
Abstract
Introduction
Atrophic rhinitis (AR) is a chronic degenerative nasal disease characterized by a triad of symptoms and signs, including progressive atrophy of the nasal mucosa, the formation of the nasal crust, and a distinctive offensive odor. 1 AR is occasionally referred to as acute necrotizing rhinitis, rhinitis atrophicans, atrophic catarrh, coryza foetida, or rhinitis in a representative fetus (ozaena). AR is classified into primary and secondary types. Primary AR presents with spontaneous onset and progresses slowly with time. In contrast, the secondary type presents underlying causes such as nasal surgery, radiation therapy, and granulomatous disease. 2
Previous articles have separately described the etiology, pathogenesis, and treatment of AR without much emphasis on the impact of AR on patient quality of life. Furthermore, recent advances in AR diagnostics and management strategies have not been reported comprehensively to help clinicians make the appropriate treatment decisions. Therefore, this article reviewed the pathogenesis, types, diagnostics, and new treatment modalities of AR and its impact on quality of life.
Materials and Methods
A comprehensive literature search was conducted using PubMed, Web of Science, Google Scholar, and Saudi Digital Library databases. The articles were examined to extract information on the pathogenesis, types, new treatment modalities of AR, and its impact on lifestyle.
Primary AR
Primary AR, also known as ozaena, is an age-old disease first described by Fraenkel in the late 19th century. The condition is characterized by a sclerotic change in the mucous membrane, abnormal patency of the nasal passages due to atrophic changes in the mucosa and underlying bones, and thick viscous secretions that emit a foul odor when dry. 3 It affects all parts of the nasal cavity while rhinitis sicca affects only the anterior and caudal parts of the nasal cavity. 4
Etiology of primary AR
Several theories have been proposed to explain the etiological factors that can contribute to the development of primary AR. These include heredity factors 4 , infections, and infectious agents,5,6 developmental disorders, 7 nutritional deficiencies, 5 phospholipid deficiency, 8 autonomic disorders,5,9 endocrine imbalances, 5 allergy, and immune disorders.10,11
Clinical presentation of primary AR
Primary AR is characterized by a triad comprising widening of the nasal cavity, greenish crusts, and foul nasal odor (foeter). Progressive atrophic changes in the nasal cavity and turbinate can lead to paradoxical nasal obstruction. 3 Paradoxical nasal obstruction describes a patient who perceives nasal congestion with a wide and patent and wide nasal cavity. 5 Generally, AR tends to affect women more than men and presents with bilateral crusting and a foul smell due to superinfections. 5 Atrophy in the olfactory epithelium of patients with AR can lead to the development of hyposmia or even anosmia. 3
Diagnosis of primary AR
The diagnosis of primary AR is based on the appropriate symptoms and physical findings, along with consistent findings on computed tomography (CT) of the sinuses. 12 No specific investigation has been conducted on primary AR. Therefore, it was diagnosed to exclude other causes of secondary AR. There are many diagnostic tests to exclude secondary causes of AR, including a complete blood count to exclude anemia (low hemoglobin level) and infections (leukocytosis). A nasal swab should be taken for stains and culture if leukocytosis occurs. An elevated erythrocyte sedimentation rate is found in granulomatous infections, such as tuberculosis. Evaluating nutritional status by serum protein and plasma vitamin levels is necessary to exclude malnutrition. 5 Evaluation of underlying systemic diseases, such as leprosy, sarcoidosis, granulomatosis with polyangiitis (GPA) (Wegener disease), GPA, or syphilis, should be considered if systemic symptoms, such as weight loss, shortness of breath, or chronic epistaxis, are present. In this case, laboratory evidence of a systemic disorder such as hematologic and renal abnormalities or an abnormal finding on chest radiography may also suggest an underlying inflammatory process. 13 In addition, serological tests, such as venereal disease research laboratories test, can be performed to exclude syphilis in suspected patients. Radiological investigations such as chest radiographs and CT scans can also be used to exclude secondary causes of AR.
