
Abstract
Pyogenic granuloma is a benign vascular tumor of the skin or mucous membrane. One-third of pyogenic granulomas have been reported in the head and neck, but it is rarely present in the external auditory canal. Pyogenic granuloma mostly presents as a solitary granuloma, and only a few cases of multiple forms have been reported. This report describes a rare case of multiple pyogenic granulomas in the external auditory canal of a 36-year-old man along with a review of the literatures. Although it is very rare for PGs to occur in the EAC, it can be suspected in conditions such as after acute and/or chronic trauma, hormonal changes or systemic drug administration, rapid growth, and easy bleeding tendency with a friable surface. Some PGs may spontaneously resolve, but when they cause symptoms, excision is recommended for treatment and diagnosis. In the case of excision, the tumor should be excised down to the perichondrium level to prevent recurrence. Although PG mainly occurs in a solitary form, the present case shows a new clinical variation where multiple PGs were present in the EAC.
Introduction
Pyogenic granuloma (PG), or lobular capillary hemangioma, is a benign vascular tumor of the skin or mucous membranes. It occurs at any age, with a peak incidence in the second and third decades of life. 1 Moreover, it can occur in any part of the body, but one-third of PGs were reported in the head and neck region, especially on the cheek, lip, and oral cavity. Although PG is commonly found in the head and neck regions, it rarely presents in the external auditory canal (EAC). This is the first report of multiple PGs in the EAC of a 36-year-old man.
Case Report
