
Abstract
Solitary fibrous tumors (SFTs) originating from the external auditory canal are uncommon; only few cases have been reported in the literature. In this article, we report a case of a 35-year-old man who presented with a 6-month history of a gradual swelling in the entrance of the left external auditory meatus associated with hearing loss. The tumor was surgically removed, and histological examination showed spindle-cell proliferation with a collagenous stroma. Immunohistochemically, the tumor cells were positive for CD34 confirming the diagnosis of an SFT. Although SFTs are benign, complications such as relapses and metastasis after excision were reported. Thus, a careful and long follow-up is recommended.
Introduction
Solitary fibrous tumors (SFTs) are rare spindle cell tumors that were initially described as tumors originating from the pleura. However, it has been documented that SFT could exist in multiple extrapleural sites.
The external auditory canal is a rare location for the SFT with only a few cases reported in the literature.1-5
Diagnosis has been confirmed on the basis of the histopathological findings and the tumor cells positivity for CD34 antibodies. 6
In this study, we present an additional case of an SFT arising from the left external auditory canal.
Case Report
A 35-year-old man, with no prior medical history, presented with a swelling in the entrance of the left external auditory meatus and hearing loss. The symptoms steadily increased over a 6-month period. Physical examination revealed a pale and firm mass located in the superior wall of left external auditory canal (Figure 1).
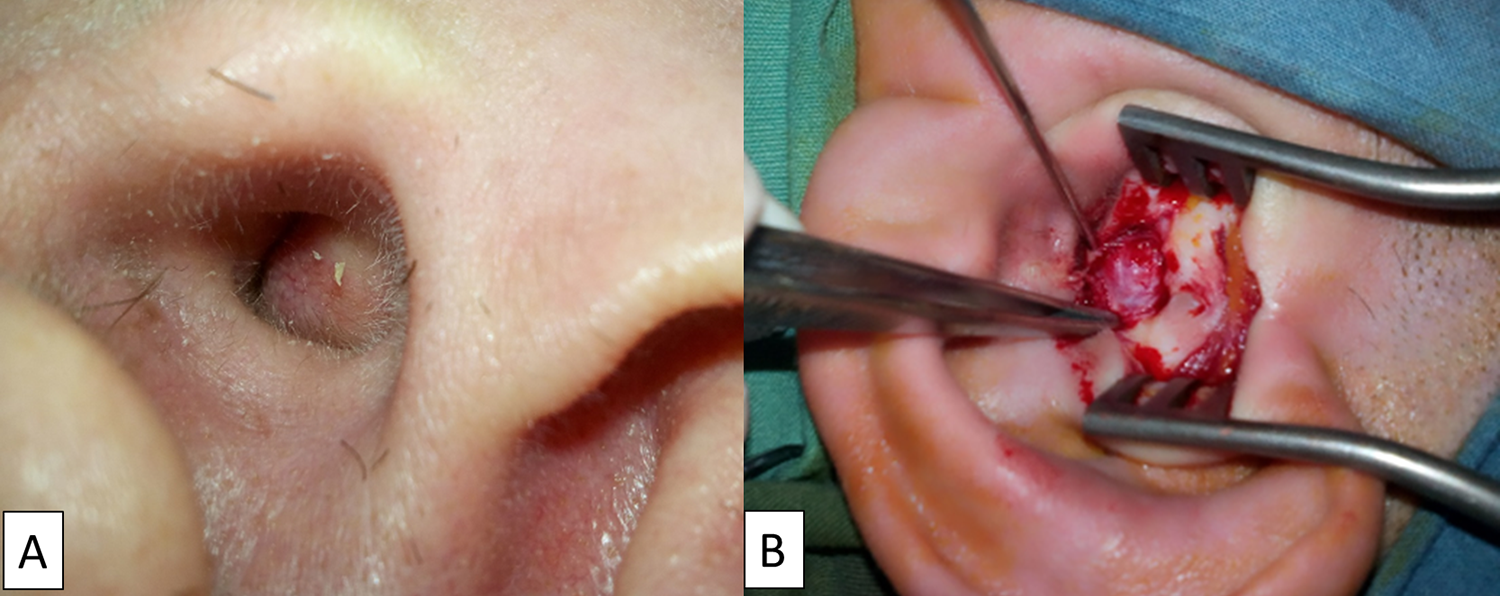
Rounded formation obstructing the left external auditory canal originating from the upper wall of the canal (A) preoperative (B) per operative.
The audiogram showed a slight conductive impairment due to the obstruction caused by the tumor.
A computed tomography (CT) scan of the temporal bone revealed a well-circumscribed soft tissue mass narrowing most of the external auditory canal (Figure 2). The mass originated from the superior wall of the cartilaginous portion of the external auditory canal with no bone erosion.

A computed tomography scan of left ear (axial section): a homogeneous, low-density mass without any definable invasion into the adjacent structures.
Magnetic resonance imaging (MRI) showed a well-defined tumor measuring 20 × 15 × 13, 5 mm with homogeneous enhancement after gadolinium injection. The mass was hypointense on T2-weighted sequence (Figure 3).