Histopathology
Normally, the nasal mucosa consists of 3 layers, beginning with the epithelium of the basal membrane, which separates it from the tunica propria or stroma. The nasal epithelial layer is formed by pseudostratified columnar epithelium, mainly of the ciliated type, with goblet cells attached by desmosomes. The stroma is divided into 3 sublayers starting superficially with a lymphoid layer, a glandular layer consisting of seromucinous glands, and a venous pseudo cavernous layer adherently attached to the periosteum and perichondrium. 14 AR affects all layers of the nasal mucosa and has different levels of severity. Changes ranged from some abnormality in the pseudostratified columnar epithelium to metaplasia of the respiratory epithelium to stratified squamous epithelium with keratinization accompanied by a decrease in goblet cells. 1 The basement membrane, if present, usually appears thin. Stroma changes included normal-looking serous and mucinous glands with inflammatory cell infiltration in the lymphoid immediately under the epithelial layer. The periarteritis and endarteritis of terminal arterioles, inflammatory infiltration, and basement membrane thickening are all observed. However, Taylor and Young denied these changes. 15
The nasal mucosa starts anteriorly with a squamous epithelium in the vestibule and gradually changes to a pseudostratified columnar epithelium with numerous ciliated cells posteriorly. 16 Garcia et al suggested that the flow of water and airflow in the anterior portion were more significant than in the posterior part due to the ciliary effect on the posterior lining mucosa. Thus, in the case of AR, water flow and airflow increase in the nasal cavity’s rear part, leading to mucous evaporation. The drying effect of airflow is believed to cause the respiratory mucosa’s metaplasia to the squamous type. 17 Also, Bourne found that the capillary endothelial layer of AR tissue had more than a normal cytoplasm and strongly reacted with alkaline phosphatase, explaining the underlying bone’s thinning. 18
Vascular involvement has 2 classic categories that Taylor and Young have reported. AR Type 1 is the most typical type (50-80% of cases) with periarteritis, endarteritis obliterans, and the terminal arterioles having periarterial fibrosis as an outcome of prolonged infections with plasma cell and round cell infiltration. By logic, these patients will be relieved from the influence of vasodilating action of estrogen treatment. AR Type 2, a less common type (20-50% of entire cases), has capillary vasodilatation. The dilated capillaries have endothelial cells that have more cytoplasm than usual and show a definite alkaline phosphatase reaction telling running bone resorption, which is a characteristic feature of this illness. This variety is not manageable by estrogen therapy. Nevertheless, in a single study, eighty percent of cases were consistent with the Type 2 histopathological grouping with capillary vasodilatation. 15 Similarly, Bunnag et al’s study showed that 80% of patients had Type 2 capillary involvement. 19
Management
The primary goal of AR management is to decrease crust formation, increase nasal hydration, and attempt to solve atrophy by managing the underlying causes, starting from prevention to medical management and even surgical intervention, if needed. 20 For primary AR, various management modalities have been suggested in the literature, as described below.
Medical management
The mainstay of the management of AR is conservative medical management, locally or systemically, which includes:
Nasal douches
A solution made of 28.4 g of sodium bicarbonate, 28.4 g of sodium diborate, which acts as an antiseptic and buffers the bicarbonate in the solution, 56.7 g of sodium chloride to make the solution isotonic, and 280 mL of warm water. Irrigation for both nostrils was performed with a 10 to 20 cc syringe or any other nasal irrigation device 3 to 4 times daily. During irrigation, the patient was advised to say “k k k” to close the velopharyngeal sphincter, thereby preventing aspiration. 5
Sumaily et al compared homemade saline solutions used for nasal irrigation and their effect on mucociliary clearance (MCC). They found that saline with iodized table salt improved MCC in healthy people, similar to saline without iodized salt, with a significant decrease in saccharine clearance time (SCT), which was more pronounced in iodized saline solution. 21 They evaluated the effect of diluted baby shampoo saline irrigation (1% concentration) on MCC in healthy subjects and found an increase in SCT after using the irrigation compared to SCT before using. 22
Nasal drops
Glucose glycerin drops consisting of 25% glucose were found to inhibit bacterial growth by fermentation, which produced local lactic acidosis and prevented bacterial growth. Glycerin is a lubricant that increases mucosal moisturization by absorbing atmospheric water. It is recommended to use it after nasal douches. 5 Liquid paraffin nose drops are effective lubricants, but they are not recommended due to the risk of inhalant lipoid pneumonia.5,23 Estradiol in Arachis oil drops can be used based on histopathological findings, and it was found to be beneficial in Type 1 but not recommended in Type 2 AR, as it may lead to a worsening of the condition. 5 Topical antibiotic solutions, such as 80 mg of gentamicin sulfate dissolved in 1 L of normal saline solution, should be reversed in patients with purulent discharge and target the causative organism, mainly Klebsiella. 24 In one study, patients who received streptomycin and vasodilator medication orally or subcutaneously had satisfactory results. 25
Systemic medications
It is usually necessary from time to time and should be directed according to the nasal culture of purulent discharge. Tetracycline, aminoglycosides, and, more recently, ciprofloxacin (250-500 mg twice daily for 4 weeks) have been successful. 3 Supplements are recommended for iron, zinc, protein, and vitamin (A and D) supplements for malnutrition patients with mineral deficiencies. 5 Bernat found satisfactory results from iron therapy in 50% of patients, as they noticed improvements subjectively. 26
Nasal submucosal injections
