
Abstract
Although hemangiomas are common in the head and neck area, they are uncommon in the temporal bone. External auditory canal (EAC) hemangiomas are a relatively uncommon otologic condition. In the English literature, only 29 cases of temporal bone hemangioma have been reported. We also present the case of a 32-year-old male patient who presented with an 8-month history of decreased hearing, tinnitus, and aural fullness on the right side. Otoscopic examination of the right ear revealed a smooth, oval, well-circumscribed, reddish, pulsatile, nontender mass, which was about 1 cm in diameter and occupied two-thirds of the EAC. It was soft in consistency, compressible, and appeared to be arising from the right posterior-superior portion of the bony canal wall; the tympanic membrane seemed to be uninvolved. The patient had mild conductive hearing loss of the right ear with an average air-bone gap of 20 dB; the left side was normal. High-resolution contrast-enhanced computed tomographic scanning of the temporal bone showed well-defined, rounded, homogenously enhancing lesions at the posterior-superior aspect of right EAC measuring 0.7 × 0.8 cm. Angiography was performed and there was evidence of vascular blush in the region of the right EAC. Three blood vessels were identified and embolized. The mass was completely removed by the endaural approach, and a retroauricular skin graft to restore cutaneous integrity was not required. Histopathology indicated a capillary hemangioma without cytological atypia or mitotic activity. There was no recurrence 1 year after the surgery.
Introduction
Hemangiomas are rare benign vascular tumors. They are relatively common in the head and neck and can be divided into capillary, cavernous, or mixed types. They are commonly found on the skin or mucosal surfaces of the oral cavity and nasal cavity during childhood. Children usually develop them at 1 year of age and they involute at 5 or 6 years of age. 1 Capillary hemangiomas are capillary-like channels found in the skin, subcutaneous tissues, lips, liver, spleen, and kidneys. 2