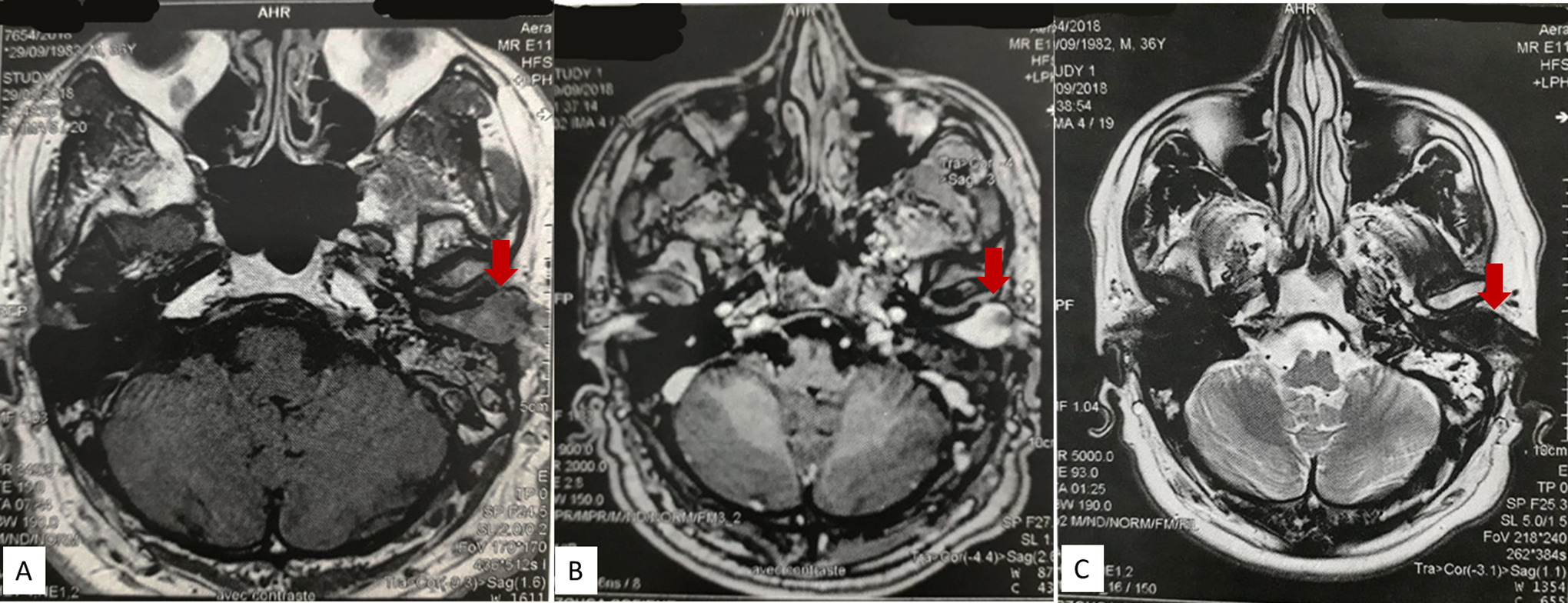
Magnetic resonance imaging scan of ears on axial section: circumscribed formation of the left external auditory canal which measures 20 × 15 × 13.5 mm. It has an intermediate signal in T1-weighted sequence (A), a strong homogeneous enhancement after injection of gadolinium (B), and a T2 hyposignal (C).
The patient underwent surgery under general anesthesia. The tumor was easily removed via the meatus since it did not have any adhesions to the surrounding tissue. The epidermis between the tympanic membrane and the tumor was removed. Postoperative follow-up was simple and uneventful.
The surgical specimen consisting of a firm cartilaginous homogenous mass measured 20 × 15 × 15 mm. On the cut surface, the tumor exhibited a white color and fascicules without any hemorrhagic or necrotic zones.
The microscopic examination revealed a nonencapsulated but well-circumscribed tumor, composed of spindle cells and a focal hypercellular zone. No significant cytologic atypia, necrosis, or mitotic activity was identified.
Immunophenotypically, the tumor cells were positive for CD34, vimentin, CD99, and Bcl-2, and negative for s100, desmin, actin HHF35, and actin 1A4 (Figure 4).