Many materials have been used for nasal submucosal injection to treat patients with AR. A study using autologous fat and platelet-rich plasma injected into the inferior and middle turbinate, septum, and nose floor showed a significant improvement in subjective and objective aspects, as indicated by a decrease in the SNOT 20 score and the nasal MCC time, respectively. 27 The placental extract contains vitamins, nucleotides, and amino acids and has anti-inflammatory and wound-healing effects. It also causes vascularization, and vasodilation causes a decrease in the space of the roomy nasal cavity. Jaswal et al found that patients treated with systemic rifampicin were superior to those treated with a nasal injection of placenta extract in a subjective, objective, and histopathological study. 28 Vitamin E is an anti-inflammatory and antioxidant that prevents membrane lipid destruction. Testa et al used a nasal spray of pure α-tocopherol acetate, 2 puffs in each nostril, 3 times a day for 6 months, and found an improvement in nasal symptoms and perception of nasal airflow but no increase in nasal resistance. 29 Mitomycin C has an antiproliferative effect, inhibiting fibroblast activity and preventing nasal mucosa fibrosis. In one study, mitomycin C was added to nasal douches (0.2 mg/mL in 200 mL of warm water) as an adjuvant to oral rifampicin and showed a significant subjective and objective improvement along with the control group, who received oral rifampicin with nasal douches without mitomycin, with the superiority of the study group over the control group in decreasing crustation and softening thickened mucoid discharge. 20
Vaccine
In swine, AR is mainly caused by Bordetella bronchiseptica and Pasteurella multocida. Vaccines consisting mainly of toxoids against these organisms showed control of the situation, which must be evaluated in managing AR in humans. 30
Surgical management
Surgical approaches have been used to manage AR. They aim to decrease the size of the nasal cavities to increase nasal resistance. Therefore, the drying effect of air turbulence decreases. Second, regeneration of the normal nasal mucosa is promoted by temporary partial or complete closure of the nostril; third, increasing lubrication of the dry nasal mucosa by increasing the activity of the nasal mucosal glands or bringing secretions from other places. Furthermore, it improves the vascularity of the nasal cavities mainly by blocking the sympathetic system. 5
Decreasing the size of the nasal cavities
Many approaches have been used to decrease the nasal cavity, from Caldwell-Luc up to the endoscopic approach. Many materials have been used, including homologous autologous endings with synthetic materials. 5 Shina et al implanted acrylic resin implants in 60 patients, with improvement in 80% of the patients. After 2 years of follow-up, 80% of the patients worsened due to implant extrusion, while the result was satisfactory for the remaining 20%. They also used a Dermo-fat implant, harvested from the anterior thigh and implanted on the nasal floor with a cure rate of 25% due to the risk of resorption. 31 A graft is usually performed in empty nose syndrome (ENS) cases and implanted in the lateral nasal wall just below the inferior turbinate after the elevation of the mucoperiosteum starting at the level of the pyriform aperture. Park and Jang used it in a patient with primary AR with significant subjective and objective improvement. 32
Promoting regeneration of the normal nasal mucosa
Young operation: Young suggested complete closure of the unilateral nostrils or both to promote regeneration of healthy mucosa. His technique involved a circumferential incision at the mucocutaneous junction, and the skin was sutured together. 33 They believed that the closure of the nostril would stop air turbulence and increase CO2 and pH, which would help in mucosal regeneration. In addition, they thought that closure would create negative pressure, which would promote revascularization. However, patients may develop scars and vestibular stenosis. 4 Some modifications were applied to Young’s approach, targeting improving the results or preventing its disadvantages.
- Sinha modification: Instead of complete nostril closure, he did partial nostril closure with the same technique as the Young by leaving a small opening in the nostril. He achieved complete cure in cases with a 3 mm opening, while the percentage of cure dropped to 70% as the size increased to 5 mm. 31
- Gadre modification: He suggested a modification that involves elevating the mucosal flap posterior to the incision rather than reflecting the nasal vestibular skin. The mucosal flap was then sutured together, forming the obliterating membrane. 34 The result was a three-layered membrane; the external epithelial layer continued with the skin externally, the internal epithelial layer continued with the mucous membrane internally, and fibrous tissue was found. 35 The advantage is the simplicity of raising the flap and aesthetic improvement because the obliterating membrane will not be evident. 35
- Ghosh’s vestibuloplasty: Ghosh hypothesized the etiopathogenesis of AR, namely that decalcification of the turbinate secondary to reflex sympathetic dystrophy, which makes them collapsible under the impact of the inspiratory stream, which hits them continuously, resulting in AR. His technique elevates the flap from the skin on the lateral wall from the ala 3 mm posterior to the nostril opening with its base to the vestibular lumen. Then fold it over itself with its base laterally and suture it together so the air stream hits it and is redirected to the septum. Thus, the lateral wall is kept without direct air turbulence. This technique will allow the lateral nasal wall to regenerate normal mucosa while the nasal cavity is opened and accessible for cleaning and the advantage of doing both nostrils at 1 stage. 36
- El Kholy modification: To prevent scar and vestibular stenosis, he modified by making a hemitransfixion incision in the contralateral nasal cavity, elevating the flap, and then making a cartilage incision to access the ipsilateral mucoperichondrial flap. Additionally, an incision was made at the posterior end of the elevated ipsilateral flap, which was then reflected and sutured with another flap raised on the lateral vestibular skin on the ipsilateral side. 37