The current International Society for the Study of Vascular Anomalies classification for vascular anomalies includes 2 main categories, namely vascular tumors and vascular malformations (Table 1). 3 The vascular tumors are further classified as 3 subtypes of hemangiomas: benign, locally aggressive, and malignant. Vascular malformations comprise either simple or combined malformations.
Patient Information for Hemangioma of the External Auditory Canal and Temporal Bone and Literature Review and Current Cases.
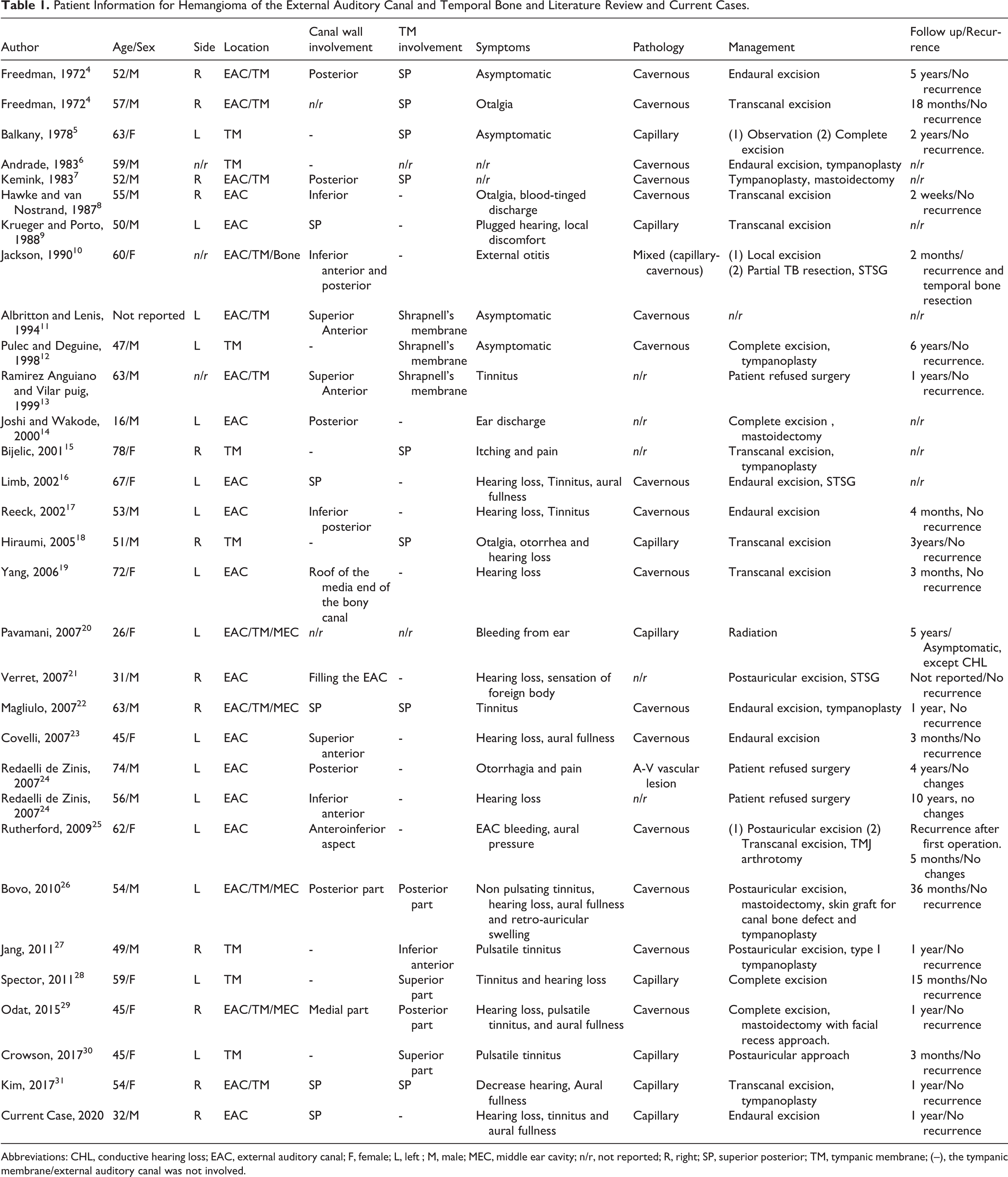
Abbreviations: CHL, conductive hearing loss; EAC, external auditory canal; F, female; L, left ; M, male; MEC, middle ear cavity; n/r, not reported; R, right; SP, superior posterior; TM, tympanic membrane; (–), the tympanic membrane/external auditory canal was not involved.
There has been some misunderstanding in the terminology of vascular lesions in the literature, and the term hemangioma has been used incorrectly to describe what are apparently vascular malformations. 32,33 Although vascular lesions are common in the head and neck, 34 they are uncommon in the temporal bone, where they are typically located inside the internal auditory canal or along the path of the facial nerve, due to the abundant blood supply surrounding the scarpa and geniculate ganglions. 35 Only a few cases of middle and external ear localization have been recorded. 17
We present one case of a vascular lesion of the external auditory canal (EAC) that was treated surgically after embolization, and followed without any sign of recurrence. A discussion of the characteristics of this disorder, based on a review of the pertinent literature, is also presented.
Materials and Methods
This clinical investigation was conducted in accordance and compliance with all statutes, directives, and guidelines of an Internal Review Board and the research performed under the authorization of the Ethics Committee of Ohud Hospital, with appropriate informed consent.
Our review of the English literature was based on a PubMed search from 1972 to 2021 for all cases of the EAC and temporal bone hemangioma (capillary, cavernous, or mixed types, including synonyms), and 29 cases were finally evaluated.
