
Abstract
Primary laryngeal synovial sarcoma is an extremely rare tumor predominantly affecting young adults. There are currently no well-defined guidelines to direct investigation and management, and treatment is largely based on what is known for synovial sarcoma of the upper and lower limbs. This PROSPERO-registered study aims to review the diagnostic methods, treatment regimens, and survival outcomes for patients with synovial sarcoma of the larynx. A systematic search of databases Medline, Embase, SCOPUS, and Web of Science was undertaken in December 2017. The literature search identified 1031 potentially relevant studies, and after the deletion of duplicates and excluded papers, 98 full-text articles were screened. A total of 39 cases were reviewed from 32 studies in the data extraction. The average age at the time of laryngeal synovial sarcoma diagnosis was 32 years (range, 11-79 years). In all cases (n = 39), patients underwent wide surgical excision, with 20 patients requiring a partial or total laryngectomy. A total of 18 patients received adjuvant and 3 received neoadjuvant radiotherapy. Chemotherapy was used in 10 cases, with ifosfamide the most frequently used agent. There was considerable variability in the order and combinations of the abovementioned treatments. No clinicopathologic factors or treatment regimens were associated with improved overall survival or lower rate of recurrence. There is a paucity of literature and heterogeneity in clinical approaches to this highly aggressive sarcoma. Reporting of cases must be standardized and formal guidelines must be established to guide clinical management.
Introduction
Synovial sarcoma is a rare and aggressive soft tissue tumor classically arising from mesenchymal tissue. It accounts for 5% to 10% of all soft tissue sarcomas and most commonly affects the upper and lower limbs. 1 Primary synovial sarcoma of the head and neck is rare, accounting for less than 5% of all synovial sarcomas, with those originating from the larynx being even rarer. The most common site of head and neck synovial sarcoma is the hypopharynx. 2 However, synovial sarcoma arising from other sites including the oropharynx, 3 nasopharynx, 4 paranasal sinuses, 5 trachea, 6 and the parotid gland 7 has also been reported. Each of these heterogeneous locations is associated with varying degrees of complexity of surgical resection and morbidity from radiotherapy.
There exist only a few reported cases arising explicitly from the larynx. The first case of laryngeal synovial sarcoma was described by Gatti and Miller in 1975. 8,9 Over the last 4 decades, an increasing body of literature on cases of synovial sarcoma of the larynx has been published. Synovial sarcomas of the larynx typically present as a painless neck lump associated with airway symptoms including dysphonia, dyspnea, and stridor in advanced cases. Although the imaging pathway for initial investigation remains undefined, final diagnosis is made on the basis of tumor morphology, immunohistochemistry, and molecular studies. Histologically, synovial sarcoma tumors are comprised of varying proportions of spindle and epithelial cell components. Tumors are subtyped based on the relative presence of each component. Monophasic tumors contain only spindle cells or, more rarely, only epithelial cells. In biphasic tumors, both spindle and epithelial cell components are present. Synovial sarcoma is a translocation-associated sarcoma, defined by a t(X;18)(p11.2;q11.2) translocation involving genes SS18 on chromosome 18 (which encodes SYT or SSXT protein) and SSX1, SSX2, and SSX4 genes on the X chromosome. 10
Wide local tumor resection is the mainstay of synovial sarcoma treatment, with adjuvant radiotherapy and, less commonly chemotherapy, also administered to the affected region to reduce the known high rate of recurrence. 11 Thus, management of laryngeal synovial sarcoma presents a unique set of challenges for patient and clinician, requiring a balance to be struck between aggressive tumor treatments while attempting to preserve intrinsic laryngeal function. Extensive laryngeal resections and irradiation of the neck are often associated with permanent dysphagia, compromised phonation, and impaired ventilation, all of which may significantly impact upon patient quality of life. 12 Improved understanding of the outcomes of stand-alone surgery or combination treatment regimens may allow for a more targeted and effective treatment approach, reducing morbidity for patients without compromising cure rates.
To date, no study has systematically reviewed the treatment approaches and outcomes for synovial sarcoma of the larynx. The primary aim of this study was to determine the demographic and histopathological features of patients diagnosed with synovial sarcoma of the larynx. Our secondary aim was to compare the rates of recurrence and overall survival at follow up between each of the major treatment regimens.
