
Abstract
Hemangioma is a subtype of benign vascular tumors. Although they are commonly found in head and neck region, they are rare in the external auditory canal. Few cases reported capillary hemangioma in the external auditory canal with surgical excision is the mainstay of management and low recurrence rate. We present a 41-year-old woman with left external auditory canal capillary hemangioma and cartilage with its perichondrium graft was used for repairing the defect after surgical excision.
Introduction
Hemangioma is a subtype of benign vascular tumors classified as capillary or cavernous according to their histopathological appearances. 1 Capillary hemangiomas are composed of arranged capillary-like channels, whereas cavernous hemangiomas are composed of an endothelial lining with large cavernous vascular spaces.2,3 Although the etiology is unclear, 1 some authors have linked them to infections, trauma, medications, and hormonal changes. 4 They are common in the head and neck region and are usually located on the cutaneous or mucosal areas of the nasal or nasal cavities. 1 Although it is very rare for hemangiomas to present in the external auditory canal, a few cases have been reported in the literature, and cavernous hemangiomas appear to be more common in this location (57.8%). 3
Hemangiomas can be asymptomatic or may cause symptoms like conductive hearing loss, episodic bleeding, and aural fullness. Computed tomography (CT) is the primary test available to determine the size and location of the mass, and whether it involves bone or middle ear structures. 5 The mainstay of treatment is surgical excision, and preoperative angiography and embolization are usually performed in cases where massive bleeding is expected.3,5 To the best of our knowledge, only 17 cases of capillary hemangioma in the external auditory canal have been reported in the literature. We present here our experience with a capillary hemangioma in the left external auditory canal.
Case Report
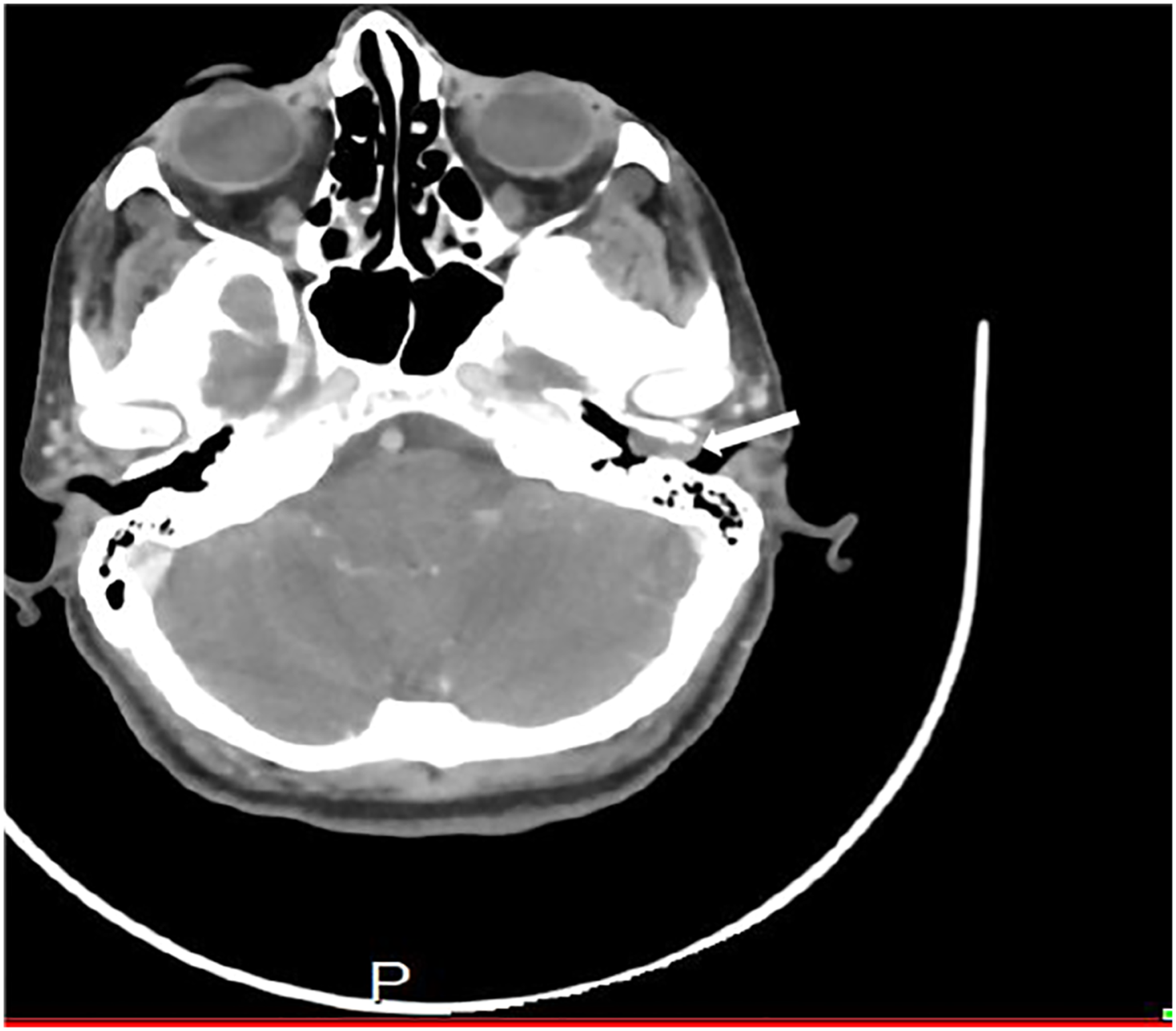
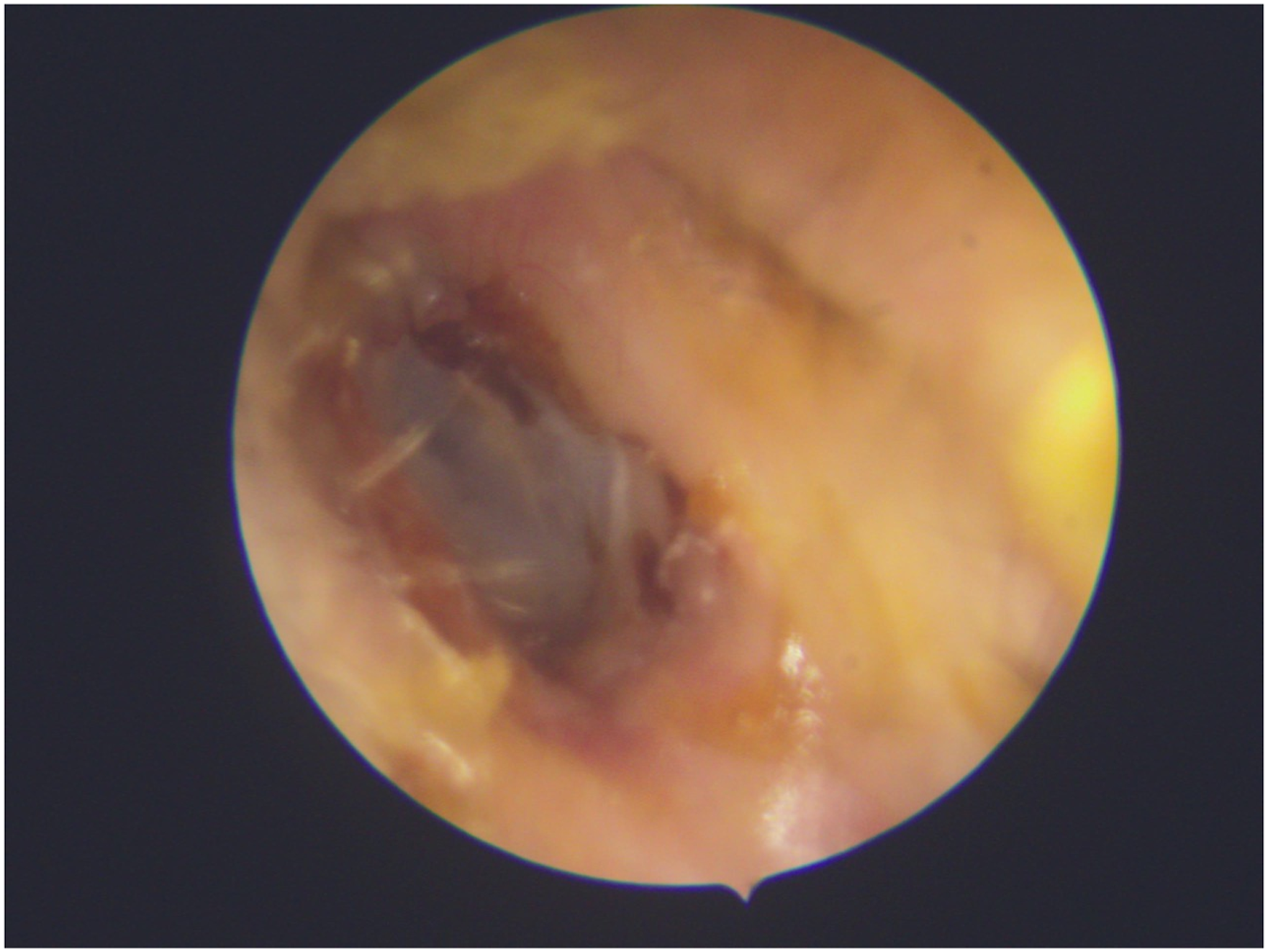
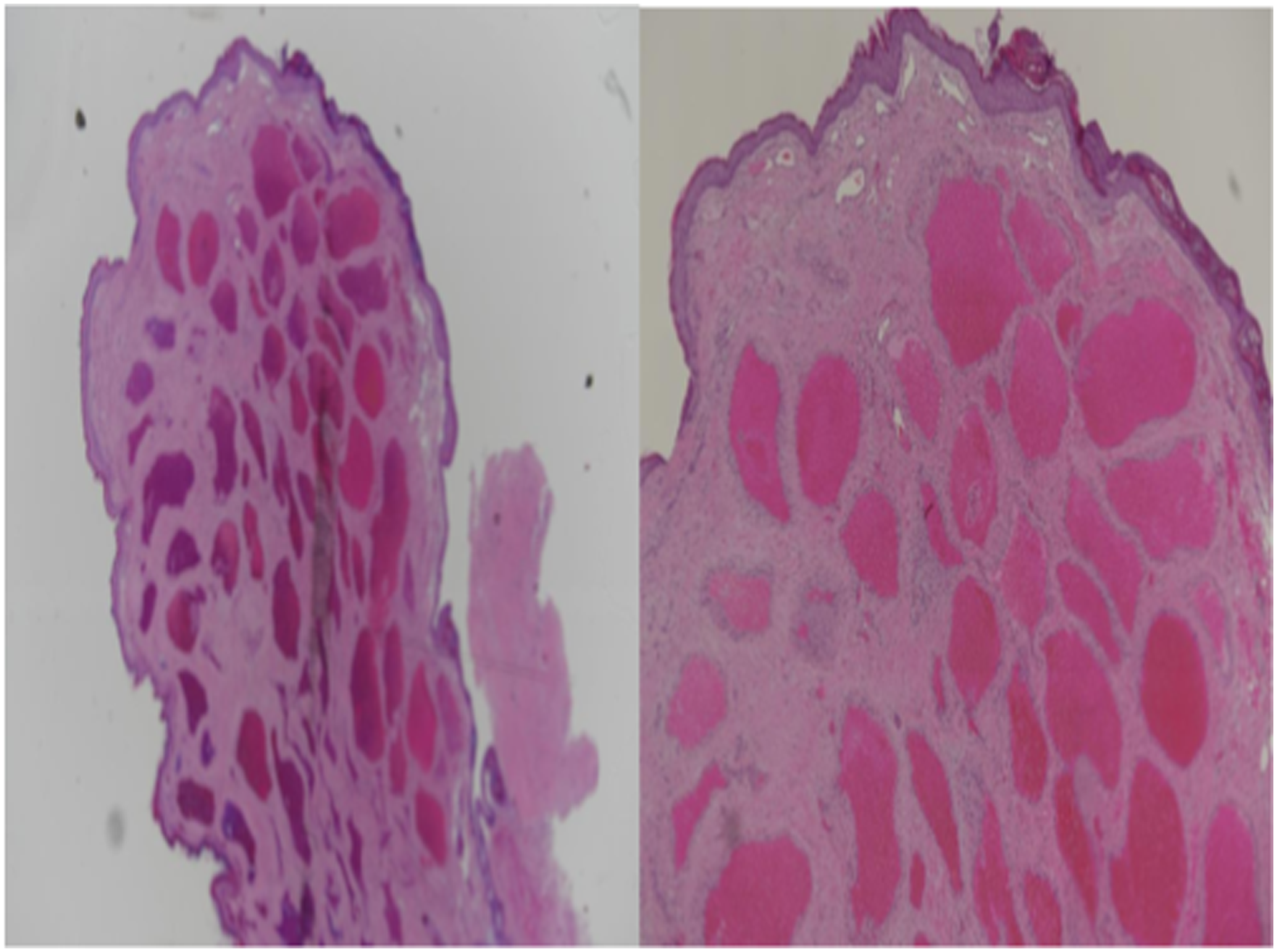
A 41-year-old woman presented to the outpatient clinic of the Security Forces Hospital complaining of pulsatile tinnitus in the left ear and progressive hearing loss over 6 years with intermittent otorrhea. The patient did not report any pain in the ear or aural fullness. Examination of the left ear revealed a bluish mass in the external auditory canal and bloody discharge. The tympanic membrane could not be visualized. Pure tune audiometry revealed moderate-to-severe conductive hearing loss in the left ear (Figure 1). Temporal CT with contrast confirmed the presence of a hyperdense mass in the left external auditory canal extending to the middle ear, suggestive of vascular tumor (Figure 2). The patient was taken to the operation room and underwent surgical excision of the mass through a transcanal approach. A soft blanchable mass measuring approximately 1 × .5 cm was removed from the posterior bony wall of the external auditory canal (Figure 3). After the excision, the canal was reconstructed from tragal cartilage with its perichondrium and silastic sheet applied over it. The tympanic membrane was found to be intact: it had only been displaced medially by the mass, and had thinned in the posterior site. There was a postoperative improvement in the patient’s hearing. On 3 months follow-up in the clinic after surgical resection, examination of left external auditory canal showed completely healed canal with no residual mass (Figure 4). The diagnosis of capillary hemangioma was made based on histopathology findings (Figure 5). Left pure tune audiometry indicating conductive hearing loss with large air-bone gap. Temporal computed tomography image showing a hyperdense mass in the left external auditory canal (arrow). Appearance of the mass after being excised from the external auditory canal. 3 months post-operative view of the left external auditory canal. Histopathological appearance of the capillary hemangioma.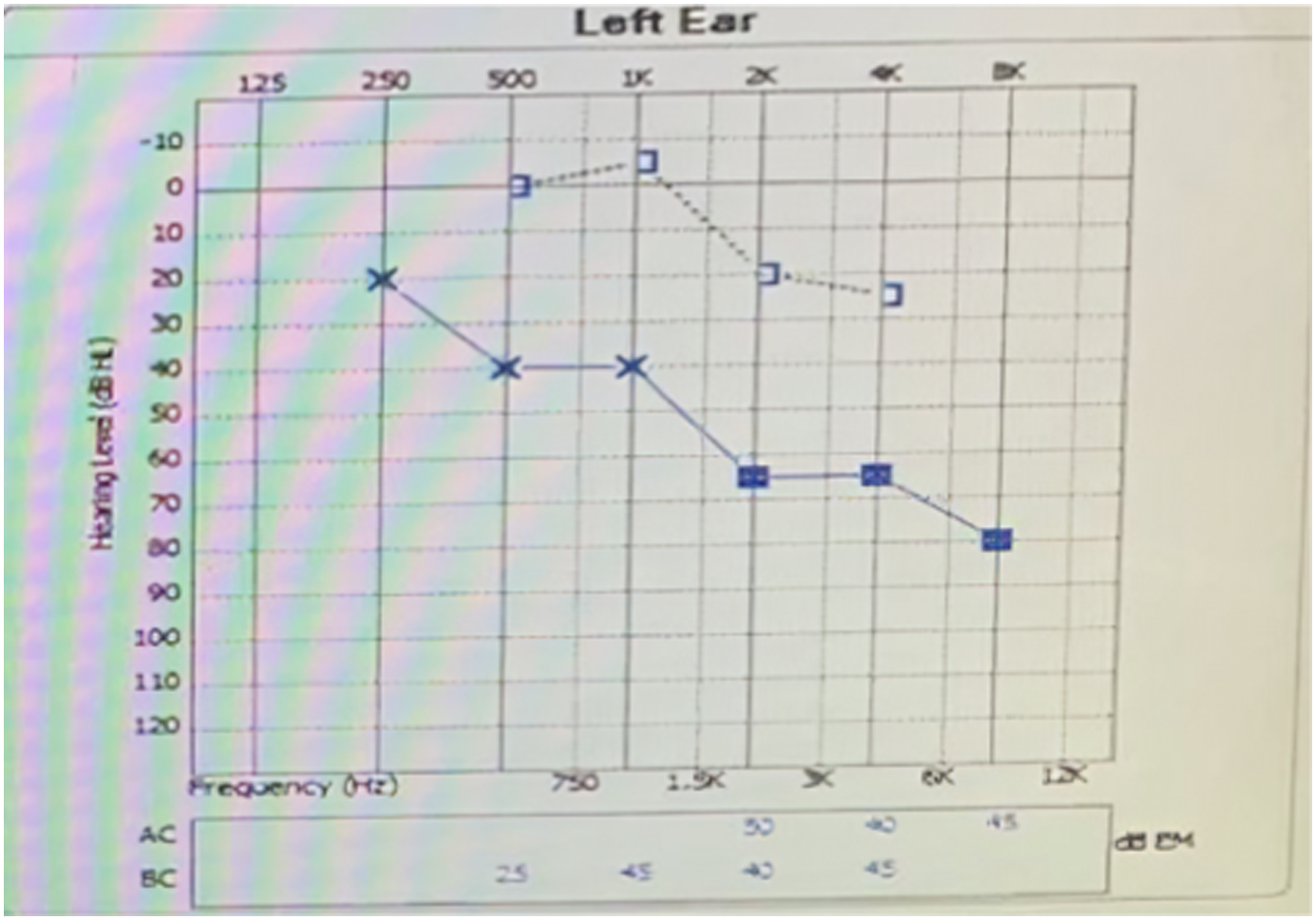

Discussion