Clinical Case
A 32-year-old male patient presented to our otolaryngology clinic with an 8-month history of progressive decrease in hearing, tinnitus, and aural fullness on the right side with no history of ear discharge, vertigo, trauma, or facial palsy. Otoscopic examination of the right ear revealed a smooth, oval, well-circumscribed, reddish, pulsatile, nontender mass, about 1 cm in diameter, occupying two-thirds of the EAC. It was soft in consistency, compressible, and appeared to be arising from the right posterior-superior portion of the bony canal wall; the tympanic membrane seemed to be uninvolved. Left-sided otoscopy findings were normal. Vestibular examination was normal, and head and neck examination findings were not significant. Weber test at 512 Hz showed bone conduction greater than air conduction, lateralized to the right side in the same ear. Pure-tone audiometry showed mild conductive hearing loss in the right ear with an average air-bone gap of 20 dB; the left side was normal.
High-resolution contrast-enhanced computed tomographic scanning (HR CECT) of the temporal bone showed a well-defined, rounded, homogenously enhancing lesion at the posterior-superior aspect of the right external auditory meatus measuring 0.7 × 0.8 cm. The internal auditory canals were normal in appearance, with normal dimensions and bony boundaries. The semicircular canals, cochlea, and middle ear cavities were normal and no intracranial extension was noted (Figure 1). Magnetic resonance imaging (MRI) of the temporal bone showed a well-defined elongated right EAC lesion measuring 1.2 × 0.6 cm; the lesion appeared homogenous hyperintense on T2, hypointense on T1, and with homogenous enhancement on postcontrast sequence. There were vessels crossing anteriorly to the lesion (Figure 2). Angiography was performed to delineate the blood supply to the mass and embolize any feeding vessels. There was evidence of vascular blush in the region of the right EAC, and 3 blood vessels was identified and embolized.
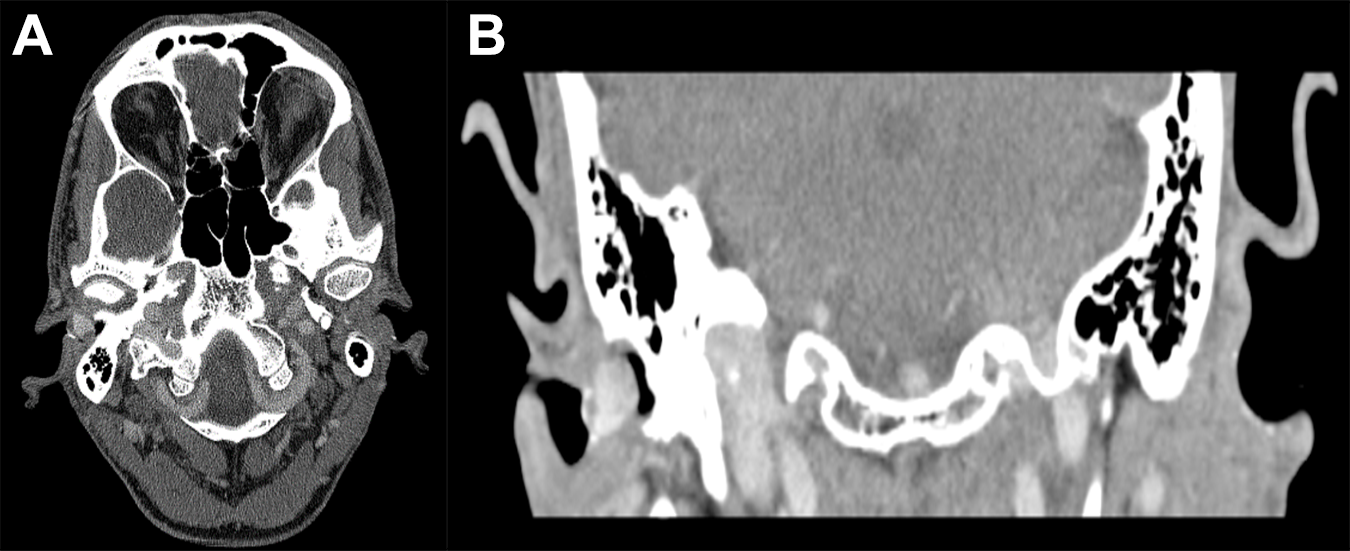
HR CECT of the temporal bone, (A) axial view and (B) coronal view, showing well-defined rounded homogenously enhancing lesion involving right EAC (arrows). EAC indicates external auditory canal; HR CECT, High-resolution contrast-enhanced computed tomographic scanning.