Materials and Methods
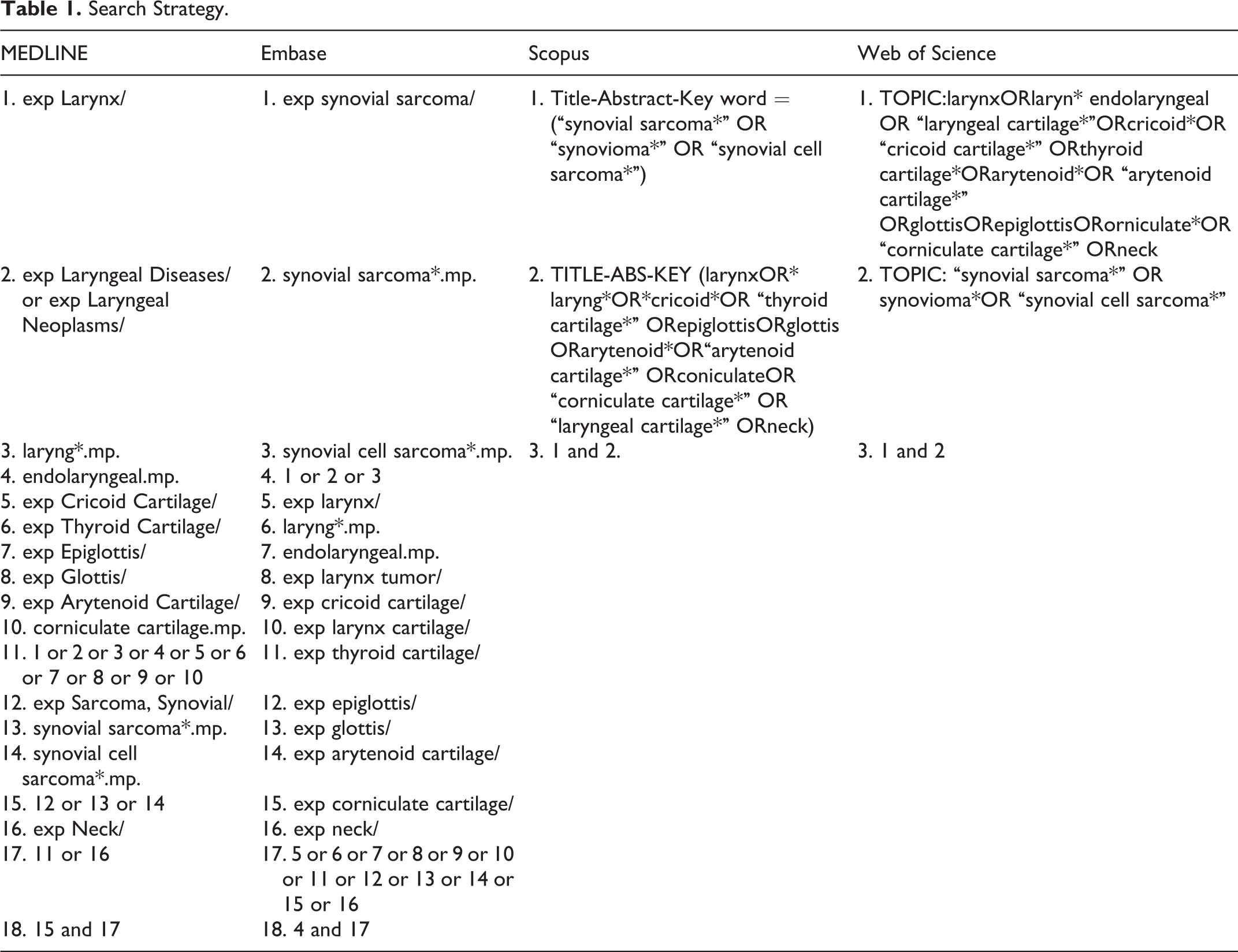
A comprehensive review of the literature was performed to identify all reported articles on synovial sarcoma of the larynx. This study was registered on the PROSPERO database of systematic reviews. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis checklist was used to guide the review process. Medline, Embase, SCOPUS, and Web of Science electronic databases were searched in December 2017 to identify cases of synovial sarcoma of the larynx. A screening of reference lists and search of the gray literature in Google Scholar was also performed to identify all cases. The Medline search combined synovial sarcoma (and synonyms “synovioma” and “synovial cell sarcoma”) with various Medical Subject Headings and free-text phrases for laryngeal anatomical structures. The search strategy was adapted for each of the other databases (Table 1).
Search Strategy.
Inclusion and Exclusion Criteria
The systematic review considered all studies reporting on cases of primary synovial sarcoma of the larynx. To meet inclusion criteria, studies needed to describe the demographic and treatment details for each case, studies needed to be written in English and published in a peer-reviewed journal, with a title, abstract, and full manuscript available. No publication date restrictions were imposed. Cases described in conference abstracts, conference posters, and letters to the editor were excluded. Cases of synovial sarcoma with metastatic spread to the larynx from a peripheral site were excluded. Cases of synovial sarcoma arising from the laryngopharynx (hypopharynx) or other pharyngeal structures were excluded.
Screening of Literature
The titles and abstracts of all studies identified by the database search and gray literature search were screened by a single reviewer, Dr Gregory Shein. From this process, the full text of each potentially relevant study was sourced and reviewed by Dr Gregory Shein and Dr Gurfateh Sandhu to determine their eligibility for inclusion. All discrepancies were resolved by consensus. Relevant data were extracted from each article according to a predesigned pivot table. Articles describing a previously published case were excluded to avoid double counting.
Data Extraction
The following data were extracted from each study: study type, publication year, location of treatment, patient age and sex, laryngeal structures involved, maximal diameter of tumor at the time of diagnosis, stage at diagnosis (localized, nodal involvement, metastatic spread), follow-up period, and patient status at follow-up. Articles were categorized as being contemporary or historical depending on whether they were published in the past 5 years (after January 1, 2013) or prior to this period, respectively. Diagnostic parameters extracted included relevant immunohistochemistry analysis, histological subtype, results of reverse transcriptase polymer chain reaction (RT-PCR), and fluorescent in situ hybridization (FISH) molecular techniques. Treatment parameters extracted included surgical technique, chemotherapy agents and treatment regimen, radiotherapy dose in Grays (Gy), field and fractions, treatment sequence, and any treatment-related complications. Outcomes including clinical state (alive with no active disease, alive with active disease, dead of disease) at follow-up and time to local and metastatic recurrence (where relevant) were also recorded.
Statistical Analysis
Statistical calculations were performed using SPSS version 25 for Mac (Armonk, New York). Descriptive statistics were presented as mean and range for continuous variables.
Quality Analysis and Extraction
The quality of the final included studies was not assessed as the valid instruments available do not assess the quality of case reports and 28 of 32 included papers were case reports.
Results
Study Selection
The search across electronic databases, reference lists, and gray literature identified 625 potentially relevant studies after the deletion of 406 duplicates. The abstracts of these studies were screened, from which the full texts of 98 studies were analyzed. A total of 32 studies remained eligible for further analysis (see Figure 1 for inclusion, exclusion flow chart). A total of 28 standalone case reports and 4 case series containing a further 11 cases of synovial sarcoma of the larynx were included.
