
Abstract
Clinically, atrophic rhinitis (AR) is well recognized. We present the case of a patient diagnosed with AR. Sphingomonas paucimobilis, an uncommon bacterial pathogen, has been isolated in nasal cultures. This study discusses the microorganisms, causing AR. According to previous research, these infections have been associated with significant morbidity and mortality. Due to the limited knowledge on the disease, the diagnosis is frequently delayed. Thus, frequent monitoring and treatment are needed to avoid complications. This rare type of infection should be suspected in patients presenting with nasal blockage, including those from non-endemic areas.
Introduction
Atrophic rhinitis (AR) or coryza foetida is a chronic condition. It is classified into primary and secondary AR, depending on the underlying etiology. The diagnosis of AR is based on the clinical symptoms of the patient, and it is confirmed via computed tomography (CT) and microbiological findings. 1
Atrophic rhinitis has various clinical presentations. In a study by Moore et al., 2 all 242 patients, included in the study, complained of bilateral nasal congestion and daily nasal crusting. In addition, only 48% and 33% of the patients complained of facial pressure and intermittent epistaxis, respectively. Similar findings were observed in another study by Bist et al. 3 all 90 patients included in their study experienced nasal crusting. Nasal factors and purulent discharge were reported by 86.6% of patients, while only 66.6% had nasal obstruction. Other symptoms included anosmia, epistaxis, nasal pain, sleep disruption, and choking due to aspiration of the crusts. Based on the nasal findings, nasal crusts, nasal mucosa dryness, enlarged nasal cavities, and atrophy of the inferior turbinate were the most common findings in individuals with AR. Nasal septal perforation and secondary saddle nose deformity occurred in a small percentage of patients.