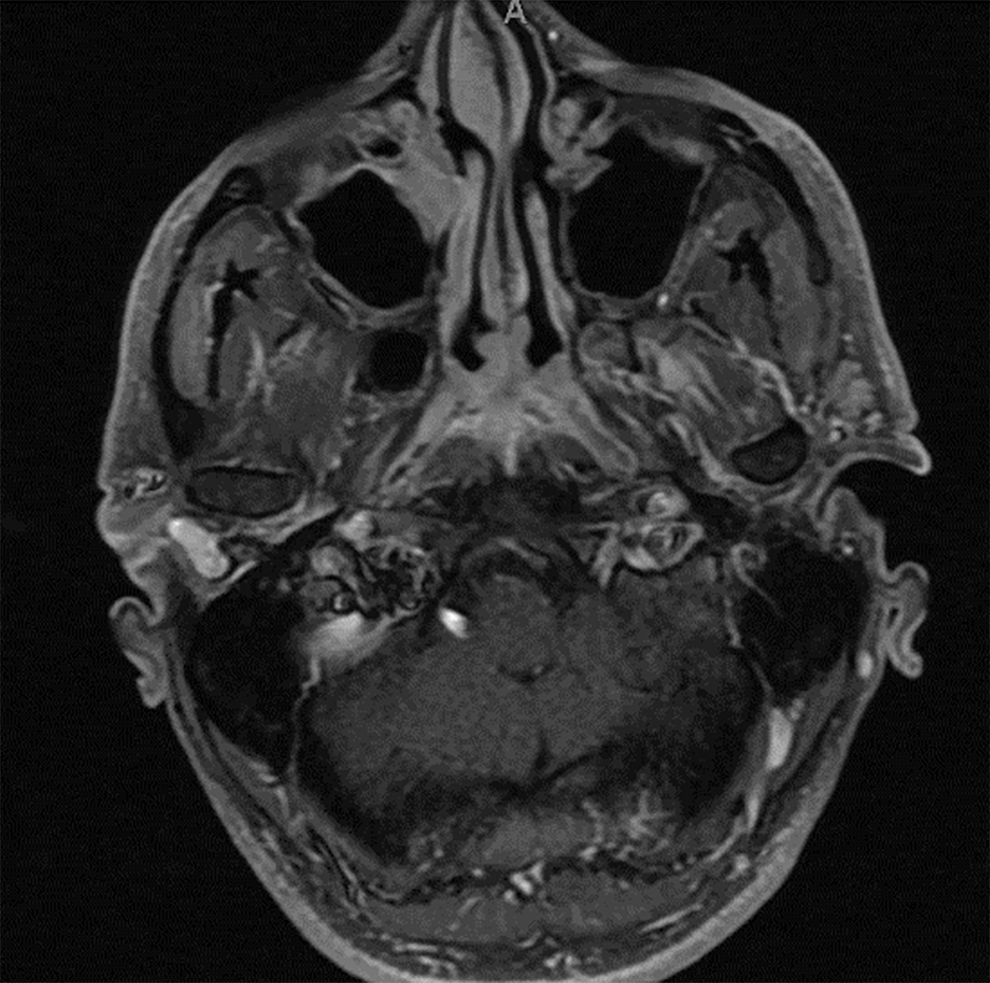
MRI of the temporal bone showed well-defined elongated lesion involving right EAC (arrows). EAC indicates external auditory canal; MRI, magnetic resonance imaging.
The patient was taken to the operating room the morning after embolization for surgical resection of the mass under general anesthesia. The lesion was smoothly excised using the microscope, with an endoaural approach. The mass, based posterior-superiorly in the ear canal and lateral to the annulus, was excised after separating the skin over the lesion. The bone of the EAC was normal in appearance. Bleeding was controlled with cautery. The mass was completely removed without needing a retroauricular skin graft to restore cutaneous integrity.