Hemangiomas are benign vascular tumors that commonly occur in the head and neck region. Based on their histopathological appearance, they are classified into capillary or cavernous. Capillary hemangiomas appear as arranged capillary-like channels, whereas cavernous hemangiomas are composed of an endothelial lining with large cavernous vascular spaces. The presence of hemangiomas in the external auditory canal is rare, with only 39 cases having been reported. Seventeen of these cases corresponded to capillary hemangiomas, indicating that cavernous hemangiomas may be more common. Patients may only present with an asymptomatic mass or may report ear pain, discharge, aural fullness, pulsatile tinnitus, or episodic bleeding. Conductive hearing loss can also occur if the mass occludes the external auditory canal. 3 Differential diagnoses include aural polyp, attic cholesteatoma, glomus tumor, carcinoma of the external auditory canal, and arteriovenous malformation. 3 CT and magnetic resonance imaging are useful tools in the identification of vascular tumors. CT is the first choice for the determination of the size and extension of the mass and for detecting the presence of bone erosion. Preoperative angiography is helpful for the visualization and identification of feeding vessels. Embolization is usually performed when the mass to be removed is large or if massive bleeding is expected. A definite diagnosis is made on the basis of the histopathological appearance of the excised mass. Many surgical approaches for excision have been reported, including transcanal, endaural, and postauricular; and both general and local anesthesia have been used for the procedure. No surgical complications of capillary hemangiomas have been reported. Only one case of hemangioma reported to be unresectable that reached the cochlea and vestibule was reported in which the patient underwent radiotherapy and remained asymptomatic, a part of moderate conductive hearing loss. 6 The case reported here belonged to the rare category of capillary hemangiomas in the external auditory canal. In all the cases reported, patients affected by this kind of hemangioma underwent surgical excision via either a transcanal or a post-auricular approach.2,4,5,8-10 Only one case canal wall down mastoidectomy was performed. 1 In many cases, the excision can be performed under local anesthesia, with minimal controllable bleeding if the patient is cooperative and the hemangioma is confined to the external auditory canal.4,7,8 One patient with recurrent hemangioma underwent resection, and the reason for recurrence was reported to be the specific capillary hemangioma subtype, known as tufted angioma. Tufted angiomas present infiltrative features and are not capsulated, which explains the recurrence observed in that case. 11
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written consent was obtained by the patient herself.