The typical CT findings include some degree of sinusitis, nasal mucosal atrophy, bone resorption, and widened cavities.2-4 Although benign, AR results in significant morbidity due to the development of bony erosions, extending to the orbits and intracranial areas. According to the microbiological findings in previous reports, Pseudomonas aeruginosa and Klebsiella spp. were the most frequently cultured organisms, accounting for 37% and 31% of cases, respectively. Other common pathogens include Staphylococcus aureus, Proteus mirabilis, and Escherichia coli.2-4 Based on the review of literature, Sphingomonas paucimobilis has not been isolated in nasal samples.
Case Report
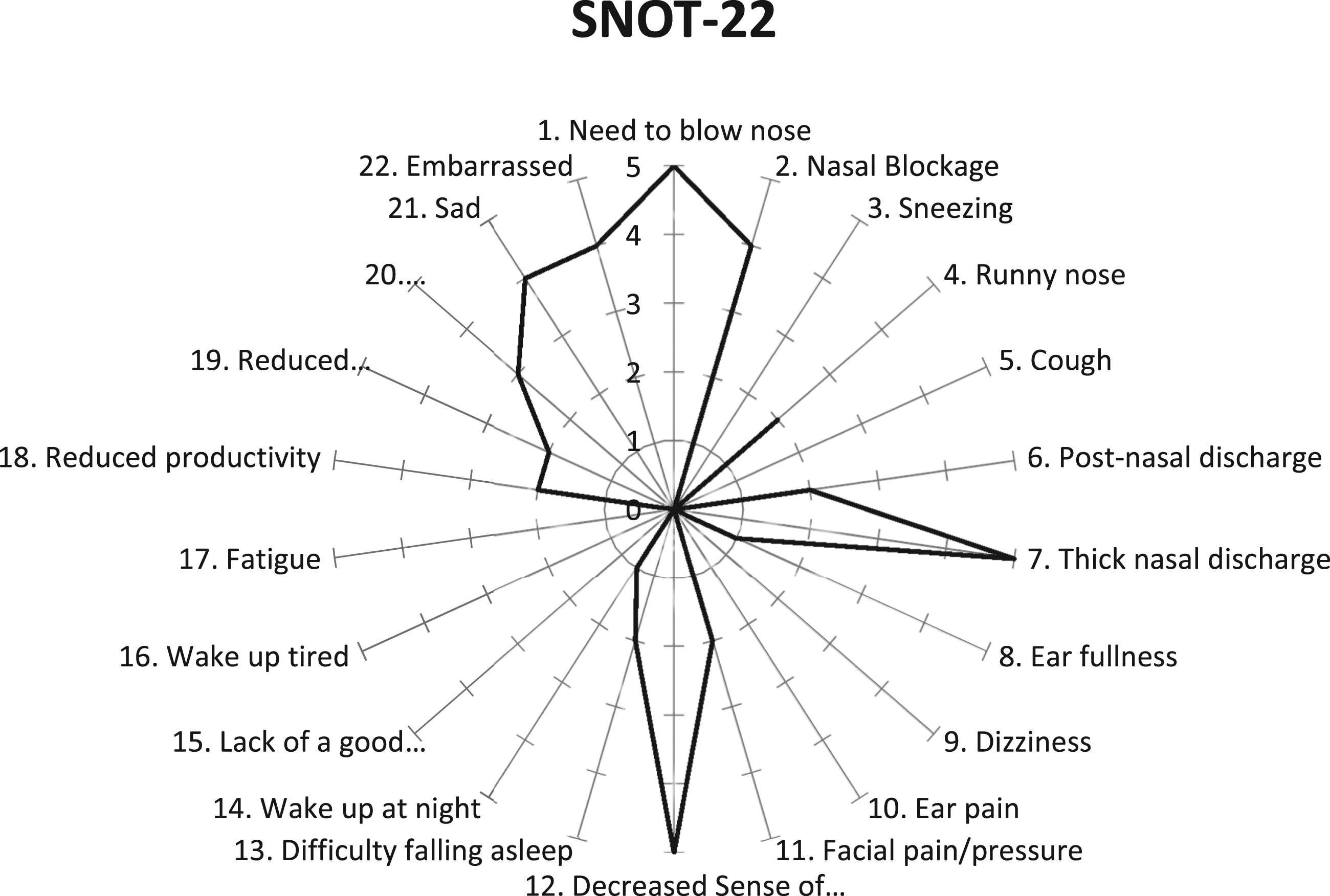
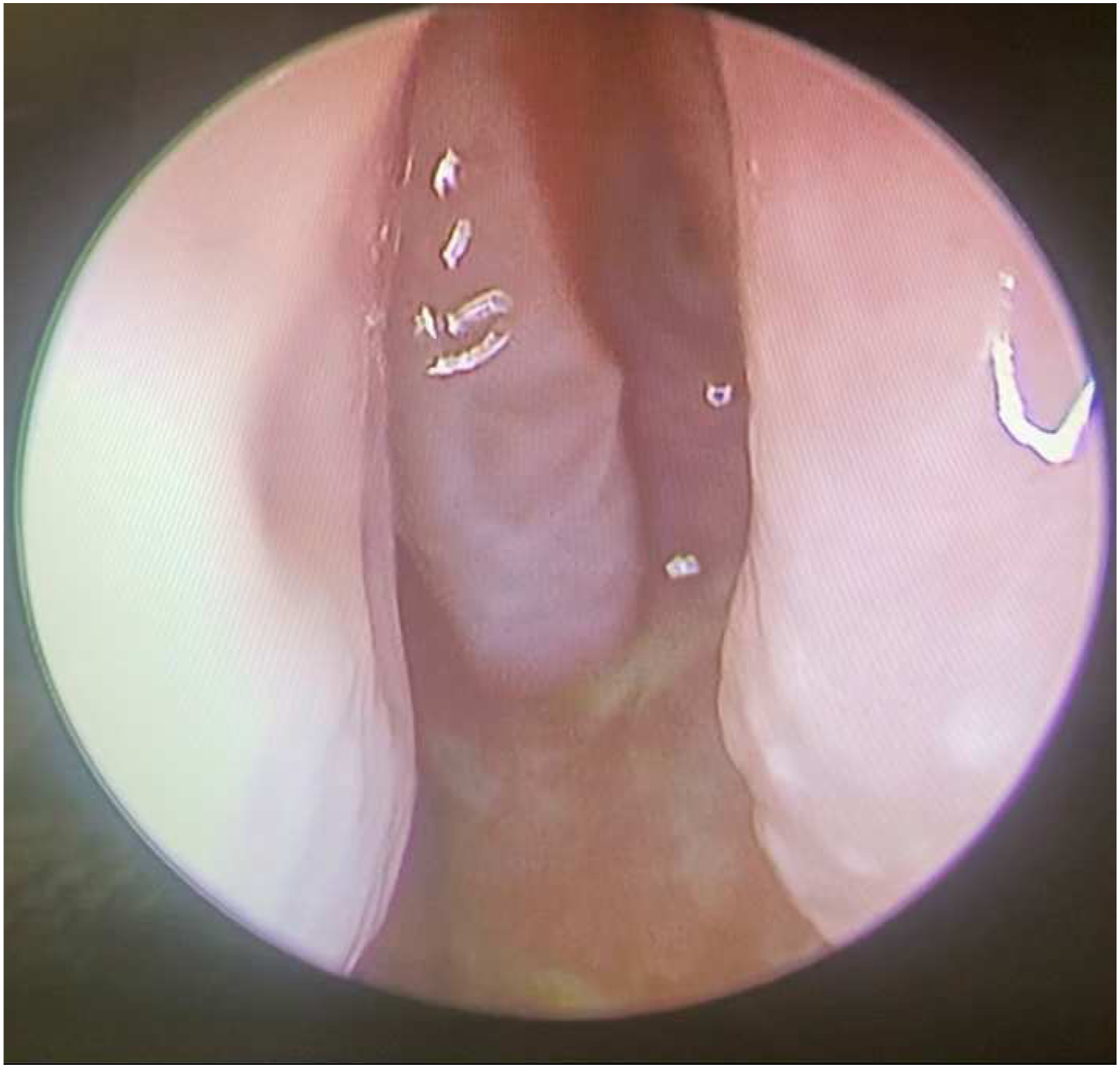
A 36-year-old woman presented to the clinic with bilateral nasal obstruction, thick nasal discharge, and postnasal drip. Nasal endoscopic examination revealed an atrophied mucosa, thick greenish discharge, crusting, and a deviated nasal septum to the left side. CT (Figure 1A and B) of the paranasal sinus showed mucosal thickening of the left and right ethmoid air cells and right maxillary sinus. The left and right maxillary ostia were patent. The patient also had a left deviated nasal septum and a thickened nasal mucosa. A swab was obtained from the discharge. The culture and sensitivity testing revealed significant growth of Sphinogomonas paucimoblis. Based on the Sinonasal Outcome test-22 (Figure 2), the patient had a grade of 44/110. His most prominent symptoms included