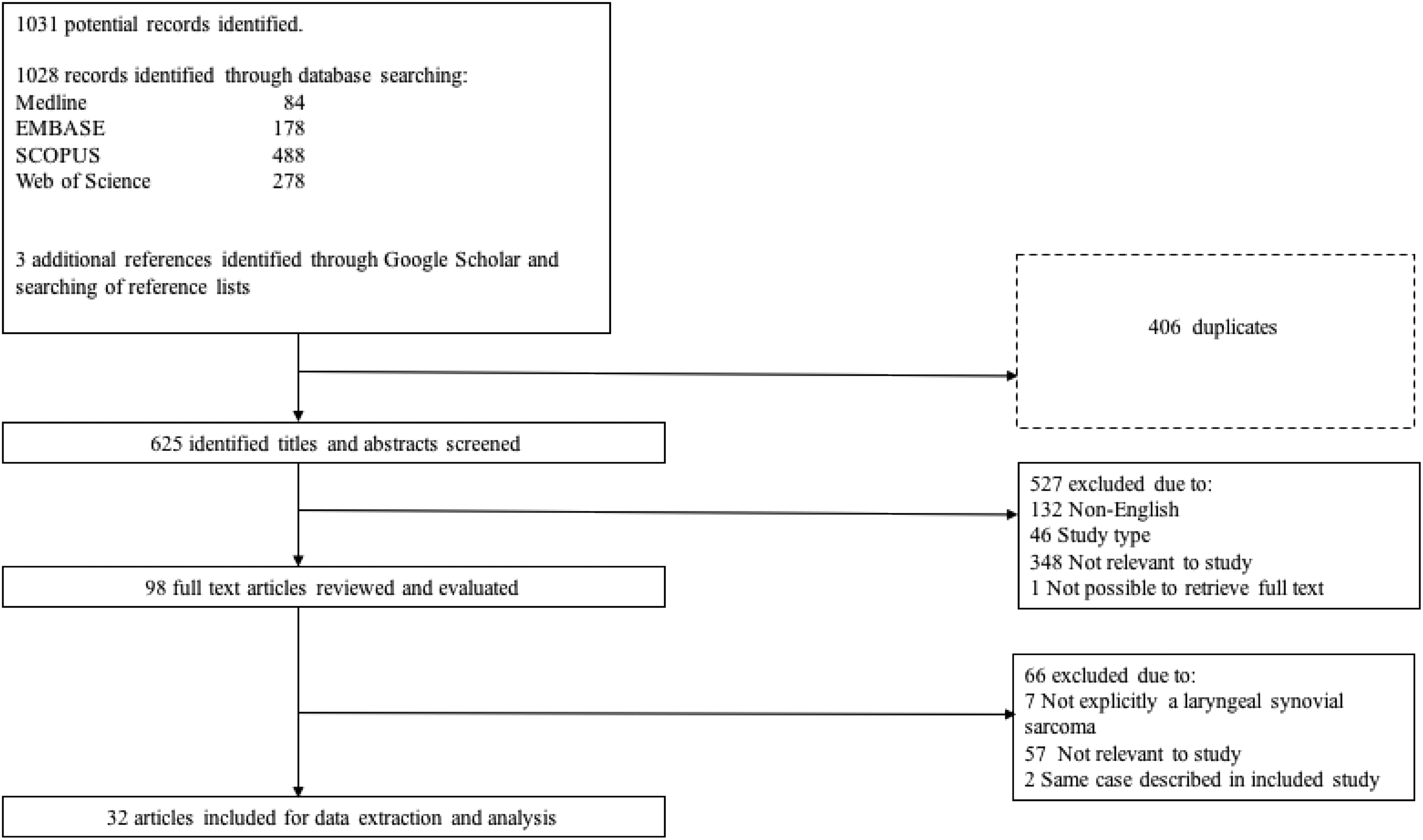
Flowchart of study selection process.
Description of Studies
A summary of the 32 contemporary and historical articles included in the review is presented in Tables 2 and 3, respectively. Data on a total of 39 cases of laryngeal synovial sarcoma were extracted from 32 articles reviewed. The mean age (range) at the time of diagnosis was 32 years (range: 11-79 years). Twenty-seven (69.2%) patients were male, while 12 were female. Studies from all continents were represented as follows: Europe (13), Asia and Middle East (11), Northern and Central America (6), Australia (1), Africa (1), and South America (0). Twenty-one (53.8%) cases arose from articles published after January 1, 2013.
Extracted Data from Contemporary Studies: 2013 to 2017.
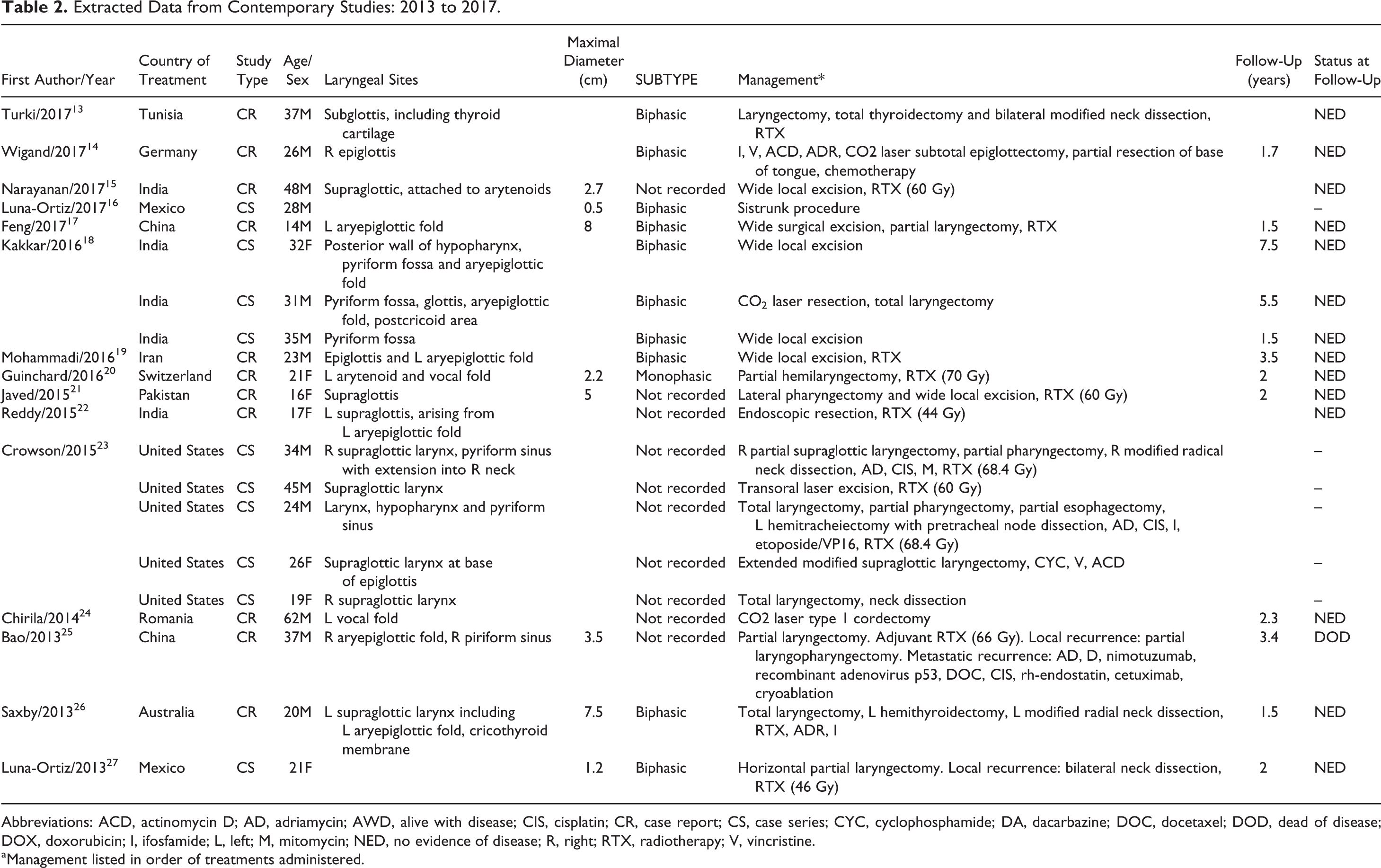
