
Abstract
Solitary fibrous tumor (SFT) is an uncommon spindle cell neoplasm, which generally arises from the pleura. There have been documented a number of extrapleural origins including the head and neck in the literature. It is emphasized to make a diagnosis in a rare location such as the retropharyngeal space. We present a case of a 54-year-old man diagnosed with giant solitary retropharyngeal SFT. Clinical symptoms were pharyngeal foreign body sensation and dysphagia associated with dyspnea. Physical examination showed a sizable submucosal mass under the posterior pharyngeal wall, which partially obstructed the upper aerodigestive tract. With radiologic images to evaluate the dimension and relationship with surrounding structures, the tumor was surgically removed en bloc via a transcervical approach. The histology and immunohistochemistry play a crucial role in differential diagnosis. Complete surgical excision is an alternative and curative strategy.
Introduction
Solitary fibrous tumor (SFT) is rare and first described in 1931, 1 and it is estimated to occur with a frequency of 2.8 per 100,000 individuals. 2 Traditionally, SFT originates from the pleura, lung, mediastinum, and pericardium, and uncommon sites including head and neck have been identified in previous literature. It occurs with equal frequency in adults of both sexes, among which 23% may be aggressive. 3 As the natural evolution of slow growth and no characteristic symptoms in the early stage, especially arising from retropharyngeal space, it is quite difficult to make a diagnosis in such a scarce site. Only 5 cases of retropharyngeal SFT have been documented in the literature.4-8 Herein we present a patient of giant solitary retropharyngeal SFT with a maximum diameter of about 15 cm, which was surgically removed en bloc via transcervical approach. Written informed consent for the publication was obtained from the patient.
Case Presentation
In March 2021, a 54-year-old man complaining of dysphagia and dyspnea for 6 months was referred to our department. Also, he felt a sore throat occasionally and severe foreign body sensations when swallowing. Such symptoms became aggravated ever since. Initial physical examination showed extensive swelling of the posterior wall of the pharynx, and the pharyngeal cavity became quite narrow. Through palpation, a sizable symmetric neck mass in the deep plane beneath the sternocleidomastoid muscle (SCM) was found, from the submandibular region to the level of the supraclavicular region. The tension of the skin was remarkable. Though the glottic region was pushed anteriorly and the airway was obstructed partially by the tumor, the bilateral vocal cord was found to present normal mobility under the fibroendoscope. Ultrasonography presented a large low-echo level mass around the trachea region, 11.5 × 4.9 cm on the left side and 9.8 × 3.8 cm on the right side with a clear boundary. Ultrasound-guided core needle puncture biopsy was performed, and it turned out to be SFT. A contrast cervical computed tomography (CT) scan revealed an extensive soft tissue density with enhancement in retropharyngeal space extending from the plane of the soft palate to the aortic arch, with a vertical extent of about 15 cm. The neoformation displaced the SCM and cervical carotid sheath laterally. The right jugular vein was compressed and partially obliterated. The larynx, trachea, and esophagus appeared displaced anteriorly (Figure 1). No significant cervical lymphadenopathy was demonstrated.
