological diagnosis was made as pleomorphic adenoma. The patient's mass was completely resected by the surgeon. Histopathological examination revealed the presence of sarcoma and carcinoma areas adjacent to pleomorphic adenoma regions in the resection material. In the axial (A) and coronal (B) contrast CT images of the first case, a mass lesion containing cystic-necrotic areas with relatively irregular borders is observed in the deep lobe of the left parotid gland. On axial section MR images of Case 1 shows a hypointense lesion on T1-weighted images (A) and heterogenous hyperintense lesion on T2-weighted (B) images. In the ADC map, there is peripheral restriction (C, arrows) in the lesion and peripheral heterogenous enhancement in the postcontrast series (D).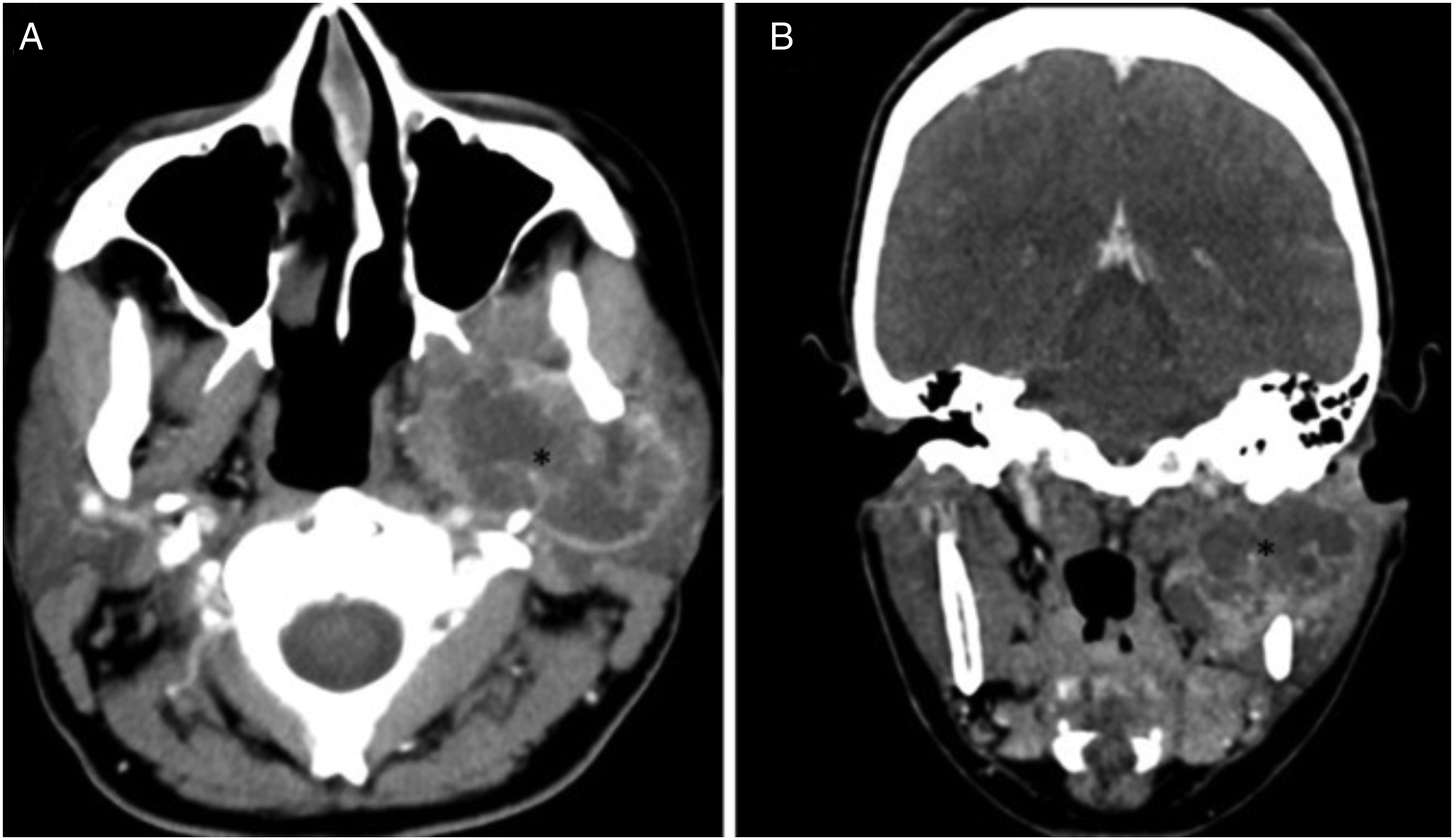
The second case was a 56-year-old male patient who presented with dysphagia and pain. CT images revealed a lesion approximately 5 × 4 × 5 cm in size, with heterogenous contrast and cystic-necrotic areas (Figure 3A). Biopsy was recommended. However, the patient did not accept. Six months later, the patient was admitted to our center with a large palpable mass on the right side of the neck that prevented him from swallowing and breathing. MR imaging showed a 14 x 12 x 9 cm giant mass with heterogenous hypointense on T1-weighted images, heterogenous hyperintense on T2-weighted images and marked diffusion restriction (Figures 3B-3D). In tru-cut biopsy, the patient was diagnosed with CCPA. In the axial section contrast-enhanced CT images of the second case, a heterogenous mass lesion in the right