
Abstract
Keywords
Introduction
Atrophic rhinitis (AR) results in a large emptiness of the nasal cavity, due to atrophy of the nasal mucosa covered with malodorous crusts. 1 Two types of atrophic rhinitis can be described; one primary (ozene) is currently rarely used, the other secondary (radiotherapy, surgery, etc) is more common. Ozene is a primary atrophic rhinitis; it is a rare chronic degenerative disease of the nasal cavity. 2 Its pathophysiology is poorly understood. Its diagnosis is essentially clinical. The isolation of Klebsiella ozaenae strengthens the diagnosis. 3 Its management is delicate, often medical, and sometimes surgical.
The aim of our work is to analyze the epidemiological, clinical, and therapeutic aspects of this condition.
Methods
We report 4 observations of primary atrophic rhinitis, collected in the ENT and head and neck surgery department of the Habib Bourguiba University Hospital in Sfax over a period of 5 years (from 2018 to 2022).
The diagnosis of atrophic rhinitis was based on the recommendation of the French ENT society 1 : atrophic rhinitis was defined by a sensation of nasal obstruction associated with the presence of numerous crusts and a feeling of dry nose. Olfactory disorders such as cacosmia or even anosmia are not rare.
We have obtained the consent of the 4 patients for the publication of this work.
Results
All patients were female, with an average age of 32 years (between 6 and 64 years).
The revealing clinical signs are cacosmia and purulent rhinorrhea (all patients), the sensation of intermittent nasal obstruction is reported by 3 patients; epistaxis by 2 patients and anosmia by a single patient.
Rhinoscopic examination found mucosal atrophy with crusts in all cases (Figure 1).
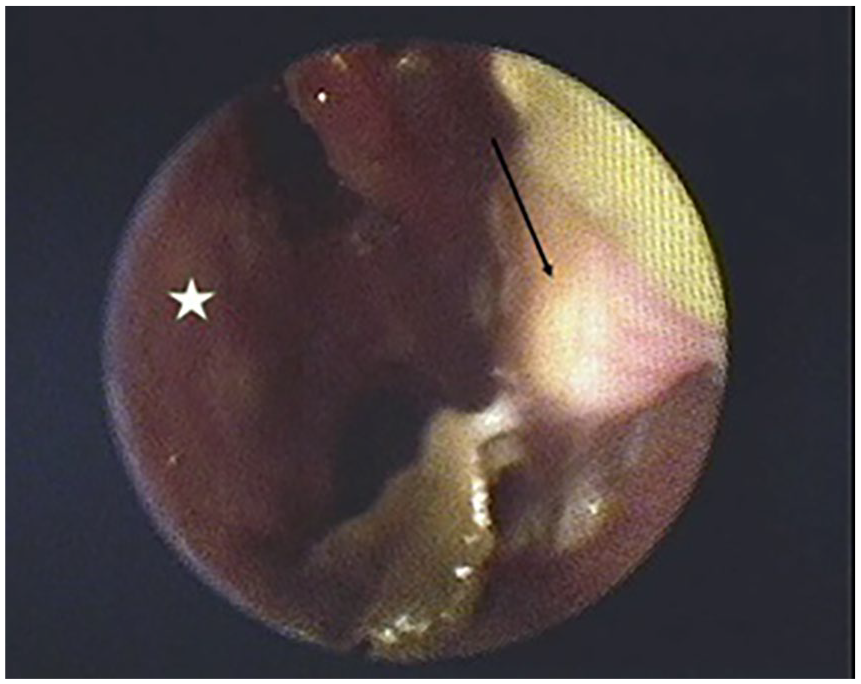
Endoscopic appearance of the left nasal cavity before treatment (Patient No. 1): Inferior turbinate: arrow, nasal septum: star.
All patients had wide nasal passages with purulent rhinorrhea; only one case of dacryocystitis was noted.
A local bacteriological sample was taken from all patients, concluding that Klebsiella pneumoniae ozaenae was present in all cases.
Three patients had a computed tomography (CT) scan of the facial area showing a very atrophic nasal mucosa without bone lysis or specific filling (Figure 2).