Abbreviations: ACD, actinomycin D; AD, adriamycin; AWD, alive with disease; CIS, cisplatin; CR, case report; CS, case series; CYC, cyclophosphamide; DA, dacarbazine; DOC, docetaxel; DOD, dead of disease; DOX, doxorubicin; I, ifosfamide; L, left; M, mitomycin; NED, no evidence of disease; R, right; RTX, radiotherapy; V, vincristine.
aManagement listed in order of treatments administered.
Extracted Data from Historical Studies: 1975 to 2012.
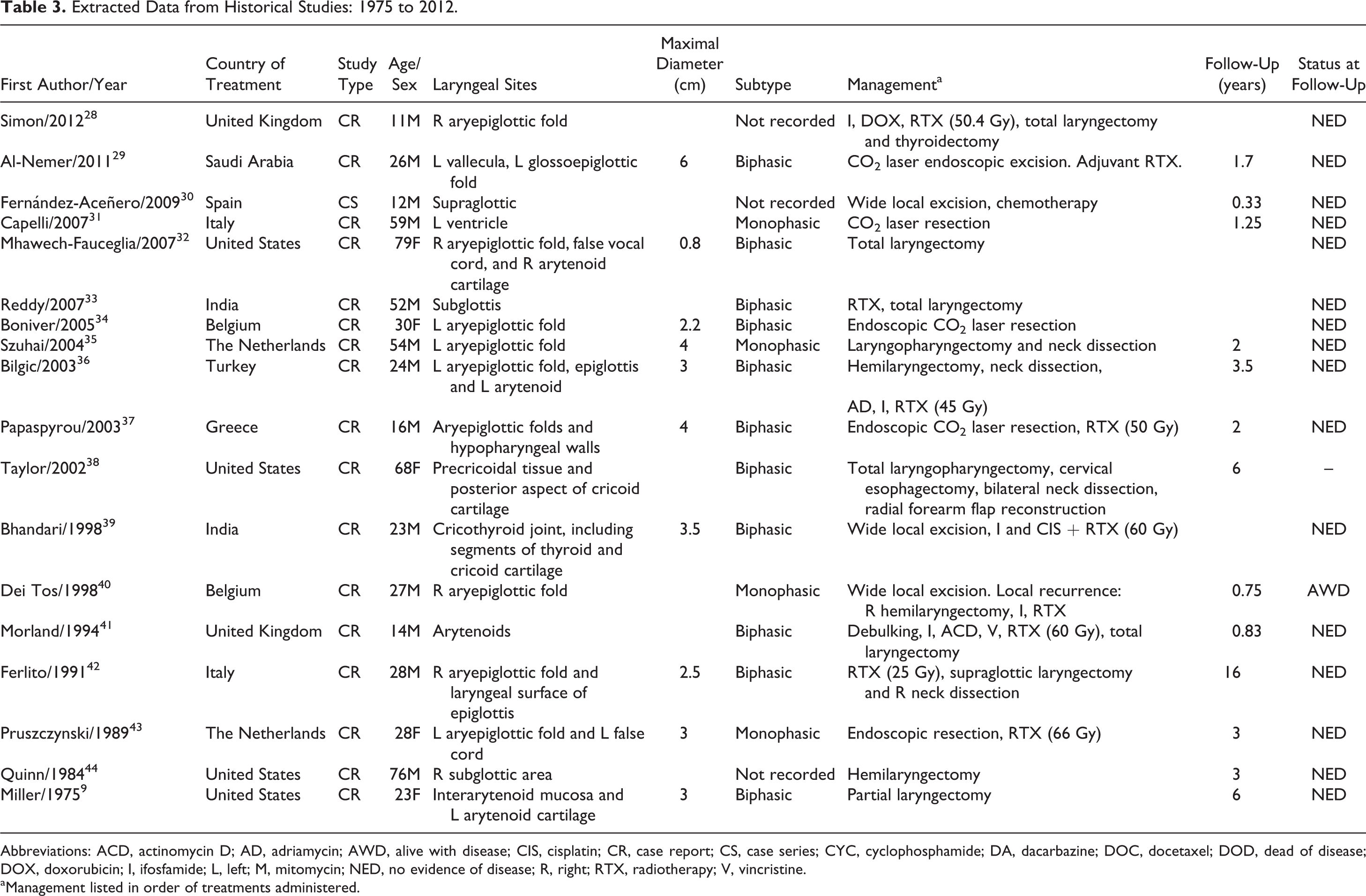
Abbreviations: ACD, actinomycin D; AD, adriamycin; AWD, alive with disease; CIS, cisplatin; CR, case report; CS, case series; CYC, cyclophosphamide; DA, dacarbazine; DOC, docetaxel; DOD, dead of disease; DOX, doxorubicin; I, ifosfamide; L, left; M, mitomycin; NED, no evidence of disease; R, right; RTX, radiotherapy; V, vincristine.
aManagement listed in order of treatments administered.