parapharyngeal space, which cannot be clearly differentiated from the deep lobe of the parotid gland, is observed (A). T1-weighted axial section MR image shows a giant hypointense lesion in the right cervical region. On T2-weighted axial (B) and coronal (C) sections, the lesion is heterogeneously hyperintense and obliterated into the airway by rupture of the capsule (arrowheads). The lesion shows marked restriction on ADC maps (arrows).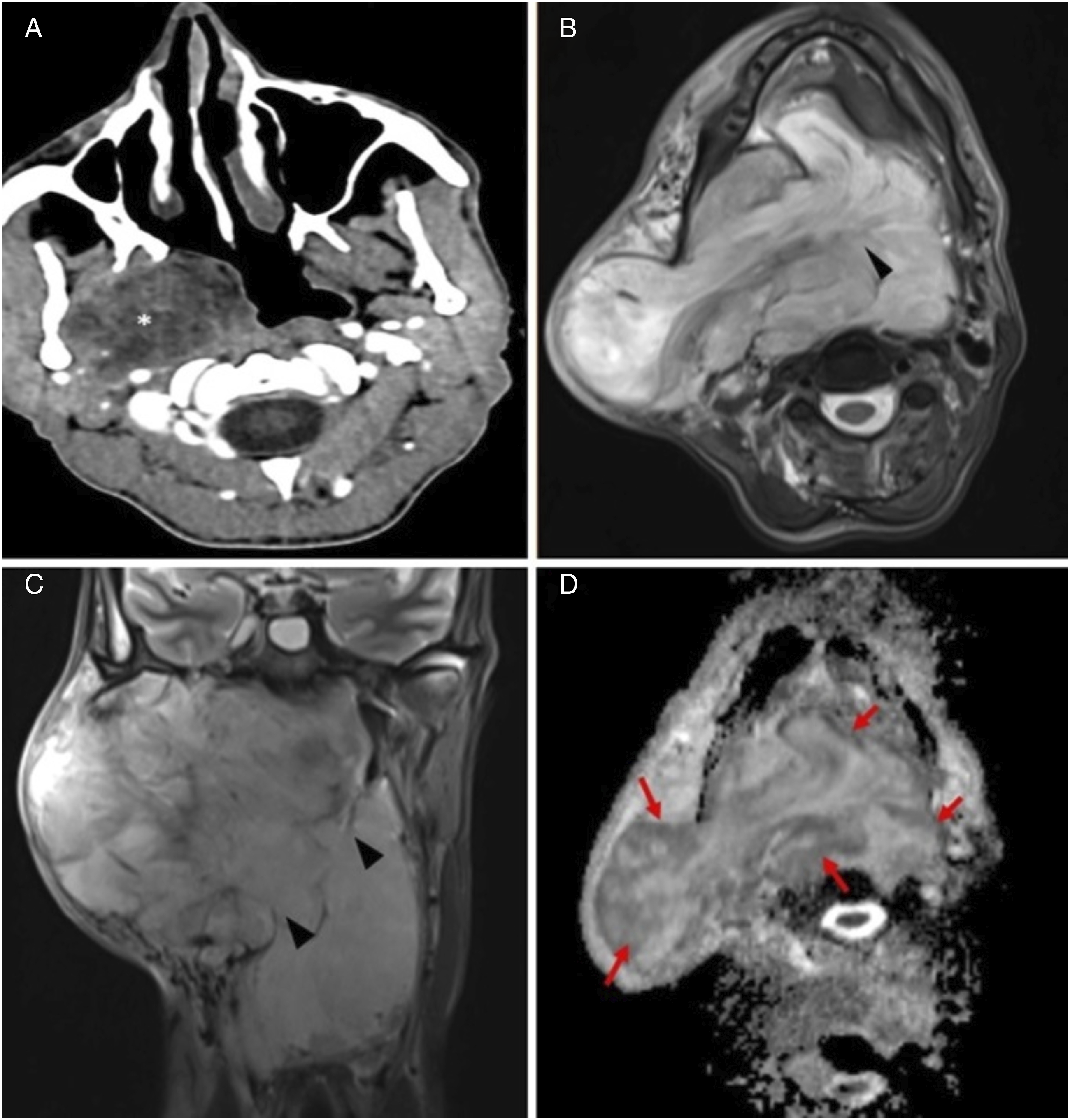
Carcinosarcoma ex pleomorphic adenoma is very rare tumor that occurs in 2 out of 100 million. It has been reported in approximately 150 cases in the literature to date. 1 Carcinosarcoma of the parotid gland accounts for only 0.05% of all salivary gland tumors and accounts for 0.1% of all malignant salivary neoplasms. 2 While there is pleomorphic adenoma in approximately 1/3 of the cases, it develops de novo in the others. It is most common in the parotid gland (67%), followed by the submandibular gland (19%) and soft palate (24%). 2 It is generally seen in elderly patients (mean age: 58 years) and there is no gender dominance. Radiological features are nonspecific as they contain different types of tissues. 3 Definitive diagnosis is made histo-pathologically. Surgery is usually used in the treatment, followed by radiotherapy and chemotherapy. 2 In this report, we presented the imaging features of two rare case of CCPA. These tumors are highly aggressive and grow rapidly. 1 Our second case is the largest CCPA to our knowledge. This rapidly growing tumor has protruded into the air column due to rupture of the capsule and caused air obliteration.
Radiologic imaging plays an important role in suspecting malignancy and showing the extension of the lesion to surrounding tissues. In the MRI findings of the 3 published cases, two of them had T1 hypointense and T2 hyperintense heterogenous contrast enhancing lesions.4,5 In other patient, increased intensity in T1 and hypointense T2 were observed. 6 Most lesion was well-circumscribed (2/3). H. Kato et al. analyzed MR images of four carcinomas ex pleomorphic adenomas. 3 They stated that the signal intensities of these lesions may vary due to different tissue contents. However, it has been remarked that the decrease in ADC values is important in terms of malignancy. MR images were similar in our cases, and there were prominent hypointense appearances in the ADC in some regions. In the second case there was a prominent capsule and in both cases the borders were irregular in some places. Although CCPA is extremely rare in the neck, it should be considered in the differential diagnosis when there are findings suggestive of malignancy such as necrosis and diffusion restriction on imaging methods.
Footnotes
Author Contributions
EG—Conceptualization, Data collection, Writing initial draft. HO—Writing initial draft, Editing, and Supervision. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to participate
Ethics committee approval was not considered necessary because it was a case report. Informed consent was obtained from the patient for this study.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images
Availability of Data and Materials
Not applicable