A 36-year-old man presented with a mass in the left ear. The mass had been present for at least 2 years, but he could not recall when it appeared and whether its size changed. He had no history of trauma or insect bites and denied using cotton buds; however, he often rubbed his ear. He did not complain of hearing loss or ear fullness, and the mass was painless when manipulated. Physical examination revealed 2 masses in the left cartilaginous EAC. The one located laterally was .6 cm × .6 cm in size, and the other one was .3 cm × .3 cm. Both lesions were firm, smooth-lined, and erythematous. No bleeding or pain occurred during manipulation (Figure 1A). Imaging studies were limited due to the small size of the masses; however, they revealed highly enhancing masses confined to the superficial layers without adjacent bony erosions (Figures 1B). Preoperative images. Two polypoid masses in the left cartilaginous external auditory canal (A). Contrast-enhanced T1-weighted magnetic resonance imaging shows enhancing masses confined to the superficial layers (white arrow, B).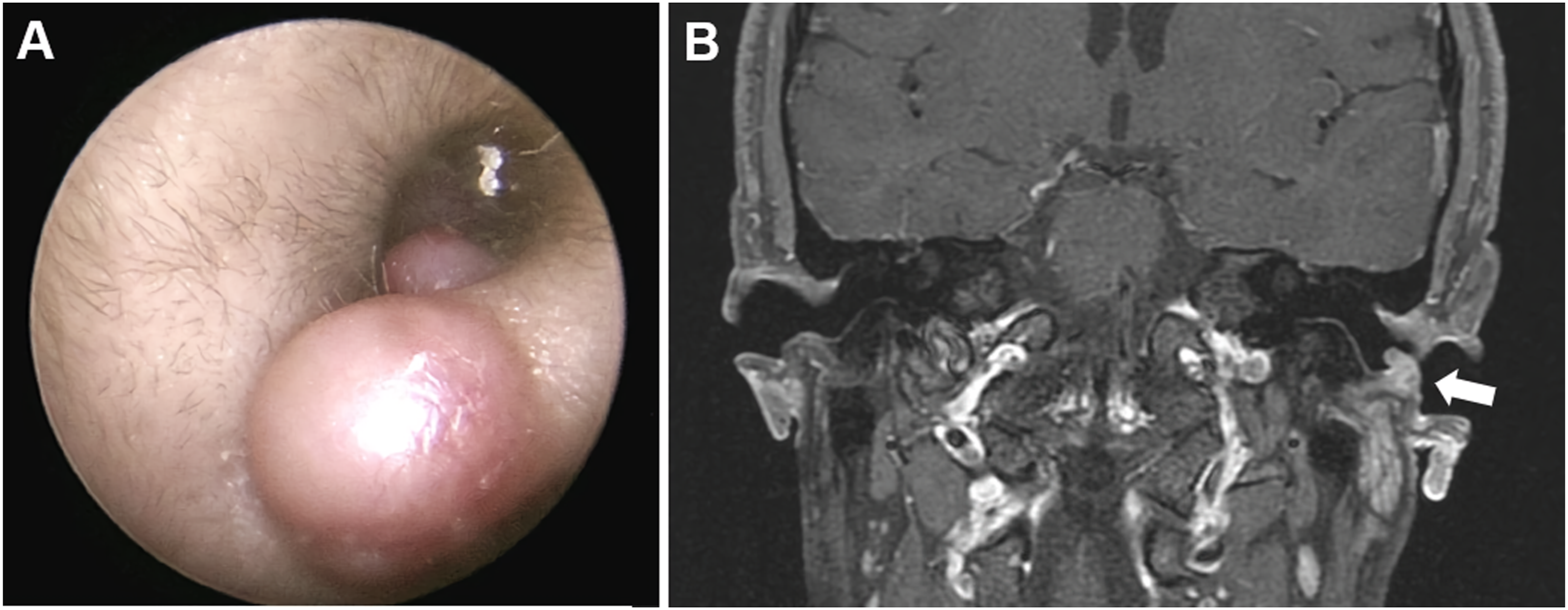
Surgical removal was planned, and the lesions were excised down to the perichondrium under local anesthesia (Figure 2A). The larger defect was sutured to achieve primary closure, and the smaller defect was left to heal by secondary intention. Histological examination revealed small capillary-sized blood vessels confined to the subcutis (Figure 2B). They were infiltrated by chronic inflammatory cells consisting of plasma cells, eosinophils, and lymphocytes (Figure 2C). These findings are consistent with the diagnosis of PG. Postoperative follow-up after 8 weeks revealed uneventful healing. Surgical specimens (A). Histological section reveals small, capillary-sized blood vessels confined to the subcutis (B) and infiltration of plasma cells, eosinophils, and lymphocytes (C).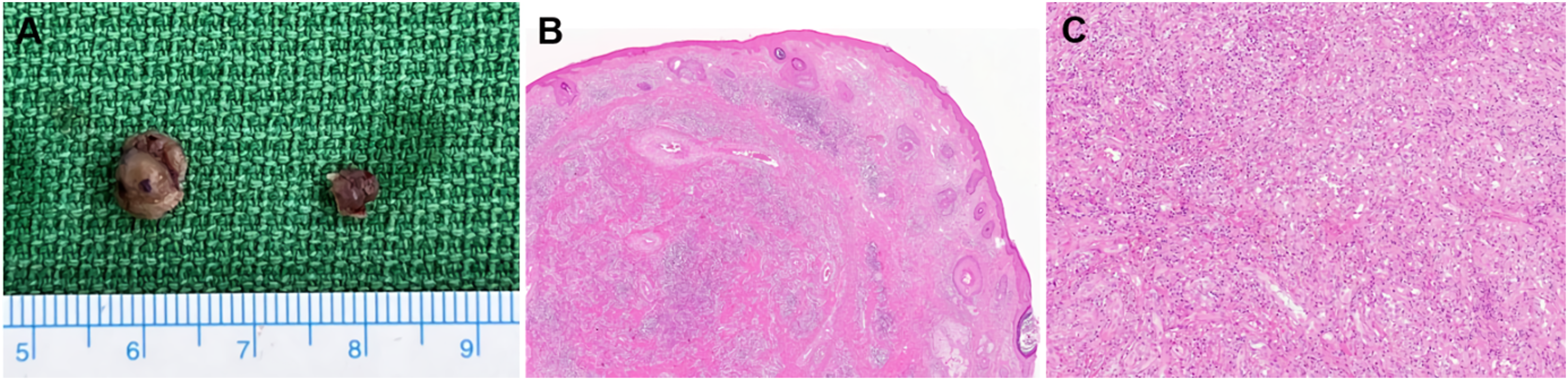
Discussion
Reported Pyogenic Granuloma in the External Auditory Canal.