Tumor Characteristics
Synovial sarcomas arose predominantly from supralaryngeal structures (n = 28) including the aryepiglottic folds, arytenoids, and epiglottis (Table 2). In 4 cases, the tumor crossed the laryngeal ventricle to involve both the false and true vocal folds (transglottic). There were a further 4 cases arising from the subglottis and 1 case arising from the glottis. The subsite was not specified in 2 cases.
The mean maximal tumor dimension at the time of diagnosis was 3.8 cm (range: 0.5-8.0 cm). The histologic subtype of synovial sarcoma was reported in 26 cases, of which 80.7% (21/26) were biphasic morphology and the remaining 5 were monophasic spindle cell morphology. There were no reported cases of undifferentiated synovial sarcoma. Histological subtype was not available in 13 cases.
Pathological diagnosis was made predominantly by immunohistochemical studies, the results of which were variably presented in 21 cases. Expression of epithelial membrane antigen (EMA), CD99, and Bcl-2 were documented in 13 (92.8%) of 14, 14 (100%) of 14, and 7 (87.5%) of 8 specimens, respectively. Fifteen tested specimens showed diffuse staining for vimentin, while TLE-1 was positive in 2 of 2 cases. Nine of 10 tumors were S-100 negative, with 3 tumors reportedly CD34 negative. Since first being used in 2004 by Szuhai et al, 8 cases utilized either FISH or RT-PCR cytogenetic studies to identify the SYT-SSX fusion gene. In terms of staging, all but one case of synovial sarcoma of the larynx (n = 38) was localized to larynx at the time of diagnosis. There was 1 case of metastatic disease at diagnosis, and no cases of confined locoregional spread.
Treatment
Surgery was the principal modality of treatment for synovial sarcoma of the larynx. In all 39 cases, the patient underwent a surgical procedure to excise the tumor. In 8 patients, a CO2 laser was used to perform an endoscopic excision. Over half of the patients (n = 20) required a partial (n = 10) or complete laryngectomy (n = 10) as part of their initial surgery, with a further 2 patients requiring a total laryngectomy for positive margins or disease recurrence. A neck dissection was performed in 7 cases. Of the 32 cases reporting on margin status following initial surgery, clear margins were achieved in all but 2 cases. There were no significant differences in the surgical approaches and treatment regimens when comparing contemporary articles from the past 5 years (published after 2013) with those published prior to this period.
In addition to surgery, 21 patients received radiotherapy as part of their initial treatment regimen. Radiotherapy was given predominantly as adjuvant therapy (n = 18) rather than neoadjuvant therapy (n = 3). A mean of 56.6 Gy (range: 25-70 Gy) was administered to patients receiving radiotherapy. Chemotherapy was given in addition to radiotherapy in 7 cases.
Chemotherapy was incorporated into the treatment regimen for 10 patients, with 8 patients having adjuvant therapy and 2 patients having neoadjuvant therapy. In 3 cases, patients were treated with surgery and chemotherapy without radiotherapy (Table 4).
Synovial Sarcoma of the Larynx: Demographic and Pathogenic Characteristics and Treatment Regimens.a
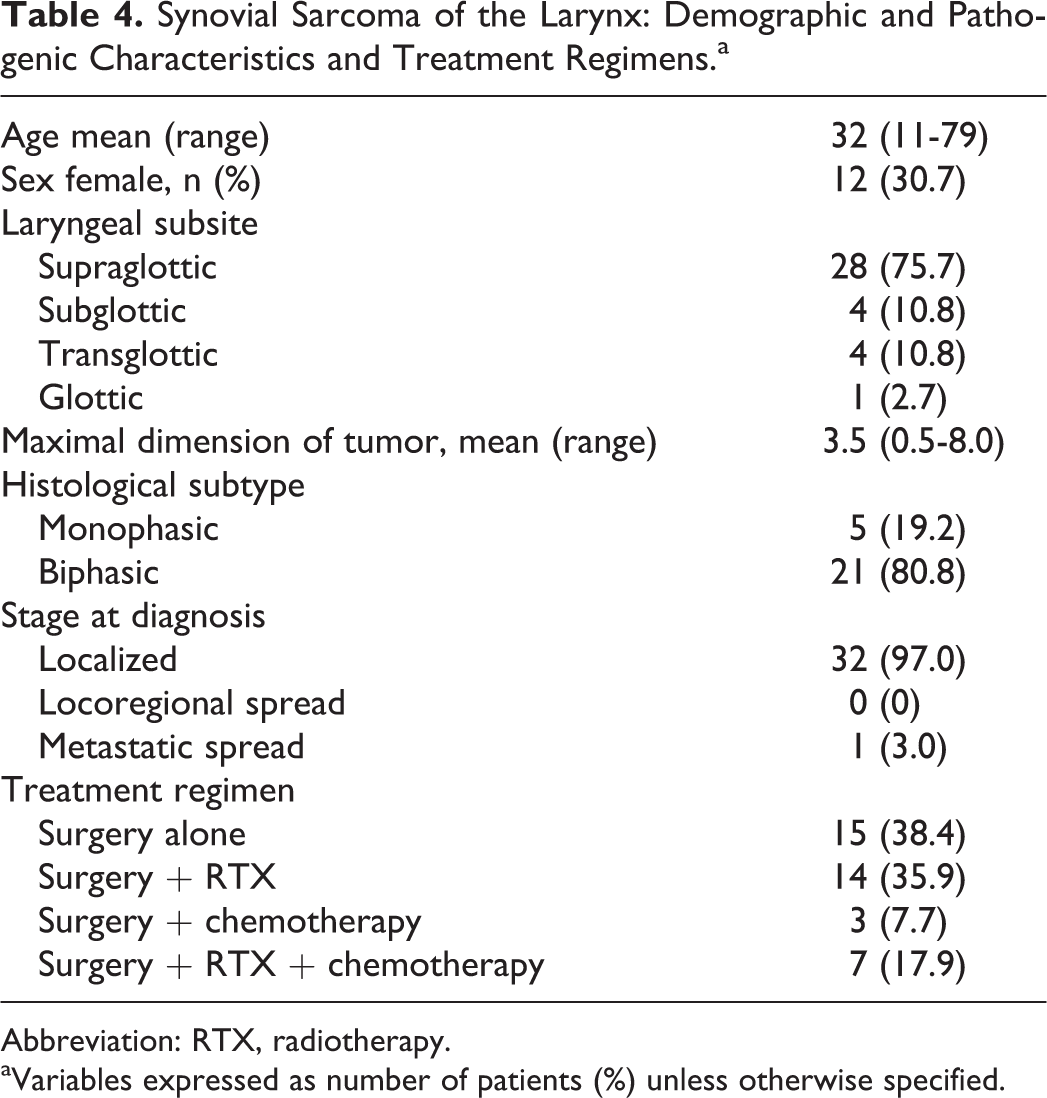
Abbreviation: RTX, radiotherapy.
