
Abstract
Synovial sarcoma (SS) is a rare malignant tumor with bidirectional differentiation potential in epithelial and mesenchymal tissues and is a more chemosensitive subtype of soft tissue sarcoma. It occurs around the synovial soft tissues of large joints of the extremities and rarely in the nasopharynx. We present a young man with recurrent left-sided nasal congestion with nosebleeds, confirmed by immunohistochemistry and cytogenetic examination as SS. SS is easily misdiagnosed, and the tumor should be considered in the differential diagnosis, with surgery combined with radiotherapy as the primary treatment option.
Introduction
Sarcomas account for 1% of all adult malignancies and include 2 major groups: 1 soft tissue sarcomas and osteosarcomas. 2 SS accounts for 8% to 10% of soft tissue sarcomas.3 –5 SS of the nasopharynx is even rarer, with a more aggressive nature, 6 high metastasis rate, and poor prognosis.7,8 Here, we report a case of SS originating in the nasopharynx, emphasizing the importance of immunohistochemistry combined with cytogenetic examination to avoid misdiagnosis and surgery combined with radiation therapy as an excellent treatment.
Case Report
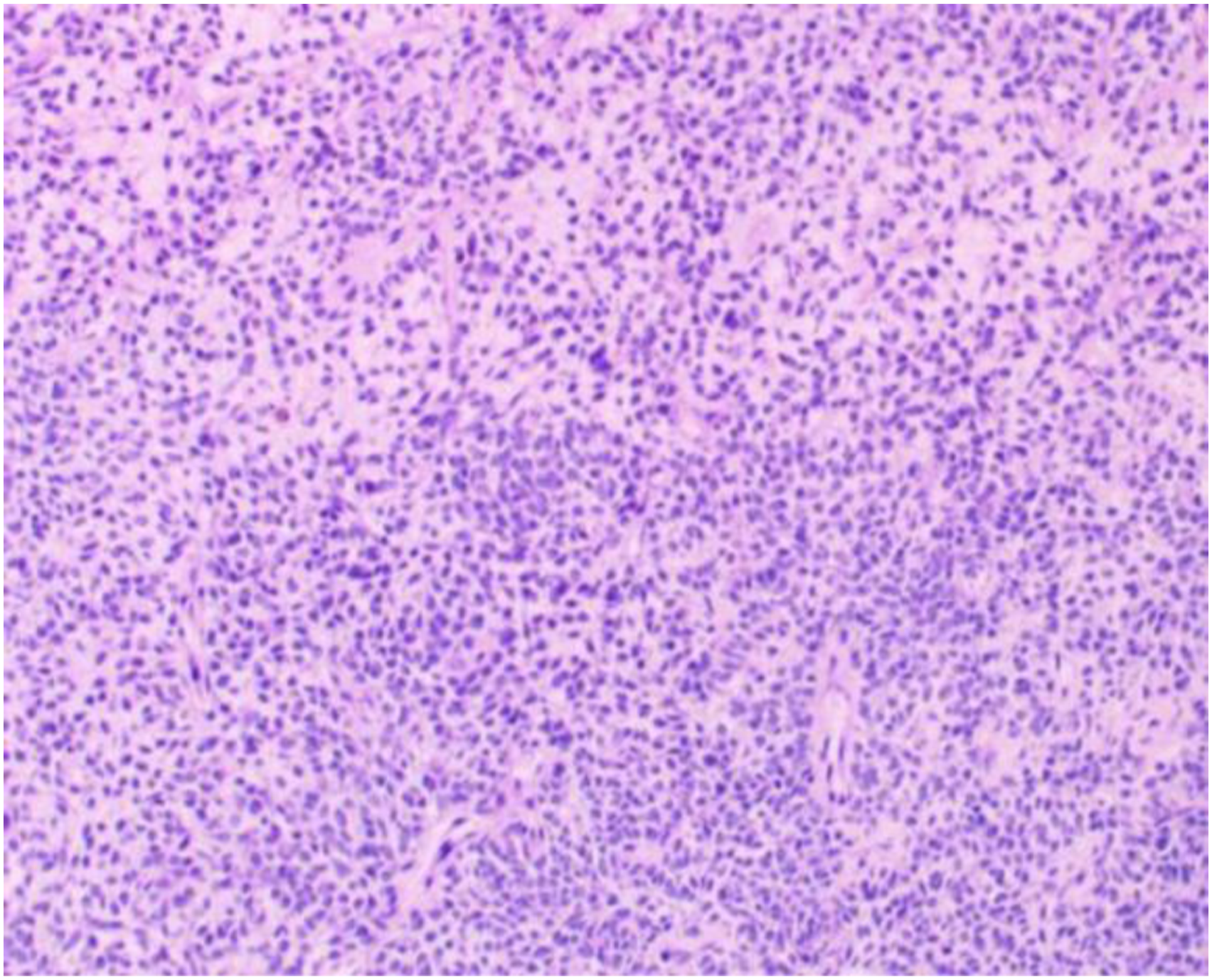
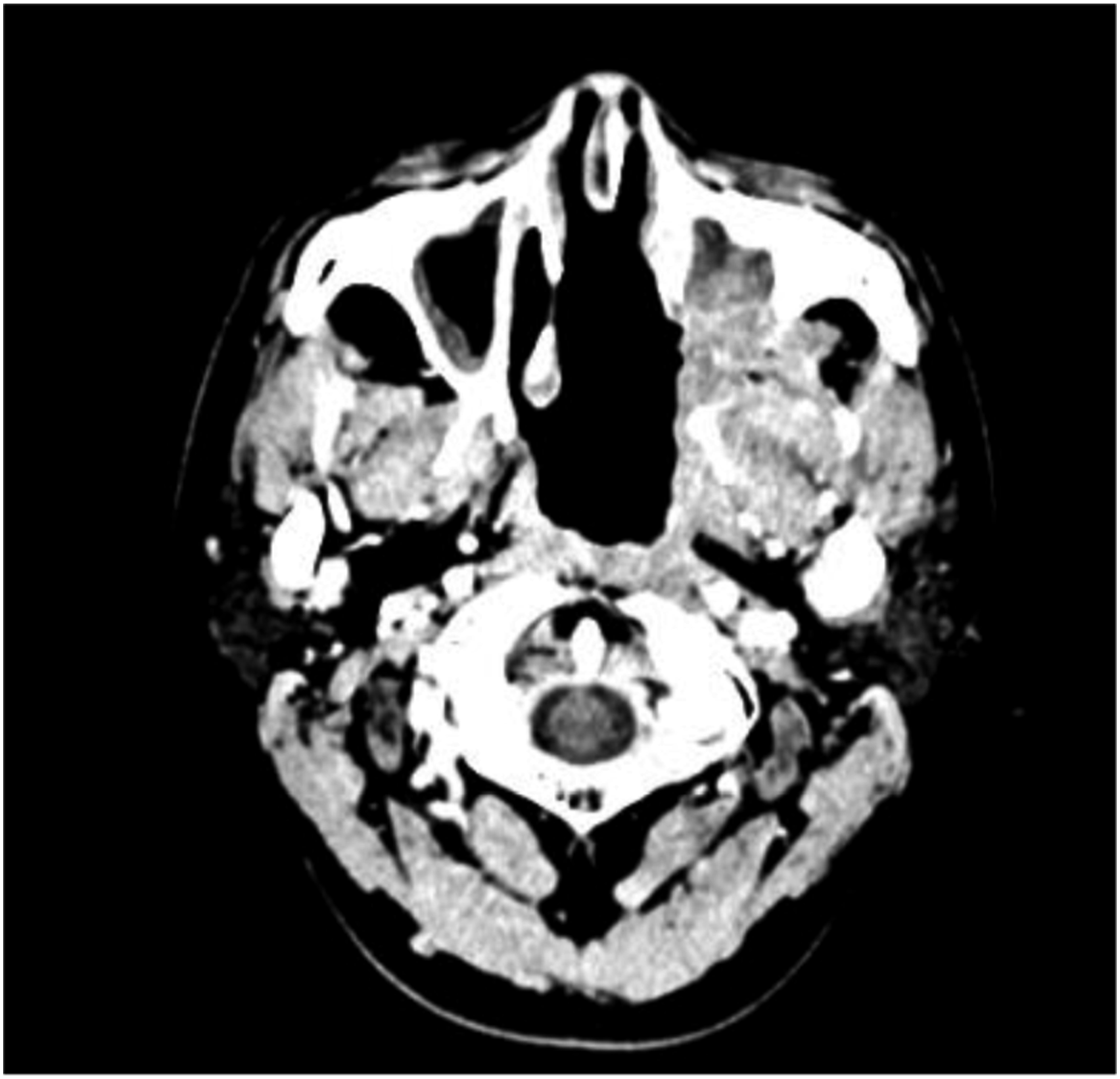
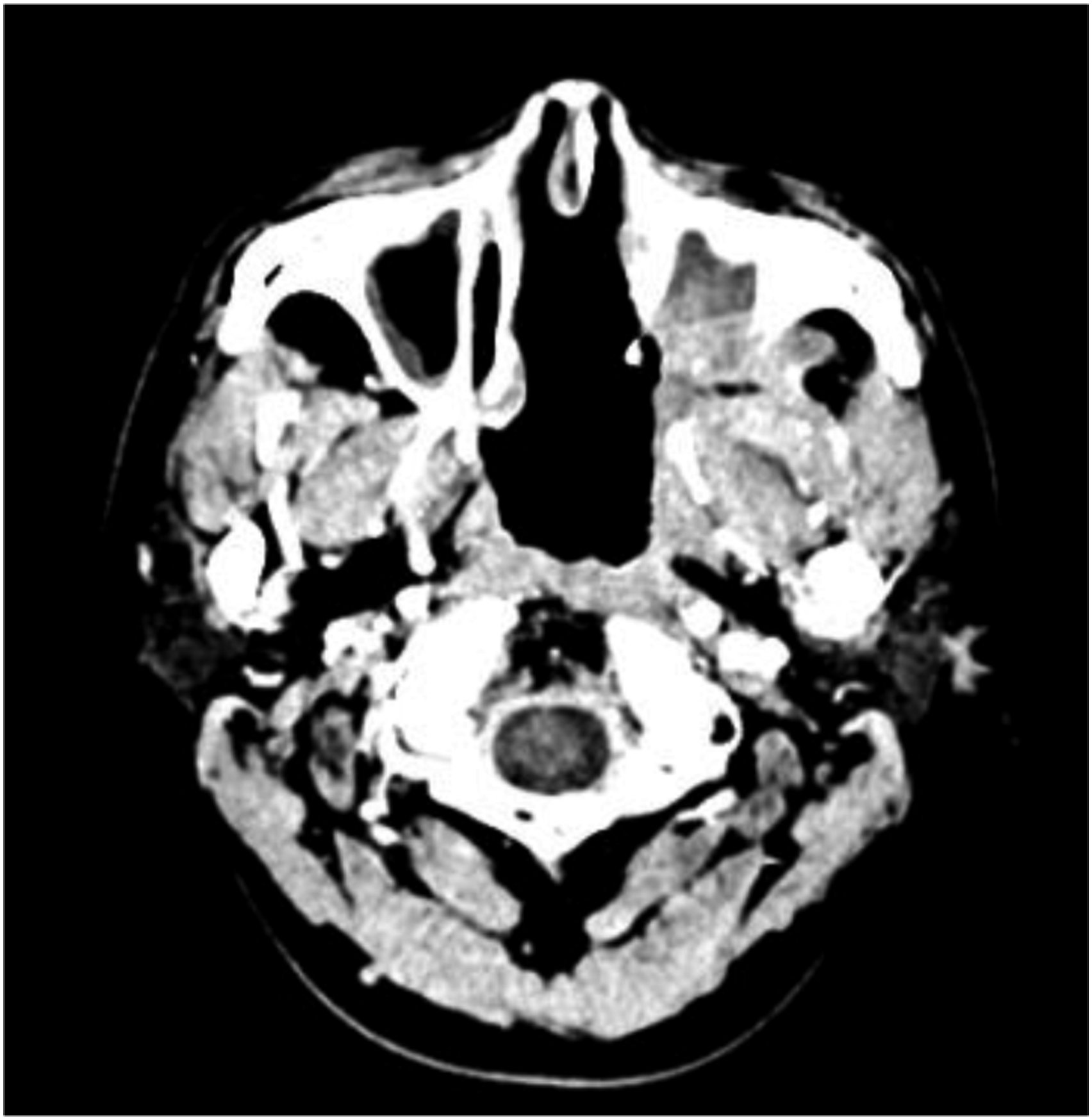