Recanalization of the obturator membrane: Young admitted to having restenosis after recanalization and may need revision surgery for a satisfactory opening. 33 Gadre suggested a three-flap technique to prevent restenosis and applied a stent with a tube for 6 weeks with no documented restenosis. 35 Pavithran et al studied 3 types of stents after recanalization using 3 flap techniques: silicone suction tube tips, dental wax plates, and customized acrylic stents. The tips of the suction tube do not have restenosis, but superior blunting of the nasal valve, while the dental wax plate has a risk of restenosis and superior synechia. The custom acrylic stent had the best result, with no restenosis or blunting. 38
Increasing lubrication of the dry nasal mucosa
The described operations are technically challenging with no satisfactory results. Wittmaack’s operation was reimplanting the Stenson’s duct to the maxillary antrum. This technique will help moisturize the dry nasal cavity through parotid secretions. 5 Sharan performed other operations using the Caldwell-Luc approach, in which the maxillary sinus mucosa was elevated from the sinus wall and then reflected through the antrum to the nasal cavity, filling the roomy nose and increasing secretion through the normal sinus mucosa. 39
Improving vascularity of the nasal cavities
Stellate ganglion injections: A local anesthetic agent (10–15 cc of 1% xylocaine) was injected into the stellate ganglion of the cervical sympathetic chain to block the sympathetic action that causes vasodilation. The effect of injection was confirmed by Horner syndrome and nasal mucosa congestion. The daily injection is recommended in unilateral cases, while in bilateral cases, injected separately on alternative days to avoid bilateral recurrent laryngeal nerve palsy. 5 However, Sinha et al found that the effect is temporary, and patients relapse within 4 to 8 days. 31 Cervical sympathectomies have the same concept as stellate ganglion injection but with permanent results. 5
Secondary AR
The secondary type of AR is attributed to a known underlying cause. Causes can be traumatic or iatrogenic. This is called ENS. Other causes could be secondary to granulomatous diseases such as tuberculosis, leprosy, granulomatosis with polyangiitis, or sarcoidosis. 5 This rare rhinologic disorder develops many years after sinonasal surgery. This was based on coronal CT showing a total or partial inferior and middle turbinectomy. Patients may have these conditions months to years after surgery. 40
ENS patients typically present with excessive nasal crusting, malodor emanating, and paradoxical nasal obstruction in the nasal cavity. Other associated symptoms include headache, facial pain, anosmia, mucosal dryness, dyspnea, sleep disturbances, epistaxis, and rarely mucopurulent rhinorrhea. ENS has an unusual symptom, aprosexia nasalis, where the patient becomes highly preoccupied with maintaining a breathing sensation, leading to a chronically reduced concentration. The sensation of not being airborne is not relieved by breathing in the mouth and mostly leads to a negative psychological impact in ENS patients, manifesting as depression, anxiety, anger, fatigue, frustration, and irritability.2,41
ENS can be classified according to surgical intervention before presentation 40 :
ENS due to inferior turbinectomy (most common)
ENS due to middle turbinectomy
ENS due to inferior and middle turbinectomy
ENS with remnant tissue of the turbinate
Pathophysiology of ENS
ENS is a poorly understood condition. Numerous studies have emphasized that the sensation of nasal obstruction is not correlated with anatomical nasal obstruction; therefore, these studies suggest that the perception of nasal patency is a neurosensory rather than an anatomical mechanism. 40 Consequently, in patients with ENS, when a large amount of inspired airstream has less contact with the surface area of the mucosal wall due to the lack of turbulence, this airflow pattern produces insufficient mucosal cooling, leading to a lesser perception of nasal patency. 40 In individuals with ENS, there were 3 consistent changes following inferior turbinate excision. The airflow patterns observed are laminar as opposed to turbulent. The velocity of the airflow vectors is increased rather than medium velocity. The compromised airflow to the inferior portion of the nasal cavity causes a shift in the airflow upward toward the middle meatus and nasopharynx region. 42
Another theory suggested that poor trigeminal nerve regeneration or damage after nasal surgeries may lead to poor input into the air-inspired perception pathway. Patients with ENS are strongly associated with conditions that affect mental health, such as depression and anxiety. This psychogenic effect affects nasal perception of airflow. 43 The study by Collins et al focused on the turbinate perimeter ratio in pigs. The findings suggest that this ratio could serve as a more reliable morphometric measure of AR. Additionally, the data collected from this ratio is suitable for quantitative analysis. 44
Clinical presentation of ENS
Patients with ENS usually present with paradoxical obstruction, indicating previous nasal surgery that led to a patent airway, while the patient complains of nasal obstruction. Other symptoms may include crusting, dryness, and even suffocation. 43 ENS differs from primary AR, which usually presents as Klebsiella ozaenae colonized in the nasal cavity with extensive crusting. Compared to other sinonasal conditions, such as chronic sinusitis and deviated nasal septum, patients with ENS have worse symptoms, according to 6-item ENS questionnaire (ENS6Q). This condition affects the individual’s cognitive ability and could lead to anxiety and depression. 43
Diagnosis of ENS
ENS was first introduced to describe patients with nasal obstruction and the absence of normal nasal tissue. 45 In contrast to primary AR, patients with ENS generally have an underlying cause of symptoms such as trauma, radiation therapy, and nasal surgery. 2 The diagnosis is based on the clinical symptoms of the patients and the clinical findings because several methods have been described to objectively assess nasal patency: anterior rhinomanometry, acoustic rhinometry, and peak nasal inspiratory flow, but they are not correlated with the severe symptoms of the patients. 40
CT scans of patients with ENS can reveal thickening of the mucosa in the septum and sinuses, enlargement of the sinuses of the nasal cavity, destruction of the lateral nasal wall, and partial or complete resection of the middle/inferior turbinate. 2 An ENS6Q containing 6 questions with a score of 0 to 5 is used to investigate common presenting symptoms of ENS. A score equal to 10.5 and more confirms the diagnosis of ENS.