Histopathologically, the lesion demonstrated keratinized, stratified, squamous epithelium covering dense fibrous, connective tissue. Within this connective tissue, there was a network of numerous variably dilated capillary vessels. There was no cytological atypia or mitotic activity indicative of a capillary hemangioma (Figure 3). The postoperative period was uneventful and there was no recurrence 1 year after surgery.
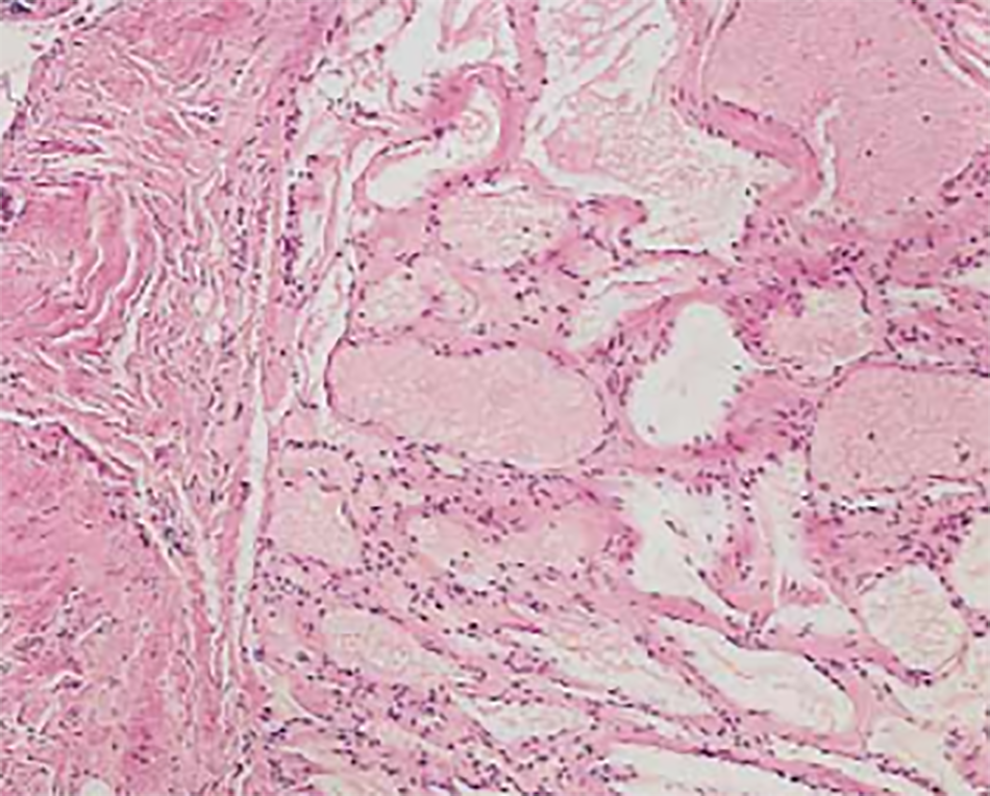
Hemangioma consisting of multiple capillary-sized vessels lined by flattened epithelium (star), inflammatory cells (arrow) (hematoxylin and eosin stain).
Discussion
Hemangiomas of the EAC and/or tympanic membrane are extremely rare and mainly appear between the sixth and seventh decades of life. 22 Males and females are affected in a 2:1 ratio. 26 Based on this clinical series and a review of the cases reported in the English literature, only 29 cases of hemangioma of the EAC and temporal bone have been reported (Table 1). Freedman et al 4 first described 2 cases of cavernous hemangiomas in 1972. One was in a 52-year-old man without symptoms, and the other was in a 57-year-old man with otalgia. Both masses were found on routine examination. Neither patient had significant conductive hearing loss preoperatively. Cavernous hemangiomas were completely excised from the posterior EAC and tympanic membrane in both cases.