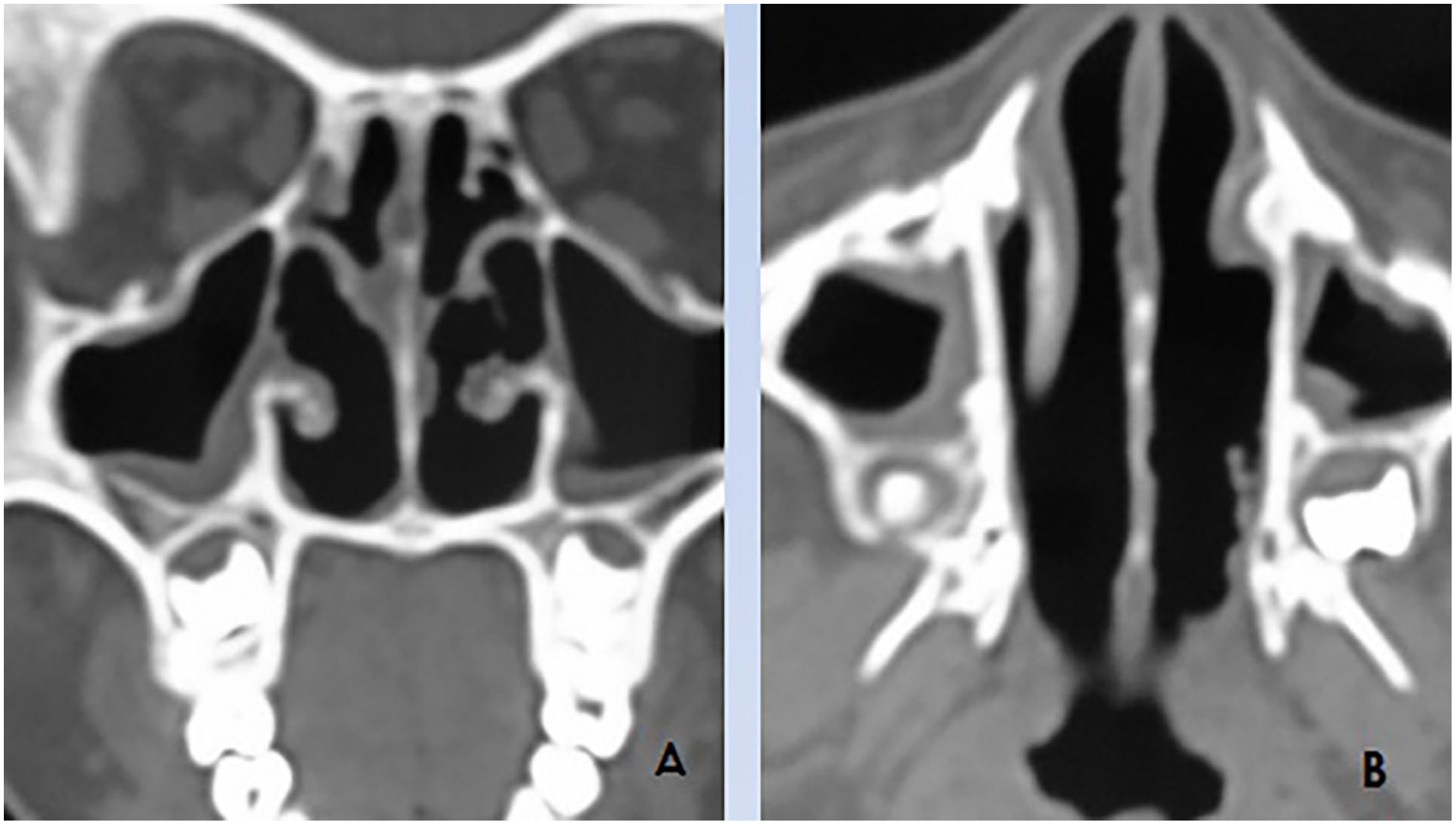
Scan of the facial area without injection in a bone window; (A) coronal reconstruction; (B) axial section.
The treatment was medical in 3 patients and surgical in 1 patient:
Medical treatment consisted of oral antibiotic therapy based on rifampicin and sulfamethoxazole and trimethoprim for a period of 4 months, associated with frequent nasal washing.
Surgical treatment was indicated for a patient by carrying out a recalibration of the nasal cavities by placing 2 silicone sticks subperiosteally.
The evolution was marked by the improvement of nasal obstruction, and the disappearance of cacosmia in 75% cases (Figure 3).