Office-based cotton test: This is an office test to evaluate the effect of the placement of cotton moisturized with normal saline in the nose area with deficient tissue. 45 Cotton was left in place for 20 to 30 minutes, then a reassessment of patient symptoms was performed using EMS6Q to confirm diagnosis and results in the surgical management of those patients. 46
Histopathology of ENS
In the secondary type of AR, histopathology is based on the underlying causes. These include granulomatous sinonasal diseases such as sarcoidosis, tuberculosis, leprosy, and GPA. In the case of sarcoidosis, the histopathology shows noncaseating granulomata associated with progressive fibrosis due to a granulomatous response, and no vasculitis or cholesterol crystals can be detected. 47 In tuberculosis and leprosy, histopathology shows that caseating granulomas have submucosal fibrosis and decrease the number of submucosal glands. A biopsy study showed epithelioid cell granulomas associated with T lymphocytes and vasculitis in granulomatosis with polyangiitis. 48
In ENS, histopathological studies have shown decreased submucosal glands, submucosal fibrosis, and squamous metaplasia. At the same time, ciliated mucosa and goblet cells were preserved in the epithelial layers. In the same study, they found that 35% of patients with ENS had goblet cell metaplasia, indicating a change in ciliated cells to goblet cells rather than hyperplasia of the residual goblet cells due to the activation of epidermal growth factor receptors after surgical insult. Immunohistochemical staining revealed a decrease in transient receptor potential channel melastatin 8 “TRPM8” receptors in ENS patients, which ended with a sensation of nasal obstruction. 49
Management of ENS
Prevention of the disease is mandatory because the management options become restricted once the ENS manifests. Carefully examining the need for surgical turbinectomy and other strategies, such as medical management, in allergic patients to reduce tissue loss and allow fast restoration of nasal physiologic mechanisms is critical.3,50
Other surgical approaches for the management of hypertrophied turbinate have been used to minimize the incidence of ENS, including electrical cauterization, laser surgery, submucosal turbinoplasty using microdebrider, partial turbinectomy, and submucosal resection using special techniques, including radiofrequency ablation or quantum molecular resonance (QMR) techniques. 51 Maniaci et al found microdebrider-assisted turbinoplasty superior to the QMR technique in controlling the short and long-term obstructive symptoms, with QMR showing less postoperative complication. 52 In another study, the QMR technique showed less postoperative complication than the coablation technique, which controls the obstructive symptoms more than the QMR technique. 53 ENS treatment can be classified into medical and surgical options. In some patients, a multidisciplinary approach may be needed that involves ear, nose, and throat surgeons, allergists, and psychiatrists to manage this challenging disease; surgical choices are usually attempted only after an adequate trial of medical management, counseling, and education has not been able to improve for a period of 6 to 12 months, taking into account the potential neurologic mechanisms of ENS development. 54
The medical treatment of ENS
Medical treatment includes hydration with saline or oil-based lubricants, mucosal moisturization, increased fluid intake, intermittent closure of the nostrils (to return humidity), and an aggressive regimen of nasal saline sprays. 54 For patients with psychological symptoms, cognitive behavioral therapy might help, and the careful use of newer-generation antidepressants might complement therapy. 55
Surgical management of ENS
Recently, surgical therapy for ENS has received excellent acceptance because evidence of beneficial outcomes in both nasal symptoms and the comorbid mental health sectors have been reported.45,56. In a systematic review, Leong reported that corrective surgery improved ENS complaints, nasal symptoms, psychopathological conditions, and sleep function. 56