aVariables expressed as number of patients (%) unless otherwise specified.
The most frequently used agents were ifosfamide (9 cases), adriamycin (6), cisplatin (4), actinomycin D (2), and vincristine (2). Dacarbazine, doxetaxel, rh-endostatin, and doxorubin were all reported to have been used in one case. There were no differences in the types of chemotherapeutic agents used and average doses between contemporary (published after 2013) and historical cases. Analysis of chemotherapy protocols and their change over time was not performed due to limited data. One case of advanced metastatic disease published in 2013 reported on the use of the immunotherapeutic agents nimotuzumab and cetuximab, both monoclonal antibodies against epidermal growth factor receptor. 25
Disease Recurrence
As shown in Table 5, disease recurrence was reported in 5 (12.8%) cases, with an average time to recurrence of 26.8 months (range: 3-60 months). In 4 of these cases, recurrence was locoregional. In 1 case, there was both locoregional recurrence and metastatic deposits in both lung and brain, while in another case, the patient developed metastatic disease in the lung alone. Surgical margins were clear after the initial surgical resection in 4 of these cases and not recorded in 1 case. In 4 of the 5 cases in which recurrence arose, the patient had originally presented with supraglottic disease.
Cases of Synovial Sarcoma of the Larynx With Recurrence.
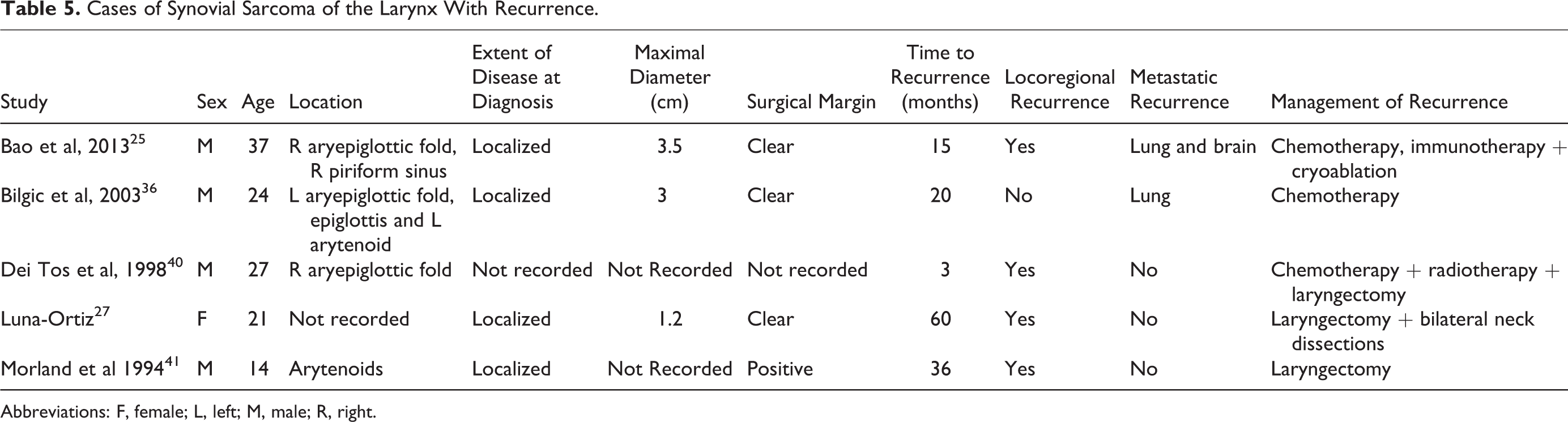
Abbreviations: F, female; L, left; M, male; R, right.
Follow-Up
The average follow-up period was 3.2 years (range: 0.3-16, years). At follow-up, 28 patients were alive and had no active disease, 1 patient was alive with active disease, and 1 patient had died from their disease. There was not sufficient and consistent recording of data with regard to postoperative or postradiotherapy complications.