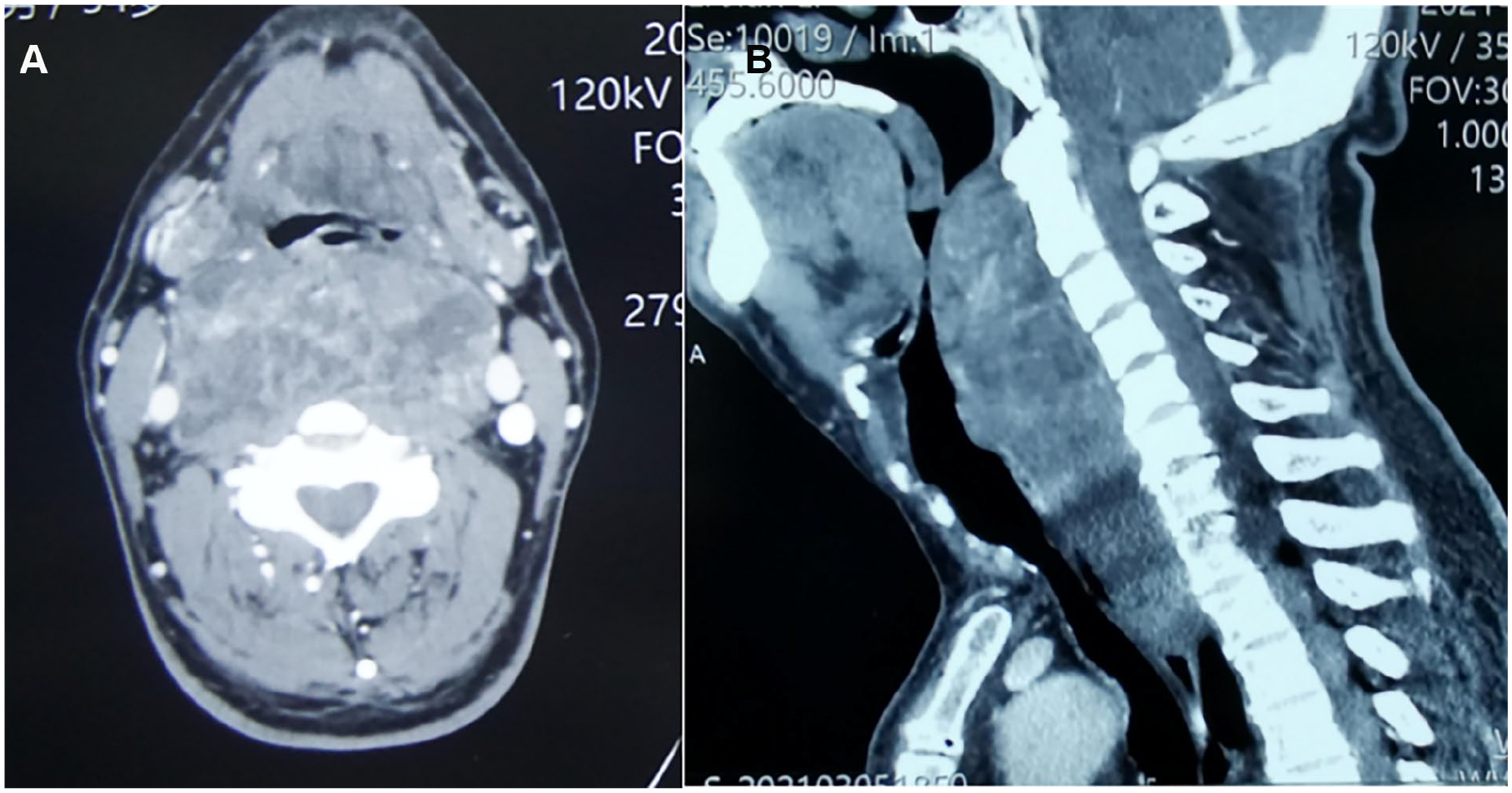
Axial (A) and sagittal (B) contrast computed tomography scan of the neck revealed an extensive soft tissue density with enhancement in retropharyngeal space, the oropharyngeal space became quite narrow. The right jugular vein was compressed and partially obliterated.
For the reason for the narrowness of the upper aerodigestive tract, the anesthesiologist was unable to intubate, tracheotomy was performed under local anesthesia, and the tumor was removed radically under general anesthesia. Considering the resectability and extension of the tumor, bilateral cervicotomy along the posterior border of the SCM was applied. As the subplatysmal flap was elevated and the bilateral cervical carotid sheath was dissected, the tumor with an apparent capsule and well blood supply was directly visible (Figure 2A). Through gentle retraction of adjacent structures, it was easy to detach and deliver the tumor by combining sharp and blunt dissection. With meticulous and precise hemostasis, the tumor was resected en bloc with preservation of cervical vessels, thyroid gland, recurrent laryngeal nerve, and esophagus (Figure 2B). The specimen, grossly measured 15 × 10 × 5 cm, was intact and circumscribed with a smooth capsule. The cut surface revealed a pale and grayish-white mass with scattered nodules.