A 24-year-old male was admitted to the hospital with recurrent left-sided nasal congestion and with nosebleeds. Two months prior, the patient developed persistent left-sided nasal congestion with nosebleeds, as well as pain in the left jaw and hearing loss in the left ear without any obvious cause. Subsequently, the patient felt that the above symptoms had worsened and therefore came to our hospital. Physical examination: The posterior portion of the left nasal cavity was filled with a bulging neoplasm, and traces of bleeding were visible on the surface with purulent secretions. A bulging neoplasm was seen at the top of the nasopharynx occupying 4/5 of the lumen, and the structures of the nasopharyngeal structures were indistinct. Electronic Nasolaryngoscope showing: nasal neoplasm? Nasopharyngeal neoplasm? (Hemangioma cannot be excluded). Computed tomography (CT) of the nasopharynx showed (Figure 1): a soft tissue density mass of approximately 4.3 cm × 3.1 cm in size was seen in the left posterior parietal wall of the nasopharynx, which protruded into the left septal sinus and was considered primarily a neoplastic lesion, with multiple lymph nodes in the bilateral submandibular and carotid sheaths showing partial enlargement. The patient underwent nasal and nasopharyngeal biopsy after surface anesthesia with bupivacaine, and the postoperative pathological diagnosis showed a “nasopharyngeal” leaning non-Hodgkin’s lymphoma. Microscopically, there were short spindle-shaped cells diffusely arranged. The nuclei were spindle-shaped or ovoid, deeply stained. The cytoplasm of the cells was few and indistinct, the nuclei were overlapping, nuclear schizophrenic images were visible, and unequal collagen fibers were seen between the cells. It is difficult to differentiate the diagnosis from other spindle cell tumors in terms of cellular histomorphology. Further immunohistochemistry showed (Figure 2): in situ hybridization EBER1/2 (−), TIA-1 (−), CD56 (+), granzyme B (−), Ki-67 (+, ∼20%), CD2 (−), CD3 (−), CD20 (−), CD79a (−), CD10 (−), mum1 (−), Bcl-2 (+), Bcl-6 (−), S-100 (−), CK (−), Syn (−), CgA (−), desmin (−), Myogenin (−), MyoD1 (−), CD99 para nuclear punctate (+), CD34 (−), SATB-2 (−), TLE-1 (+), CyclinD1 (−), NKX2.2 (−), SOX-10 (−), HMB-45 (−), NSE (−), Fli-1 (−), ERG (−), Melan-A (−). SYT gene break fluorescence in situ hybridization (FISH) assay: SS18-SSX gene translocation was detected. Combined with the above results, SS was considered. The patient has been treated with a skull base tumor resection + palatopharyngoplasty + (left) sinus opening endonasal endoscopic whole group + (left) cervical lymph node dissection + tympanostomy