The general concept of surgical intervention is to restore nasal physiologic function. 2 Submucosal filler injections are ideal short-lived bulking agents to increase tissue deficit sites, and this procedure can be performed in the clinic. This measure provides time for total healing of the operated tissues, which may subside the patient’s initial complaints. Young’s approach to temporary nasal closure (either through fabricated plugs or tissue flaps) has been described as beneficial for AR disease.37,57 This approach might also help patients with ENS due to the resemblance between AR and ENS. 2 Most surgical treatments for ENS involve reshaping nasal cavities to act as previously resected nasal tissue. These procedures are considered turbinate reconstruction procedures. Fortunately, reconstruction of the lower turbinate may be accomplished at the lateral nasal wall at the level of the inferior meatus. Several materials have been used for submucosal grafting:
temporary fillers,
autologous cartilage,
acellular dermal allografts, and
synthetic implants
Temporary Fillers
The submucosal filling of cross-linked hyaluronic acid has been described as a minimally invasive option in patients with ENS. In this description, the commercial product Juvéderm (Allergan, Dublin, Ireland) was used, but a variety of similar products are available; these alternatives are likely to offer similar usefulness. 58
Acellular Dermis Xenografts and Allografts
The submucosal implantation of acellular dermis allografts is well-described for the surgical management of ENS. 2 Human acellular dermal matrix (such as Alloderm, Allergan, Inc.) and porcine submucosal intestine submucosa are outlined to integrate into surrounding soft tissues over time. 59 To place these grafts, submucosal pockets are made under GA in the target location (typically the lateral wall of the inferior meatus). The graft material can then be tightly rolled and packed inside the pocket to narrow the overly patent nasal passage. Multiple sites along the lateral wall of the nasal cavity can be targeted for external graft placement. The locations of obvious tissue loss guide the implant site. In general, the data show the great efficacy of this procedure with lasting benefits. 42 Some users have noted resorption and failure rates of 10 to 30% for matrix materials. Fragmentation of the intestinal submucosal membrane with loss of neo-turbinate projection has been reported, making this xenograft unfavorable for this application.23,59
Autologous Cadaver Cartilage and the Donor
The ease of harvest, biocompatibility, and reduced material cost of autologous cartilage make this an attractive option for ENS surgery. The objectives of cartilage grafting are similar to those of allograft placement, and the cartilage placement techniques are analogous to allograft placement techniques. However, cartilage has the upper hand of a semirigid consistency and thus can be formed and sized to achieve the desired 3D shape. Autologous cartilage harvested from the nasal septum, ear, or rib can be carved and built to form a cylindrical shape before placing it in a submucosal pocket to simulate the lost turbinate tissue and narrow the nasal airway. Because many patients with ENS do not have adequate septal cartilage due to previous septoplasty procedures, costal or auricular cartilage may be required if the surgeon wants to use an autologous cartilage graft.60,61 The characteristics of the included studies on primary and secondary AR are shown in (Tables 1 and 2). The histologic features of primary and secondary AR are presented in (Table 3).
Characteristics of the Included Studies on Primary AR.
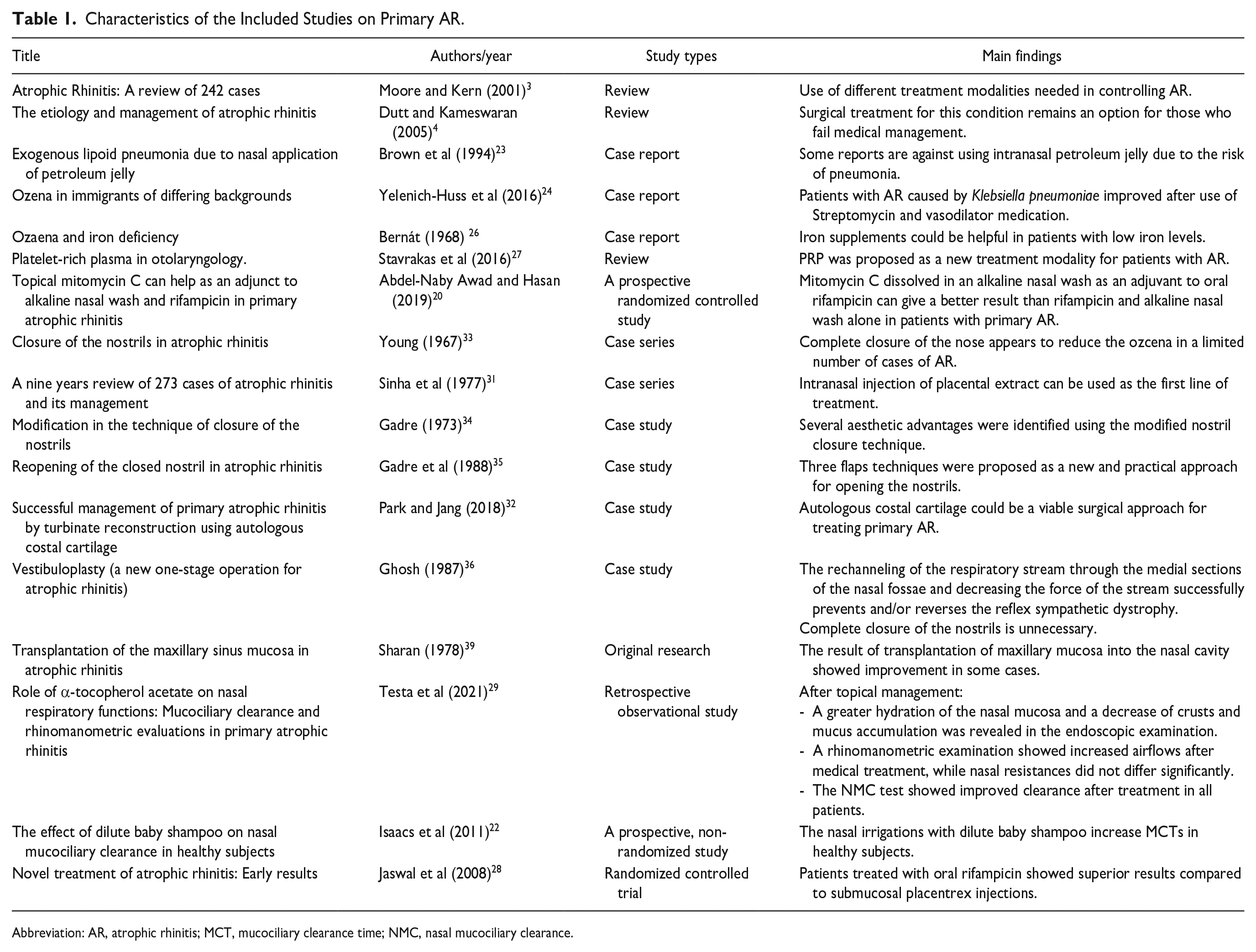
Abbreviation: AR, atrophic rhinitis; MCT, mucociliary clearance time; NMC, nasal mucociliary clearance.