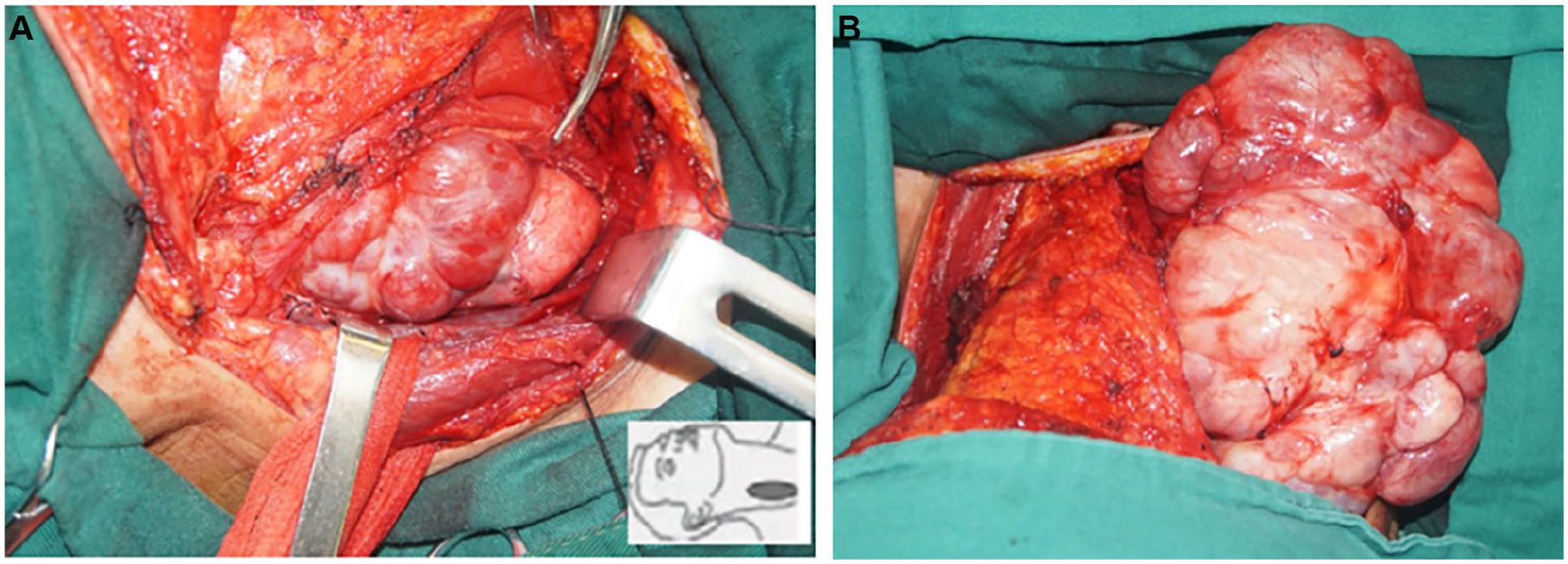
(A) The surgical vision and exposure of SFT. (B) The tumor was completely delivered from the retropharyngeal space. SFT, solitary fibrous tumor.
The patient suffered from mild postoperative aspiration pneumonia and was cured through continuous nasal-gastric tube feeding and effective antibiotic treatment. Seven days later, decannulation was performed and the patient was discharged with a complete resolution.
Microscopically, the tumor was composed of tubercular spindle-shaped cells, mixed with various cellular density and hyalinized vascular walls. The immunohistochemistry was Vimentin(+++), CD34(+++), CD31(+), Bcl2(++), STAT6(++), Ki67 (2%), SMA(−), EMA(−), and S-100(−) (Figure3). It was consistent with the preoperative diagnosis of SFT.