and drainage + (left) transnasal endoscopic pterygoid neurectomy under general anesthesia, and a grayish white brittle mass was seen in the left nasopharynx during surgery. One month after surgery, the patient returned to our hospital and received 2 cycles of chemotherapy (Epirubicin 60 mg + Isocyclophosphamide 2.5 g + Mesna 400 mg). Then he received radiation treatment for nasopharyngeal lesions and positive lymph nodes and lymphatic drainage areas (phase I: P-CTV: 50Gy/25Fx, Phase II: P-GTV: 22Gy/10Fx, P-GTVn: 20Gy/10Fx). The patient undergoes one cycle of chemotherapy again after the end of radiotherapy (same protocol as before). A repeat nasopharynx-enhanced magnetic resonance imaging (MRI) at the end of all treatments showed as shown in Figure 3. There is no sign of tumor recurrence in the follow-up so far, and the CT of the nasopharynx was recently reexamined, as shown in Figure 4, which is still under continuous follow-up. Preoperative nasopharyngeal CT scan. Microscopically, short spindle-shaped cells are diffusely arranged, with spindle-shaped or ovoid nuclei, deep staining, little and indistinct cytoplasm, overlapping nuclei, and visible nuclear schizophrenia, and unequal collagen fibers are seen between cells. (HE×100). MRI-enhanced scan of the nasopharynx. Recent CT scan of the nasopharynx.