Discussion
The literature demonstrates a clear lack of thorough and systematic reporting of cases of laryngeal synovial sarcoma worldwide. A total of 39 cases of laryngeal synovial sarcoma included and discussed here represent only a proportion of those reported, with 8 studies having to be excluded due to insufficient data. The 39 cases discussed had a mean age at diagnosis of 32 years (range, 11-79 years) and a male preponderance (69.2%), with 32 cases (82.1%) presenting before the age of 50 years. This was consistent with the general epidemiology of synovial sarcoma. Fisher reported an overall mean age of 26 years at the time of presentation for all synovial sarcomas, with a higher prevalence rate in males and 90% of cases occurring before the age of 50 years. 45
Diagnosis of synovial sarcoma remains challenging. This is because of the sheer number of differentials that may present and behave like synovial sarcoma. Within the head and neck region, cases of synovial sarcoma have been reportedly misdiagnosed in the first instance for a hemangiopericytoma, 8 branchial cleft cyst, 46 thyroid carcinoma, 47 and thyroglossal duct cyst. 48 In our review, immunohistochemistry remained the predominant method for establishing the diagnosis of synovial sarcoma of the larynx; however, it is recognized that detection of t(X;18) is much more diagnostic.
Imaging Studies
Scant information or documentation has been given with regard to imaging studies performed as part of the patient workup. In some case reports, clinicians relied solely on physical examination and chest and abdominal X-rays, whereas others used positron emission tomography/computed tomography for tumors of a similar size, grade, and stage. Although some of this may be explained by limitations in resources in different hospitals, it likely also stems from no clearly defined imaging guideline for the workup of laryngeal synovial sarcoma. The lack of preoperative staging may also be explained by the fact that in some of these cases the lesion was erroneously presumed to be benign. Additionally, magnetic resonance imaging (MRI) has been commonly purported as an option for preoperative planning, although there exist no specific radiological features of synovial sarcoma of the head and neck on MRI. 49 Distinguishing synovial sarcoma from other lesions of the larynx and other mesenchymal malignancies or spindle-cell sarcomas is vital for ensuring a proper therapeutic approach. The rate of misdiagnosis in synovial sarcoma of the head and neck and lack of concrete imaging findings and protocols are reflected in the heterogeneity of the cases presented here, and a need for greater certainly needs to be addressed.
Immunohistochemistry
Immunohistochemistry findings on laryngeal primaries were in keeping with those arising from more common anatomical sites. Cytokeratins, including 7 and 19, are helpful in distinguishing synovial sarcomas of the larynx from malignant peripheral nerve sheath tumors and were positive in 92.3% of cases. Focal expression of membranous marker EMA, vimentin, and Bcl-2 was similarly greater than 90% in keeping with previously reported studies. 10 The use of the more recently developed and more specific marker for synovial sarcoma, TLE-1, 50 was only reported in 2 recent cases. 17,37
Grading
Although some authors suggest grade as the clinicopathogenic factor most relevant to prognosis, 51 no formal grading was provided in the included studies. Current grading of synovial sarcoma is performed as for all other soft tissue tumors and follows the French Federation of Comprehensive Cancer Centers system, taking into consideration the degree of differentiation, mitotic count, and presence of necrosis. 52 The apparent lack of emphasis placed by clinicians on grade may be attributable to there being no specific histological grading system for synovial sarcoma. To that end, the development of a standardized and comprehensive grading system is vital to guiding further clinical management and prognostic information.
Tumor Size
The prognostic implications of tumor size at the time of diagnosis are unsettled. In a recent study of 93 patients with head and neck synovial sarcoma by Wushou and Miao, 53 tumor size >5.0 cm in diameter was associated with worse overall survival rates. Tumor size also correlated with local recurrence and metastasis. Similarly, a study of 111 patients with synovial sarcoma of all locations by Stanelle et al found strong correlation between tumor size and overall survival. 54 However, in a retrospective review of 150 adult patients without restriction for tumor location by Spillane et al, tumor ≥5.0 cm was not an independent predictor of survival. 55 In our series, there were 14 cases of tumors of maximal dimension <5 cm and 4 tumors ≥5 cm at the time of diagnosis. The one death and both cases of metastatic recurrence occurred in patients with a primary mass <5 cm in maximal dimension.
Histological and Fusion Gene Subtypes
The majority of cases of synovial sarcoma of the larynx were biphasic. The significance of this for prognosis is unclear. 1 In spite of its pathognomonic fusion gene, less than a quarter of all studies utilized FISH or RT-PCR cytogenetic testing to confirm the diagnosis. It is uncertain whether the absence of confirmatory molecular testing is due to a clear-cut diagnosis being made on histological and immunohistochemical studies, a lack of access to molecular testing centers, or simply an absence of documentation within the reported cases. The prognostic value of fusion type also remains unsettled. 56 In their study of 45 cases of histologically confirmed synovial sarcomas from all anatomical sites, Kawai et al found SYT-SSX2 fusion transcript was correlated with a significantly better metastasis-free survival. 57 However, a more recent retrospective review of 108 cases of synovial sarcoma found SYT-SSX fusion type is not a significant prognostic factor for patients with localized synovial sarcoma. 51 Greater use of FISH and RT-PCR may reduce the incidence of delayed diagnosis or misdiagnosis and should be used routinely, particularly when diagnosis cannot be confidently established with other techniques. 58 More widespread use may also allow for more accurate prognostication based on the SYT-SSX fusion gene subtype.
Stage at Diagnosis
Patient management for synovial sarcoma depends mostly on the stage of the disease. Unfortunately, reporting of investigations performed to stage the disease and formal staging using the American Joint Committee on Cancer/International Union against Cancer tumor–node–metastasis was poor. Only one case of laryngeal synovial sarcoma exhibited metastatic spread at the time of diagnosis, with no cases of confirmed cervical lymph node involvement. This compares with a rate of 47% of synchronous metastasis at presentation with upper and lower limb synovial sarcoma as reported by Billingsley et al at other sites. 59 This may be attributed to earlier onset of concerning symptoms prompting earlier patient presentation compared with primary tumors at more peripheral locations. Whether the location of the primary synovial sarcoma site affects hematogenous spread and the establishment of metastatic disease is similarly unclear.