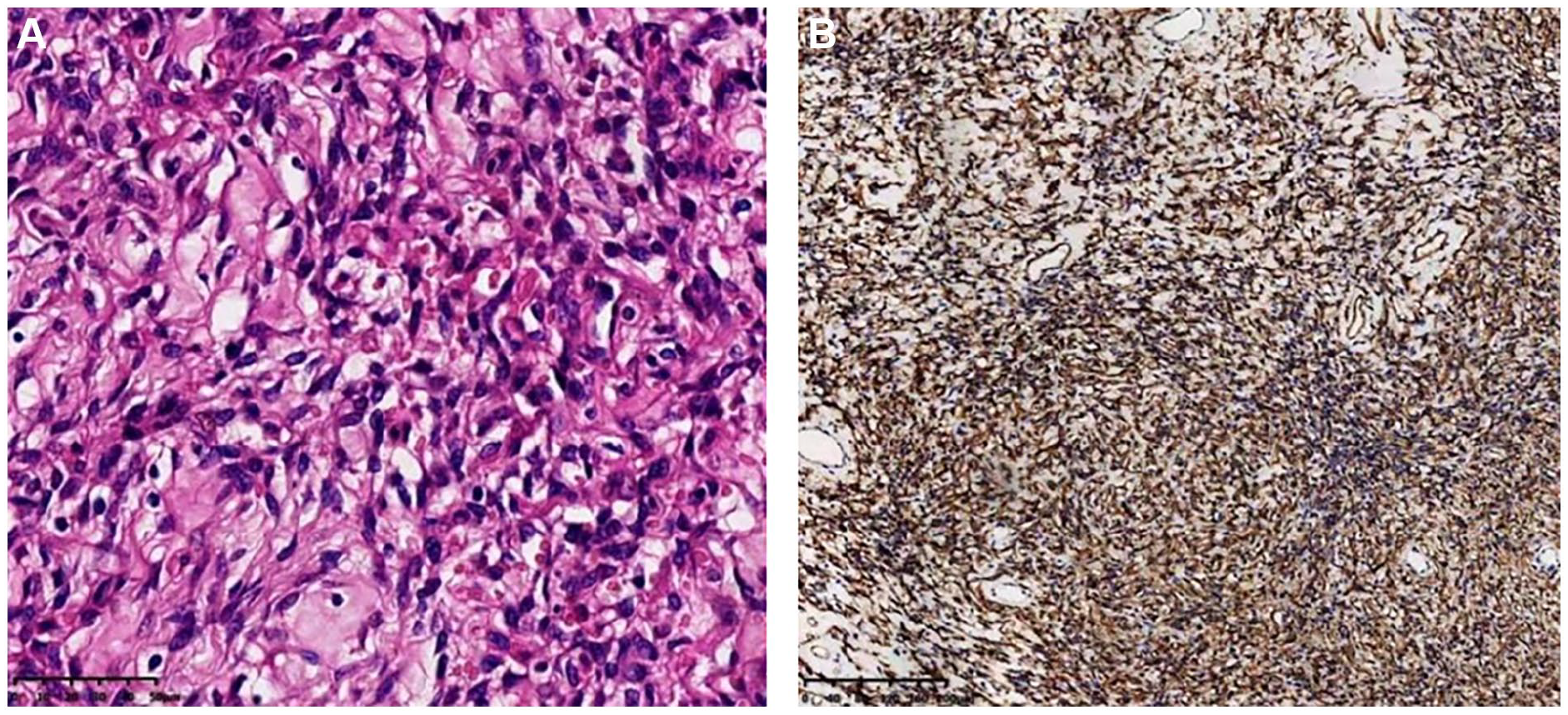
Photomicrographs of the SFT. (A) Tubercular spindle-shaped cell tumor, mixed with various cellular density and hyalinized vascular walls (hematoxylin–eosin stain ×40). (B) Positive reaction to CD34 immunohistochemical stain (×10). SFT, solitary fibrous tumor.
The patient received a periodical follow-up. The endoscope revealed a spacious pharyngeal cavity. There was no clinical evidence of recurrence 3 years after surgery.
Discussion
SFT is a histologic fibroblastic mesenchymal neoplasm. Although it is commonly thought to be intrapleural tumors, 50% to 70% of SFTs are reported outside the pleura. 9 SFT may occur at any age but most in the 15 to 70 years old, with no difference of sexes. The histogenesis is still uncertain. Approximately 20% of SFTs occur in the head and neck area, the most often localizations are the nasal and oral cavities. 10 SFTs in retropharyngeal space are extremely rare, there have been only 5 cases reported in English literature4-8 (Table 1). SFTs are usually asymptomatic and present as a slow-growing painless mass, which is strongly associated with the primary site. Nevertheless, some patients have local compressive symptoms as the tumor grows. According to the reported cases, dyspnea and dysphagia appear to be the most common symptoms, especially when the tumors have reached a quite considerable dimension.
Literature Summary of Cases of SFT in Retropharyngeal Space.