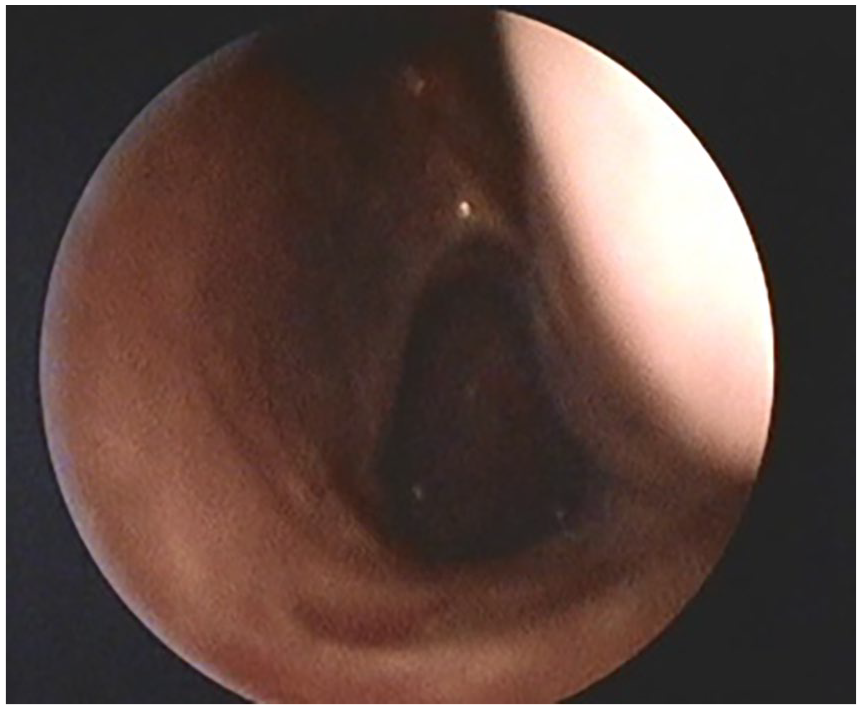
Endoscopic appearance 3 months after medical treatment (Patient No. 1).
Discussion
Atrophic rhinitis or ozene is a disease that is still common in developing countries due to poor hygiene and socioeconomic levels. It is widespread in China, Africa, India, the Philippines, and the Mediterranean region. 2 With the introduction of antibiotics in the treatment of chronic nasal infections, the incidence of AR has decreased significantly. The reported prevalence of primary AR ranges from 0.3% to 1% in high prevalence countries. 3 The female predominance has been noted by several authors. 3
Its etiopathogenesis is not yet well known; several factors have been described such as hereditary, nutritional, anatomical, endocrine, neurovascular, immune, and infectious factors.2-5
The diagnosis of atrophic rhinitis is clinical and bacteriological; the clinic is characterized by a triad: mucosal atrophy, the presence of crusts, and cacosmia.6,7 Bacteriological examination isolates K. ozaenae in most cases. 8
The CT scan of the facial mass provides diagnostic guidance by showing atrophy of the mucosa of the middle and lower turbinates, bone resorption, enlargement of the nasal cavities, and sometimes hypoplasia of the maxillary sinus. 9
The goal of treatment is to restore nasal hydration and minimize crusting. 10 It is essentially medical based on nasal washing (saline solution, sodium bicarbonate, or a mixture) to prevent crust formation. 11 Irrigation of both nostrils should be done with a 10 to 20 cc syringe or any other nasal irrigation device 3 to 4 times a day. Nasal dryness can be reduced by the application of anti-evaporation compounds such as glycerin, mineral oil, or menthol.3,12
Based on the theory that atrophic rhinitis is of infectious origin, some authors indicate the use of gentamycin locally with the aim of eliminating the colonization of bacteria. 3 Several authors recommend the use of systemic antibiotics to eradicate K. ozaenae; the antibiotics used are ciprofloxacin, rifampicin, and trimethoprim-sulfamethoxazole.3,13 The recommended duration of treatment is 2 to 3 months. 3 Other adjuvant treatments have been tried such as vitamin A, iron, potassium iodide, and estrogen with encouraging results. 3 In our study, we used rifampicin and trimethoprim-sulfamethoxazole as antibiotics for a period of 4 months with good results.
Many materials have been used for nasal submucosal injection to treat patients with AR. A study using autologous fat and platelet-rich plasma injected into the inferior and middle turbinate, septum, and nasal floor showed significant improvement. 14
Surgical treatment has been tried for years with varying results. Recalibration surgery by placing a subperiosteal graft in the floor prevents the drying effects of ambient air. 15 The material used can be silicon, silastic, acrylic, Teflon, or hydroxyapatite. Recalibration surgery was performed using silicone in only one patient without satisfactory results. However, the use of autologous materials is preferable to silicone due to the risk of migration and extrusion of the latter and the need for prolonged monitoring. 15
Conclusion
Ozene or primary atrophic rhinitis is a disease that is still common in developing countries. It is characterized by a triad made up of: nasal cavity gaping, the presence of crusts, and cacosmia. The presence of a specific germ (K. ozaenae) is important to establish the diagnosis. Medical treatment with antibiotics may be sufficient to improve the symptoms.
Footnotes
Acknowledgements
I thank the bacteriology team of the Habib Bourguiba Hospital in Sfax.
Declaration of Availability of Data
I declare that all the data in the medical file are available.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Declaration
This work did not require acceptance from the ethics committee.
Informed Consent/Patient Consent
Taken, form provided.
Trial Registration Number/Date
This is not a therapeutic trial.