nasal blockage, thick discharge, and anosmia. The patient reported no other positive findings Figure 3, including changes in smell or facial pressure. The patient was managed with regular nasal irrigation, ofloxacin (.3%), and dexamethasone (.1% drip). A. Coronal CT (bone view) showing deviated nasal septum, mucosa atrophy, and turbinates atrophy. B. Axial CT (soft tissue view) showing deviated nasal septum and mucosa atrophy. SNOT-22 score upon presentation. The patient scored 44/110 for the 22 items, on a 0–5 scale per item as reported by the patient. Nasal endoscopy was done post-management shows both clinically and endoscopically improvement.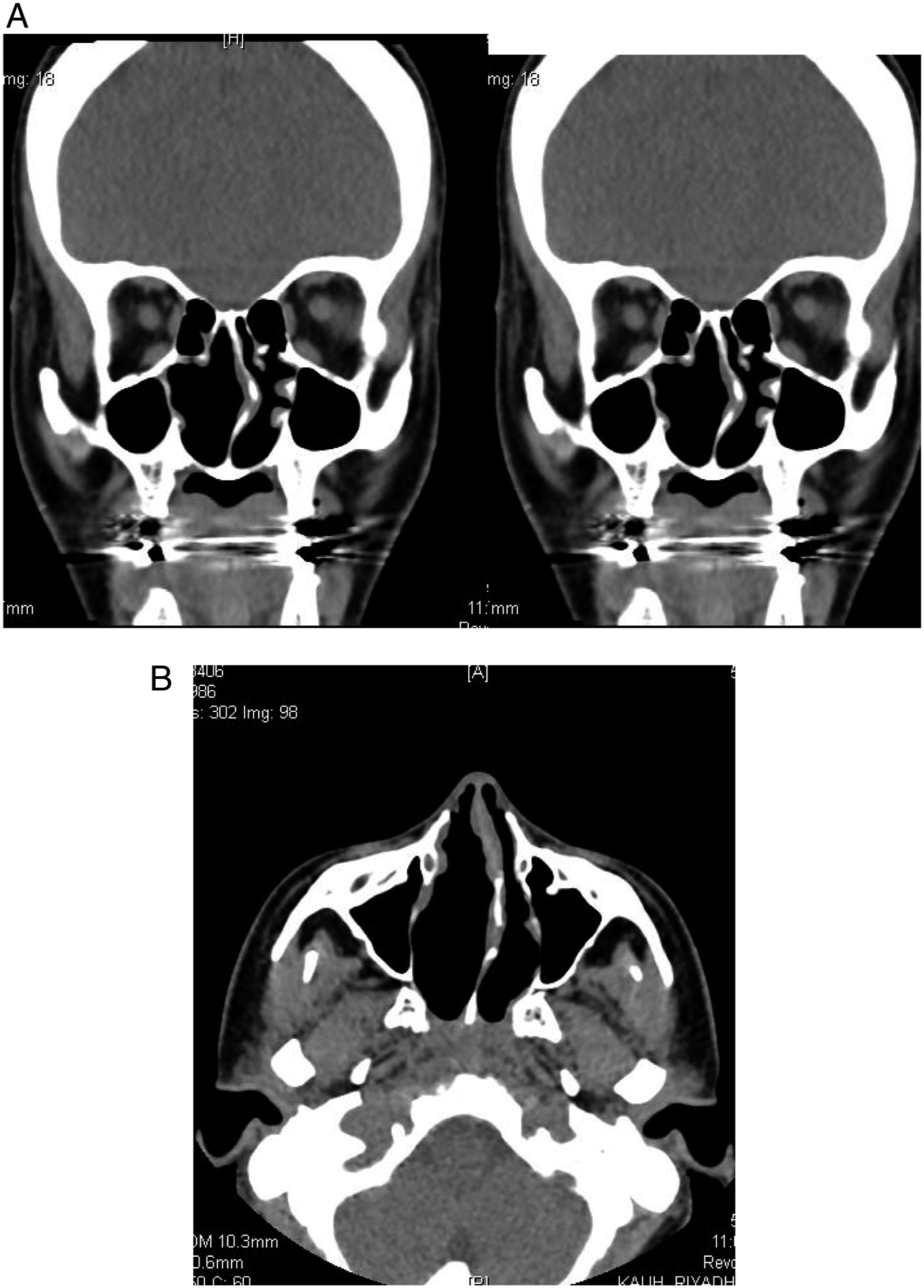
Discussion
Atrophic rhinitis is characterized by a triad of symptoms, consisting of nasal mucosa atrophy, paradoxical nasal congestion with widened nasal cavities, and ozaena (foul odor or nasal secretions). These symptoms were attributed to increased secretions and crust formation.5,6
Primary AR is prevalent in southern Saudi Arabia, China, Africa, India, the Mediterranean region, and the Philippines. 1 It is idiopathic and has been associated with mucosal colonization, predominantly Klebsiella ozaenae. 1 With the introduction of antibiotics in the last century and their application in the treatment of chronic nasal infections, the incidence of primary AR has significantly decreased. The reported prevalence of primary AR ranges from .3% to 1% in countries with a high prevalence. 