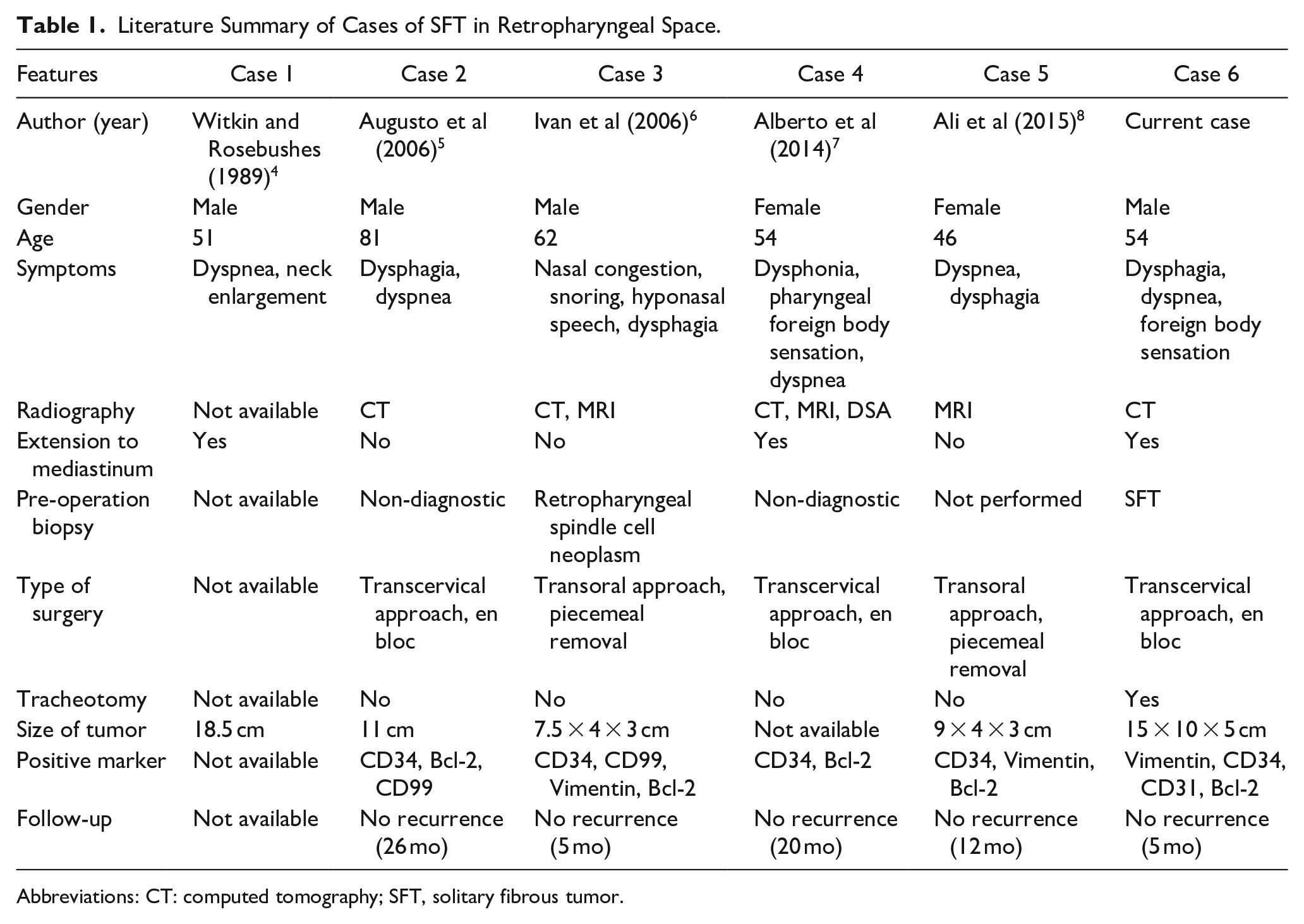
Abbreviations: CT: computed tomography; SFT, solitary fibrous tumor.
The diagnosis of SFT may be primarily considered based on clinical examinations and radiography. Most SFTs present as a well-circumscribe, lobulated mass with a tan-pink surface. SFTs of the head and neck mainly present as a solitary well-defined enhancing mass which is isointense to muscle on non-contrast studies. Most SFTs are isointense to the brain on contrast T1-weighted and T2-weighted MRI sequences. 2 Adjacent bone destruction may be seen for long-standing pressure, which is presented as regressive bony remodeling, while it is not evidence of malignancy.9,10 To exclude Schwannoma, paraganglioma, and hemangiopericytoma, enhanced MRI is particularly profitable. Although there are no distinctive features on CT or MRI, a well-defined homogenously enhancing lesion may be suggestive of the diagnosis. Ganly et al 9 collected and analyzed preoperative radiography of 8 patients diagnosed as SFTs of the head and neck. They found homogeneous enhancement was reliable for a differential diagnosis.