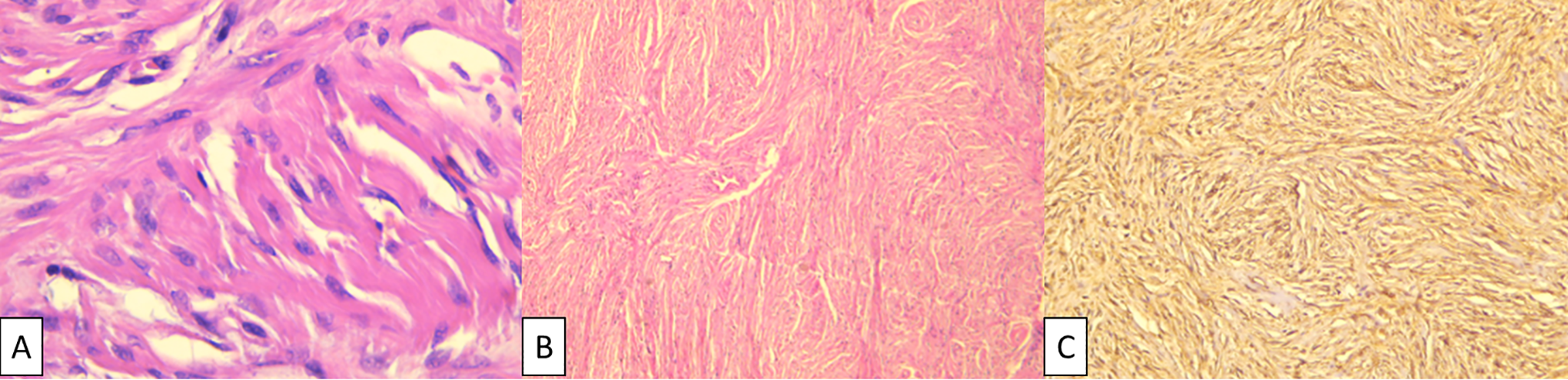
A, Fibroblastic cells with no atypia or mitosis HEx400. B, Moderately cellular fibroblastic tumor with whorled pattern hematoxylin Eosin 40. C, Positive immunostaining for CD34.
Based on these morphologic findings and immunophenotype, the final diagnosis of solitary fibrous tumor was confirmed. During 2-year follow-up care, our patient had no recurrence.
Discussion
Solitary fibrous tumors are uncommon mesenchymal neoplasms typically described in the pleura. Although SFTs are not frequently observed in extrapleural sites, they have been reported to be found in multiple locations of the human body. 7 Yet, to the best of our knowledge, the external auditory canal location was reported only 5 times in the literature.1-5
Generally, SFTs are slow-growing tumors that occur mainly in the fourth and fifth decades of life. However, rare cases have been reported in children and adolescents. 6
No sex predominance was observed, although some studies have reported slight female predilection. 6 This tumor, previously known as solitary mesothelioma, was thought to be of mesothelial origin, but the identification of SFT in extra serosal locations along with its ultrastructural and immunophenotypic features demonstrated that SFT had a mesenchymal rather than mesothelial origin. 7
Solitary fibrous tumors manifest as benign lesions in most cases; however, they demonstrate aggressive behavior with local recurrence and metastasis up to several years after surgical removal. 8
Extrapleural SFTs, which have higher risk of recurrence, are classified according to 2013 World Health Organization classification of bones and soft tissue neoplasms as a fibroblastic or myofibroblastic neoplasm with intermediate, rarely metastasizing biological behavior. 6
Prognostic evaluation has been conducted using a risk stratification model. Factors associated with an increased risk of metastasis and poor outcome are larger tumor size (≥15 cm), increased mitotic figures (≥4/10 high-power fields), and the patient’s age (≥55 years). 9
The tumors measuring more than 5 cm are not an indication for surgical excision.
Factors associated with poor prognosis in head and neck SFT are poor pathological differentiation, deep tumor location, and nonsurgical treatment. 10
Total resection was performed and none of the adverse prognostic factors were observed in our case.
The macroscopic presentation of our patient’s tumor corresponded to the classical description found in previous studies: firm, well-circumscribed, and gray-whitish.
On histological examination, this tumor is characterized by patternless proliferation of generally banal oval to spindle cells with hemangiopericytoma-like staghorn vessels in fibro collagenous stroma. 6
Tumor cells are positive for CD34, vimentin, and Bcl-2, and negative for S-100 protein, smooth muscle actin, desmin, and cytokeratin. 6 However, these immunohistochemical markers are nonspecific and can be detected in multiple other neoplasms. 8
On the other hand, STAT6 nuclear immunoreactivity, which is the consequence of NAB2-STAT6 fusion, is the most useful diagnostic marker for SFT. Sensitivity and specificity have been reported to be 86% to 100% and 96% to 100%, respectively. 6
Unenhanced CT images revealed larger SFT which had the same density as muscles and some contained hypodense areas representing necrotic, myxoid, or cystic formations. In MRI, the hypo signal with T2 weighted aspect of the lesions was attributed to hypercellularity and abundant collagenous stroma. The hyper signal images represented necrotic, myxoid, or cystic changes. Enhanced CT or MRI revealed mild to marked heterogeneous contrast uptake correlating with hypocellularity or hypervascular areas. 6
The treatment of these tumors is based on surgical resection. Despite adequate tumor-free resection margins, local recurrence and distant metastasis can occur. Consequently, long-term follow-up with serial cross-sectional imaging is recommended, as late recurrences have been reported (>10 years). 8 None of the cases previously reported about SFT in the external auditory canal showed aggressive behavior.1-5
Conclusion
We have reported a case of a solitary fibrous tumor of the auditory canal, which is presumably a rare location. Immunohistochemical analysis can provide insight into the diagnosis of this tumor.
Long-term follow-up of patients with SFT is recommended due to the risk of recurrence and metastasis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.