Characteristics of the Included Studies on ENS.
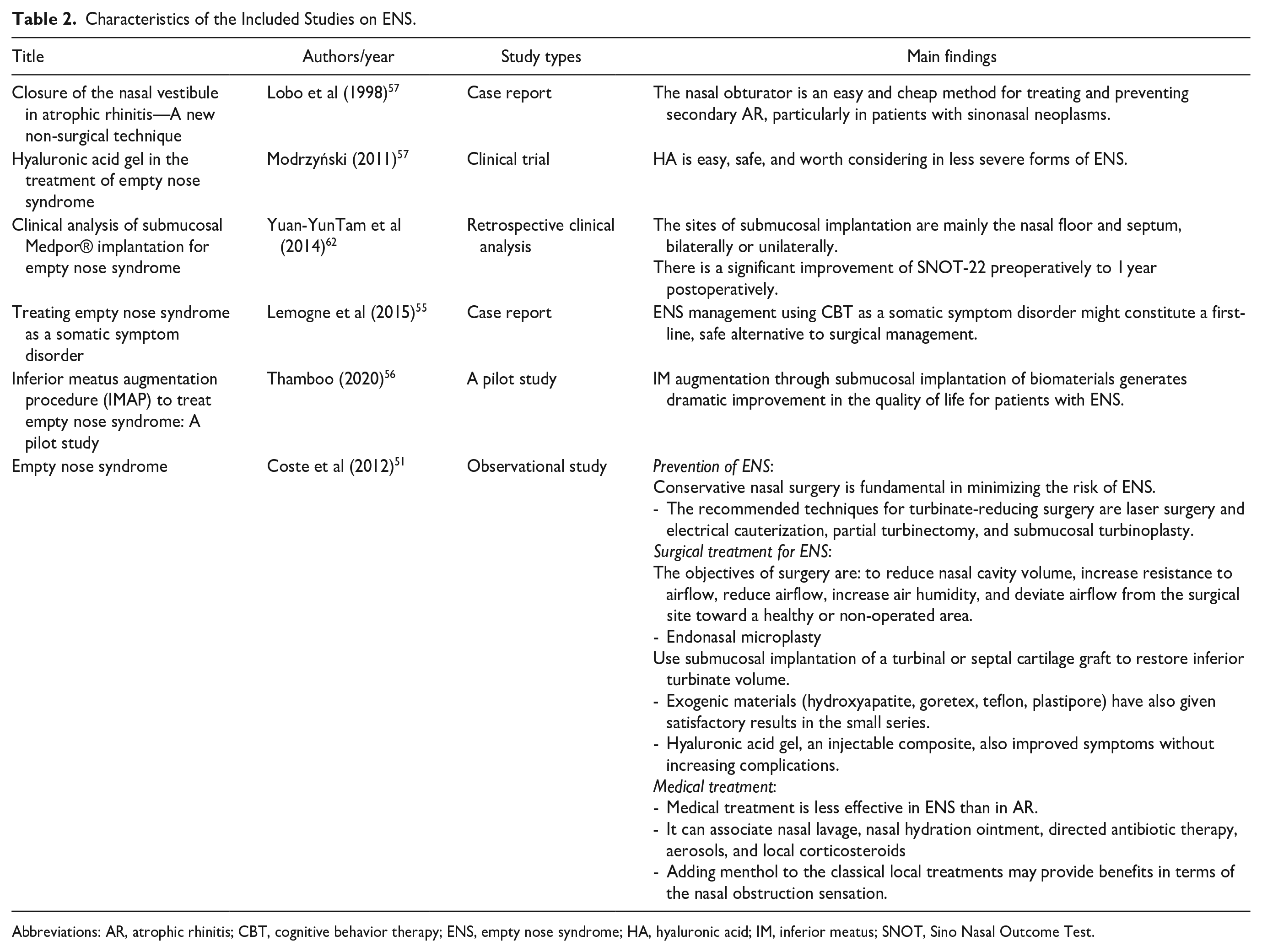
Abbreviations: AR, atrophic rhinitis; CBT, cognitive behavior therapy; ENS, empty nose syndrome; HA, hyaluronic acid; IM, inferior meatus; SNOT, Sino Nasal Outcome Test.
Histological Features of PAR and SAR.