Surgical Management
Initial management of localized laryngeal synovial sarcoma is predicated on wide local excision of the tumor. To that extent, localized disease is managed similarly to synovial sarcomas arising in other head and neck sites and the extremities. The importance of clear surgical margins for synovial sarcoma is well established. In spite of the challenge of achieving clear margins for head and neck primaries, only 2 cases 9,59 (6.2%) of laryngeal primary disease had a positive margin following initial definitive surgical resection. This compares favorably with the rates of positive margins recorded in other head and neck sarcoma studies: Breakey et al (12%), 60 Kraus et al (42%), 61 Colville et al (31%) 62 , and Le Vay et al (27%). 63 A possible reason for the low rates of positive margins for resected laryngeal synovial sarcoma is the early onset of concerning symptoms such as dysphonia that cause patients to present early with small localized disease.
It is generally recommended that neck dissection be performed only in the setting of confirmed cervical lymph node involvement with no role for prophylactic lymph node removal. Nevertheless, 7 patients from the studied articles underwent a neck dissection. In all 7 cases, no metastatic deposits in the lymph node were evident on histopathology. This again demonstrates a lack of consistent practice in managing this rare disease.
Role of Radiotherapy
The role of radiotherapy in treating laryngeal synovial sarcoma is contentious. Traditionally, head and neck sarcoma resections have been associated with high rates of positive margins following surgery. The proximity of head and neck sarcomas to vital vascular structures and nerves within the neck has tended to compromise their complete surgical excision. Radiotherapy has thus been used as an adjunct to surgery to achieve locoregional disease control. In their review of head and neck synovial sarcomas, Harb et al 64 found radiotherapy to be associated with lower recurrence rates and higher survival, although the results did not achieve significance.
Extremely high rates of clear margins following primary surgical excision were reported in this review. Moreover, all but one case had localized disease at the time of surgery. These findings, coupled with the significant potential morbidity associated with radiotherapy, would suggest radiotherapy should be used judiciously. However, few studies reported on the length of the closest clear margin, and thus, the true rate of clear wide margins achieved is likely to have been lower. In addition, the relatively high rate of recurrence of 12.8% (5/39) at follow-up may also persuade clinicians to administer radiotherapy to increase the probability of achieving disease control. In this review, 21 (53.4%) patients had radiotherapy as part of their initial treatment regimen. The mean dose of 56.6 Gy administered for laryngeal primary disease falls within the range of 50 to 70 Gy typically used for head and neck synovial sarcoma adjuvant radiotherapy. Due to the small sample size, we were unable to establish differences in overall survival and recurrence rates between the group of patients who had standalone surgery (n = 15) and the group who had surgery with radiotherapy (n = 14). More research is required to determine the exact role of radiotherapy in laryngeal synovial sarcoma treatment following clear margin resections.
Role of Chemotherapy
There is a lack of consensus concerning the roles of chemotherapy in managing synovial sarcoma. Although early studies suggested it conferred no benefit, 65 Santoro et al 66 found improvements in disease-free and overall survival with ifosfamide and doxorubicin. Similarly, the Sarcoma Meta-Analysis Collaboration found adjuvant chemotherapy for localized resectable soft tissue sarcoma of adults improved time to local recurrence and distant recurrence and overall recurrence-free survival. 67 For head and neck synovial sarcomas, Harb et al recommend neoadjuvant chemotherapy for all patients with tumor size >5 cm, local extension of tumor, or if a lesion is in a high-risk surgical site. 64 There were 3 cases of neoadjuvant chemotherapy in our study, with Harb et al’s criteria only met in one of these cases. In our review, we were unable to establish further benefit in the addition of chemotherapy to a combined surgery and radiotherapy regimen.
Recurrence
There are 5 reported cases of recurrence. The epidemiological characteristics of the 5 recurrences compared to the 34 cases with no recurrence at follow-up are much the same, with the average age of those with recurrence being 25.4 years at the time of diagnosis. Furthermore, those who developed recurrent disease, the average tumor maximal size was 2.6 cm compared with 3.9 cm for the nonrecurrent group. The average time of recurrence was 26.8 months after initial treatment. Two of the 5 recurrences were metastatic and that to the lung and brain, being consistent with sites of metastasis of synovial sarcomas in general. Furthermore, there was no difference in anatomical site of those patients with and without recurrence, with the majority of disease occurring in the supraglottic area. More data are required to determine the disease- and patient-related factors that predispose patients with synovial sarcoma to developing disease recurrence.
Multidisciplinary Approach
In order to optimize overall treatment outcomes, a multidisciplinary, patient-centered approach to the management of synovial sarcoma of the larynx must be adopted. In spite of their importance, few cases were reported on the specialist care delivered by allied health services including speech pathology, physiotherapy, and psychology. Laryngectomy and the consequent laryngeal dysfunction may be associated with reduced quality of life and overall emotional well-being. For the young patients affected by synovial sarcoma of the larynx, this impact is likely to be even greater. Providing comprehensive airway rehabilitation and psychological support for these patients is essential. 28
Limitations
There are a number of limitations to performing a systematic review on a rare condition such as synovial sarcoma of the larynx. This review relies on relatively low-grade evidence in the form of case reports and case series. Several articles did not record key data variables, limiting the power of the study and the robustness of its conclusions. The exclusion of non-English articles may have also affected the overall findings in this systematic review. However, given that only 6 relevant articles written in a language other than English were excluded, 68 -73 the overall effect of this exclusion criterion is likely to have been small.
Conclusion
This is the first systematic review of synovial sarcoma of the larynx reported in the literature. Overall demographic and clinicopathogenic data for synovial sarcoma of the larynx are consistent with the findings of studies from more common sites of disease. There are still several aspects of synovial sarcoma that are poorly understood. The role of imaging, what implications tumor size, histological subtype, and SYT-SSX fusion gene subtype have on prognosis, among other factors, still remain unclear. A large reason for the lack of understanding is the scant recording and analysis of these cases.
To meaningfully advance our understanding of synovial sarcoma of the larynx as a disease entity, we propose that a readily accessible database of all cases be established. We also advocate for the establishment of evidence-based guidelines to ensure patients receive timely diagnosis, optimal treatment, and avoid unnecessary morbidity.
Footnotes
Acknowledgments
Monica O’Brien, Academic Services Librarian at the University of New South Wales, assisted with the development of the database search strategy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.