Discussion
SS most commonly occurs in and around the large joints of the extremities, and the primary nasopharynx is less common. Only 8 cases of nasopharyngeal SS have been reported by Nakahira M et al. SS can occur at any age but is most common in men between 20 and 40 years of age.9,10 In the present case, the patient was a 24-year-old man, which is more consistent with studies from previous years. SS lacks specificity in imaging, and not all patients show “peripheral calcification” on CT or “triple signal sign” on MRI, 11 so it is difficult to diagnose the disease based on imaging data alone.
There are no specific immune markers for SS, while the detection of AE1/AE3, EMA, CK, CD99, Calponin, Viment in, Bcl-2, cyclinD1, S-100 protein, and Ki-67 is favorable for the diagnosis of SS, and positive Ki-67, Bcl-2, CD99, and TLE-1 in our patient indicates that the diagnosis is more inclined to SS. 12 The initial pathological diagnosis of this patient was considered non-Hodgkin lymphoma, which is highly likely to be misdiagnosed without further investigations. B-cell lymphoma CD20 with PAX5 or CD79a is often positive; T-cell lymphoma CD3 with CD2 or CD45RO is often positive. Immunohistochemical examination of this patient showed negative for the above immunomarkers, indicating that the diagnosis of non-Hodgkin lymphoma is unlikely. According to the cytogenetic characteristics of SS, its X chromosome and chromosome 18 can translocate to each other to form the fusion gene SYT-SSX which promotes tumorigenesis, so the SYT-SSX test is considered the gold standard for the diagnosis of SS.13,14 When SS is considered by immunohistochemistry, the FISH test can be applied to aid in the diagnosis. The diagnosis of SS was confirmed by immunohistochemistry and the translocation of the SS18-SSX gene detected by FISH.
The clinical manifestations of SS are related to the location of the tumor. In this case, the tumor was located in the nasopharynx, so the main manifestations were nasal congestion with nosebleeds, along with pain in the left jaw and hearing loss in the left ear. SS has a diverse histopathological pattern with varying degrees of differentiation, some exhibiting a benign appearance, such as an intact envelope, and often needs to be differentiated from fibrovascular tumors of the nasopharyngeal, rhabdomyosarcoma, hemangiopericytoma, nerve sheath tumors, myoepithelial carcinoma, papilloma, and nasal polyps. 15 SS is very easy to misdiagnose, and clinical caution should be exercised.
The malignancy of SS is high, and due to the complex anatomy of the nasopharynx, dense neurovascular, and many adjoining structures, it is mostly intermediate to an advanced stage and more malignant when clinically diagnosed. Surgical resection alone is highly likely to have residual tumor tissue, and to improve patient survival and reduce recurrence and metastasis, a combination of surgical treatments is often used.16,17 The prognosis of this disease may be related to the patient’s age, tumor size, and location, whether it invades surrounding tissues, and the presence of vascular cancer emboli. 18 In this case, the patient was a young male, no vascular cancer embolism or bone destruction was observed, postoperative radiation therapy and chemotherapy were administered, tumor recurrence was not seen in the follow-up so far, and the prognosis was good. Fonseca et al. suggested that follow-up is important to monitor recurrence and improve disease-free survival, and this patient is still being followed for early detection and treatment of recurrence. 19
Conclusions
SS is a highly aggressive tumor, and its diagnosis cannot be made by histopathological biopsy alone but also by combining immunohistochemical and cytogenetic examinations. Furthermore, proven nasopharyngeal synovial sarcoma (SS) requires the exclusion of metastatic synovial sarcoma, as the incidence of soft tissue synovial sarcomaof the extremity joints is much higher than that of nasopharyngeal synovial sarcoma. Based on the treatment experience of this patient, it is recommended that patients with SS in the nasopharynx should be treated with a combination of surgery and radiotherapy and be followed-up with regular imaging.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 2023ER100-1.
Ethical Statement
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Contributorship
Xuejing Xiang: Writing - original draft, collecting data, formal analysis, Data Curation. Yuanyuan Luo: Writing - original draft, collecting data, formal analysis, Data Curation. Haibo Du: Data Curation, visualization, collecting data. Xiaojie Ma: formal analysis, methodology, resources, Writing- Reviewing and Editing. All authors have read and approved the manuscript.
Data Availability
The data used to support the results of this study has received hospital ethical approval for use.