Vascular lesions involving the EAC usually originate from the epithelium of the tympanic membrane or from the EAC itself. The patient may be asymptomatic or have multiple symptoms. Conductive hearing loss due to the hemangioma obstructing the EAC is a common symptom, but no studies have mentioned the percentage of hearing loss. According to our literature review, 12 of 31 cases (including our case) present with hearing loss. In addition, faint ear discharge, ear congestion, tinnitus, and earache are common symptoms. Of the 29 patients, 4 patients presented asymptomatically, with abnormalities found only on physical examination. On otoscopy, red or purple blood vessels could be seen in the external auditory meatus. 17,16
Attic cholesteatoma with aural polyp, granulation tissue, intradermal nevus, glomus tympanicum, glomus jugulare, arteriovenous malformation, high jugular bulbus, aberrant internal carotid artery, and carcinoma are also possible differential diagnoses. 17,4,24,23,19,36
When a hemangioma is suspected, high-resolution computed tomography (HRCT) scan of the temporal bone, MRI, and angiography should be performed further.
A temporal bone computed tomography (CT) is the first choice for evaluating the location and size of the lesion and middle ear involvement. Hemangiomas appear to be of the same density as the cerebral parenchyma on CT scans and can produce ossifications. 37 They appear as well-defined masses with limited contrast enhancement that are homogeneous in the proliferative phase and heterogeneous in the involution phase. 38 Preoperative HRCT is the preferred method of radiological assessment because it can reveal the size of the tumor, the presence of bone erosion, and the possibility of ossicular chain involvement. 39 To rule out the existence of a high jugular bulb or an aberrant carotid artery, radiological findings must be carefully reviewed. 40
An angiogram is not usually needed, but it may be helpful in identifying and embolizing any feeding vessels supplying an advanced lesion if severe bleeding is expected. 41
For a definitive diagnosis, a histological examination is needed. Capillary hemangiomas are capillary-like channels caused by a proliferative endothelial process that begin in childhood and disappear before the age of 5, while cavernous hemangiomas are huge cavernous vascular spaces that appear after the sixth decade of life. 42
There are a variety of treatment choices, from watchful waiting to temporal bone resection. Small asymptomatic lesions should be monitored. Balkany et al 5 described a patient who had a lesion that was initially treated by observation in 1978. The lesion doubled in size after 18 months and was excised locally.
The surgical approach is determined by the location and size of the lesion. Small lesions restricted to the external auditory meatus can be removed by a transcanal approach 43 or through an endaural approach like our case, while lesions extending to the middle ear cleft and mastoid need mastoidectomy with tympanoplasty and, in some cases, temporal bone resection. 16 The recurrence rate is relatively high and is dependent on the adequacy of surgical resection. No study mentions the recurrence rate, and according to our literature review, only 2 studies, Jackson 10 and Rutherford, 25 had recurrence.
Aside from surgery, there has been some exciting progress in alternative treatment options. The use of CO2 laser-assisted tumor excision, as defined by Kostrzewa et al, reduced the risk of bleeding and improved visualization. 44 Pavamani et al recorded a 5-year recurrence-free duration after using radiotherapy as the primary treatment of an inoperable capillary hemangioma of the external and middle ear. 20
Conclusion
Hemangiomas in the EAC and/or tympanic membrane are rare but must be considered in the differential diagnosis of EAC and/or tympanic membrane lesions. Audiogram, CT, and tissue biopsy are essential for diagnosis. Options for management are case dependent and can be selected after adequate preoperative evaluation. Surgical excision is still considered the treatment of choice.
Footnotes
Authors’ Note
Consent was obtained for case publication of imaging and pathology materials. All procedures performed in this retrospective data analysis involving human participants were in accordance with the ethical standards of the institutional review board of Ohud Hospital, with appropriate informed consent.
Salamah Marzouqi is now also affiliated with King Abdullah Ear Specialist Center (KAESC), College of Medicine, King Saud University Medical City (KSUMC), King Saud University, Riyadh, Saudi Arabia.
Halawani Roa is now also affiliated with Otolaryngology Consultant, Ohud Hospital, Al-Madinah Al-Munawarah, Kingdom of Saudi Arabia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.