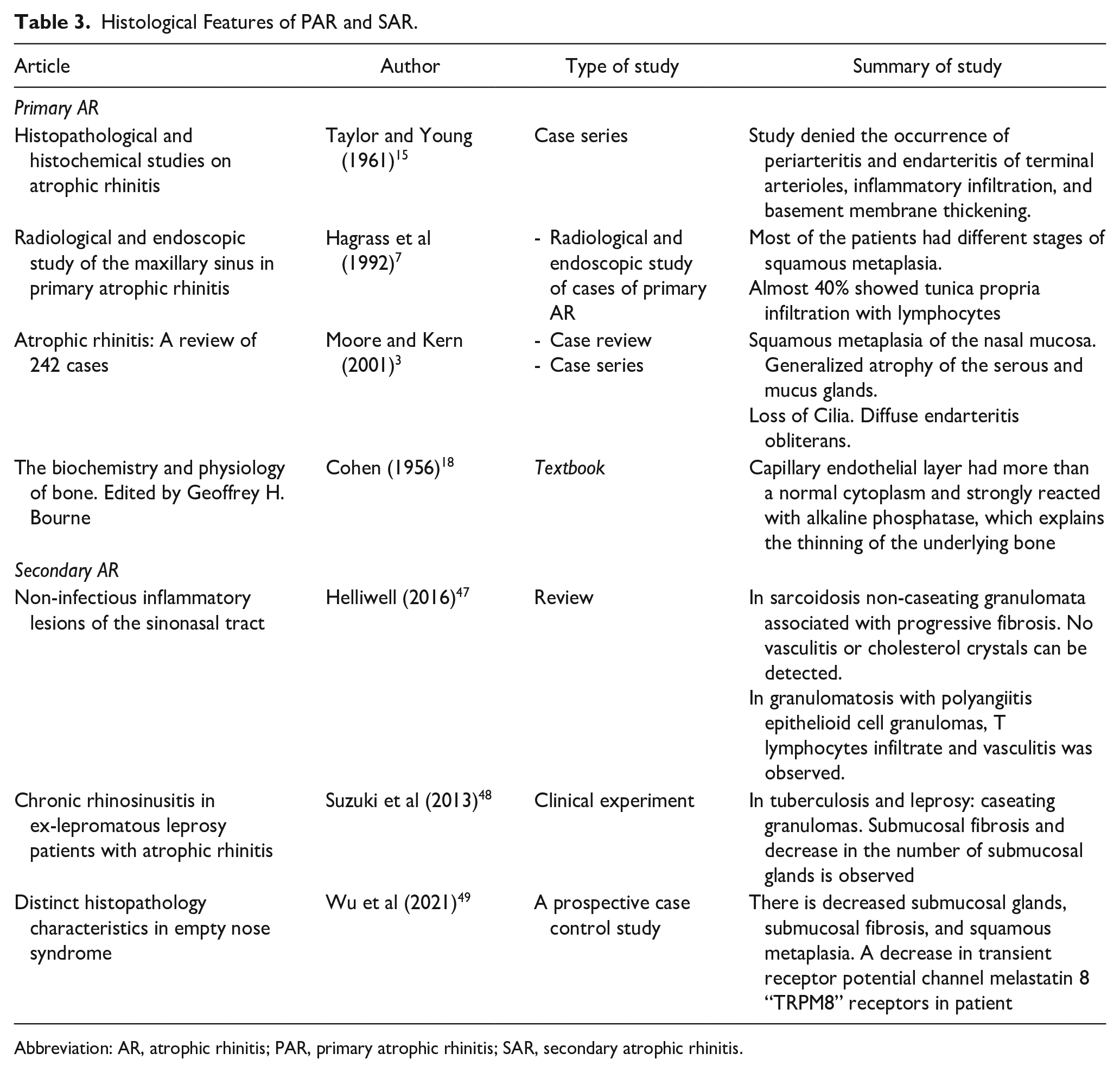
Abbreviation: AR, atrophic rhinitis; PAR, primary atrophic rhinitis; SAR, secondary atrophic rhinitis.
Synthetic Implants
The use of synthetic implants has been studied in ENS reconstructive surgery. These implant types include silicone perforated sheeting or porous polyethylene (MedPor, Stryker Corporation, Kalamazoo, MI, USA). 62 These materials do not react and are designed to allow tissue growth to penetrate the material and improve long-term integration. Synthetic implants are generally inexpensive and easy to obtain in most practices. Since synthetic implants are foreign bodies by nature, infection, and extrusion are possible complications. After tissue ingrowth, implant removal due to scarring is challenging if such extraction is warranted.
Conclusions
The prevalence of AR varies between different populations with different etiology and clinical manifestations. The availability of a wide range of diagnostic procedures and newer treatment modalities could improve the quality of life of AR patients. This narrative review has comprehensively outlined the various aspects of RA, including the impact of newer treatment modalities on patient quality of life.
Footnotes
Author Contributions
I. A. Sumaily was involved in concept and supervision. N. A. Hakami was involved in concept. A. A. Alserhani was involved in design and literature review. A. D. Almutairi was involved in design and literature review. M. M. Abualgasem was involved in data collection and/or processing and literature review. E. A. Abulqusim was involved in data collection and/or processing, analysis and/or interpretation, and literature review. A. A. Alsudays was involved in data collection and/or processing, analysis and/or interpretation, literature review, and writing. A. A. Alghulikah was involved in writing.
Data Availability Statement
Data are available upon request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval was waived from the institutional review board.