7 Multiple causes, including granulomatous disease, nasal trauma, nasal surgery (empty nose syndrome), and radiation, have been identified for secondary AR. 2 In our case, primary AR was caused by an atypical bacterium, Sphinogomonas paucimoblis. It is an opportunistic Gram-negative bacillus, commonly detected in patients with nosocomial infections. It is uncommon in the clinical setting. According to a case study by Hardjo, 8 it typically affects immunocompromised patients, including those with diabetes mellitus and a history of steroid use. This organism is most commonly found in intensive care and highly dependent units. 9 The management of primary AR involves conservative treatment. Medications are locally or systemically. Nasal irrigation and douches were recommended. 10 Previous studies have recommended the application of topical gentamycin and a systemic (intravenous) aminoglycoside (tobramycin) for 2 weeks to treat patients infected with Klebsiella. Favorable outcomes were also achieved in patients treated with rifampicin (600 mg once daily for 12 weeks). 7 Ciprofloxacin (500-750 mg twice daily for 1 to 3 months) was also effective in alleviating symptoms of crust formation and olfactory changes in patients infected with K. ozaenae. 7 The study had several limitations. First, the likelihood of a false-positive result for this organism was not considered. Second, there is insufficient data on this research topic, so the study findings cannot be generalized.
This article reported a case of AR in a patient, whose culture was positive for S. paucimobilis. The patient was successfully managed with conservative treatment, consisting of topical antibiotics and nasal irrigation. This organism has been rarely reported in AR cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from King Saud University Institutional Review Board
Informed consent
Written informed consent was obtained from the patients for the anonymized information to be published in this article.