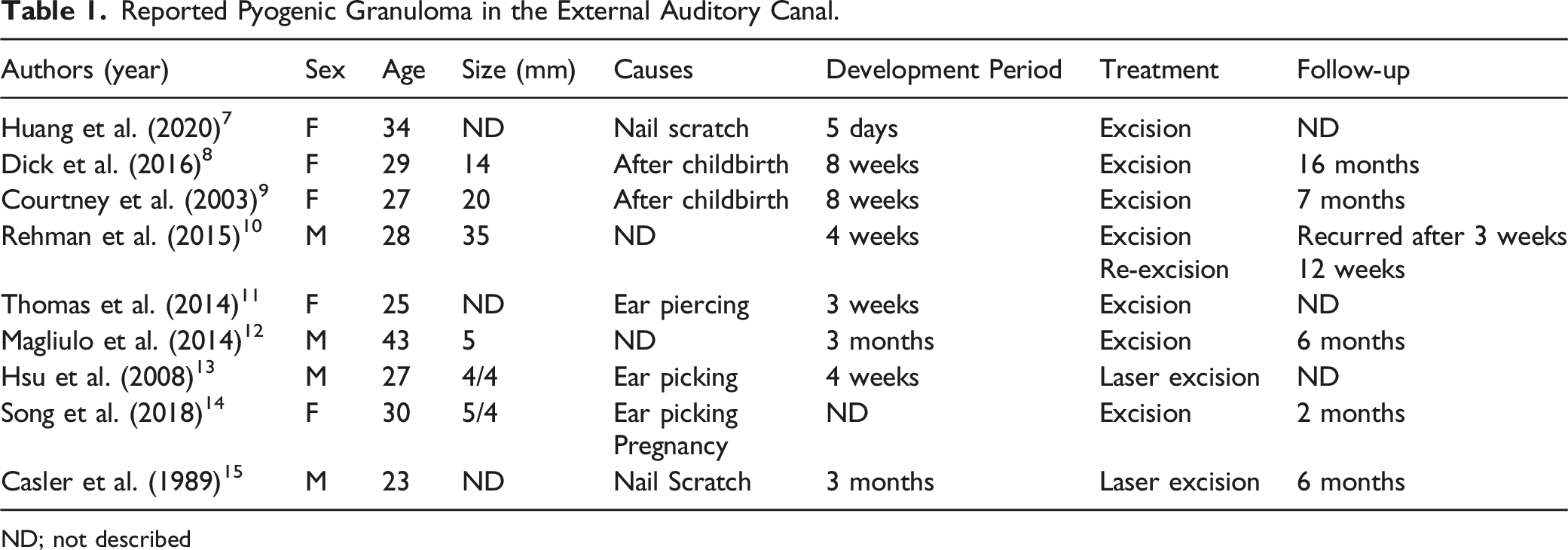
ND; not described
PG is characterized by rapid growth over weeks and months. Although the patient in the present case could not recall its development, all previously reported cases showed rapid lesion growth within 3 months. Its pathogenesis is uncertain, but most hypotheses describe the development of PG as a hyperplastic, neovascular response to an angiogenic stimulus. 1 This is supported by its common development in preexisting vascular lesions and during pregnancy. The effect of female steroid hormones during pregnancy on the pathogenesis of PG has been confirmed through basic research. 16 It was found that hormones increase the expression of angiogenic factors in the inflamed tissue and reduce granuloma cell death to prolong the angiogenic effect. When this angiogenic stimulus disappears after delivery, PG typically recedes spontaneously. 17 However, PG has also been reported to appear following childbirth.7,8 Hormones are thought to play a role in the development of PGs. However, there are individual differences in when, how, and by what they are affected. Trauma is also an important factor and can be classified as acute and mechanical, such as ear piercing; 11 chronic and mild, such as nail scratches;7,15 or simple cotton bud usage.13,14 The cause in this case could be the frequent touching by the patient.
Although some individuals may experience spontaneous regression,18-20 surgical treatment is usually necessary because of frequent bleeding, obstruction, and cosmetic aspects. Various modalities have been utilized to treat PG, including full-thickness excision, shave excision, curettage, laser therapy, and cryotherapy. A review compared the results of 19 treatment methods for 1162 cutaneous PGs. 21 According to this report, surgical excision showed the lowest recurrence rate (2.94%), whereas blunt removal followed by cauterization with silver nitrate showed the highest recurrence rate (15.38%). Recurrence can occur when complete excision is not achieved. The EAC is a difficult structure for surgical access because of its narrow shape and limited amount of soft tissue; thus, there is a high possibility that remnants will remain upon removal of the lesion. A case of recurrence among the EAC lesions has been reported previously. The lesion was a 35-mm large PG that showed immediate recurrence after surgical excision. 10 After the reoperation, in which the lesion was excised down to the perichondrium level, as in the present case, there was no subsequent recurrence. In the external ear, most defects would heal by second-intention if the cartilaginous structures are intact. 22 Therefore, while planning surgical removal of the PG in the EAC, it is recommended to excise the lesion sufficiently down to the perichondrium.
A variety of benign and malignant tumors occur in the EAC; thus, differentiation of these tumors is important. Although it is very rare for PGs to occur in the EAC, it can be suspected in conditions such as after acute and/or chronic trauma, hormonal changes or systemic drug administration, rapid growth, and easy bleeding tendency with a friable surface. Some PGs may spontaneously resolve, but when they cause symptoms, excision is recommended for treatment and diagnosis. In the case of excision, the tumor should be excised down to the perichondrium level to prevent recurrence. Although PG mainly occurs in a solitary form, the present case shows a new clinical variation where multiple PGs were present in the EAC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by a National Research Foundation (NRF) of Korea funded by the Korean government (MSIT) (No. 2022R1F1A1071824) to J.M.L.
Ethical Statement
This study was approved by the Institutional Review Board of the authors’ institute (IRB number: ISPAIK 2022-11-002), and the requirement for informed consent from the patient was waived. A patient’s anonymity is preserved in the manuscript.
Data Availability Statement
The data used to support the findings of the study are included within the article.