Fine-needle aspiration biopsy is inadequate and not commonly recommended. In most clinical cases, core needle puncture is valuable to establish a diagnosis of SFT, just as in this present case. However, the limited sample provided by core biopsy is not accurate to exclude a high risk of aggressive behavior. Complete resection for histopathologic evaluation is required for a definite diagnosis.
Macroscopically SFT is firm, compact, and richly vascularized, generally with a smooth and glistening surface. Histologically, SFT is well circumscribed with non-encapsulated, composed of numerous proliferated spindle cells arranged in a collagenous background with variable vascularity, which is found to coexist with areas of diffuse hyalinization. It is reported there are 2 fundamental architectural types according to cellular and stromal fibrous components: the solid spindle type and the diffuse sclerosis type. Both types can be found in all tumors with varying proportions. Mostly the tumor does not present aggressive characteristics, including atypia, hypercellularity, increased mitosis rate, infiltrative margins, necrosis, and hemorrhage. 11 England et al 12 reported that most malignancies tended to be a larger mass, 10 cm or more in diameter, with mitotic counts of 4 or more per 10 high-power fields.
Immunohistochemical study makes a significant contribution in distinguishing SFT from other soft tissue tumors. It is demonstrated that SFT generally presents an intense positive immunoreactivity of the spindle cells with CD34 antigen (80%-95%)and CD99 (70%), less commonly it expresses Bcl-2, epithelial membrane antigen, and smooth muscle actin (20%-35%).11,13 The characteristics of immunohistochemical reaction help to exclude the diagnosis of other soft tissue tumors, such as hemangiopericytoma, myofibroma, fibrosarcoma, and neurogenic tumors. Nevertheless, it is difficult to distinguish SFT from hemangiopericytoma. Hemangiopericytoma presents more homogenous areas, decreased hyalinization, and negative reaction with CD99 and Bcl-2. It is reported that these 2 neoplasms may represent continuous anatomopathologic periods.13,14
Most SFTs behave in a benign fashion, while malignant behavior has been reported occasionally. Complete resection with free margin is the most important prognostic factor for SFT, while it is of great importance to preserve the vital surrounding structures. Local recurrence may correlate with malignant histologic features and incomplete microscopic margin. Routes of access for neoplasms in the retropharyngeal space include a transcervical approach and a transoral approach. Although the SFTs in retropharyngeal space can extend to the mediastinum, sternotomy or thoracotomy are unnecessary, because the well-defined boundaries and intact capsule facilitate the complete isolation of tumor in the mediastinum into the neck. The transoral approach is beneficial for better cosmetic effects and relatively shorter recovery time but supplies limited exposure. This approach is adopted in 2 cases of these 6 retropharyngeal SFTs with the strategy of central debulking and piecemeal removal. A transcervical approach is helpful to remove the tumor radically and preserve surrounding vital structures, though with an obvious cicatrization. According to the general conditions and perioperative risks, tracheotomy is selective. Considering the difficulty of intubation, we performed tracheotomy preoperation for this patient.
Generally, the diagnosis of SFT should be considered based on the clinical features, while an accurate diagnosis requires immunohistochemical confirmation. Complete surgical resection with a negative margin is the therapeutic management of localized SFTs, the adjuvant or neoadjuvant radiation may be profitable in the context of multidisciplinary discussion. 10 Also radiation therapy and chemotherapy can provide local tumor control in those patients with unresectable or progressive SFTs. For all the patients of SFT, careful long-term surveillance is essential, given cases of very late recurrences. 11
Conclusion
The medical histology and immunohistochemistry play a crucial role in differential diagnosis. Complete surgical excision is an alternative and curative strategy, which is essential to prognosis and reduction of the possibility of recurrence.
Footnotes
Author Contributions
B.D.: collected the data; contributed data or analysis tools; performed the analysis; wrote the paper; F.W. and E.Z.: conceived and designed the analysis; contributed data or analysis tools; performed the analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Scientific Research Seed Fund of Peking University First Hospital (Grant Number: 2023SF30).
Informed Consent
The written informed consent has been obtained from the patient for the publication of this case report.