
Abstract
Solitary fibrous tumor of the pleura (SFTP) is a rare disease, and most published case reports are in patients over 40 years old. We report a case of SFTP in a 22-year-old woman. The imaging features were observed using contrast-enhanced computed tomography (CT), and histomorphological features were evaluated using pathology and immunohistochemistry. The CT showed a mass in the pleura inside the ninth rib on the left. Pathological results of percutaneous puncture in the chest suggested the possibility of solitary fibroma. The patient underwent surgical resection, and the tumor measured 2.5 × 1.5 × 1.5 cm with an intact capsule. Pathological examination revealed a spindle cell tumor, and immunohistochemistry showed strong positive staining for CD34 and STAT6, consistent with typical solitary fibroma. Although SFTP is rare in young patients, early diagnosis and intervention are needed to avoid the possibility of future complications.
Keywords
Introduction
Solitary fibrous tumor of the pleura (SFTP) is a rare disease that accounts for approximately 5% of pleural tumors. 1 Immunohistochemical evidence indicates that it originates from mesenchymal cells in the submesothelial tissue of the pleura, which is a multifunctional tissue. 2 Patients mostly present with respiratory symptoms such as cough, chest pain, and dyspnea in clinical practice. SFTP is more common in individuals over the age of 40, and many papers have described detailed clinical characteristics of patients with SFTP.3,4 However, case reports on young people are very rare. This report describes a 22-year-old woman with SFTP.
Case presentation
In December 2019, a 22-year-old woman weighing 68 kg came to Qingdao University Affiliated Hospital for a routine physical examination. Contrast-enhanced computed tomography (CT) showed a dense shadow of a mound-like soft tissue in the left ninth costal medial pleura, approximately 2.5 × 1.6 cm, with clear borders and significantly unevenly enhancement, with no obvious destruction of adjacent bone. Neither mediastinal lymphadenopathy nor pleural effusion was observed (Figure 1). The patient’s lung function was normal, and she had no other chest complaints, such as cough, bloody sputum, or chest pain. Her blood results showed no abnormalities except for a slight increase in cholinesterase. Ultrasound examinations of thyroid, digestive, and urinary systems and electrocardiogram were normal. The patient denied any history of previous major diseases.
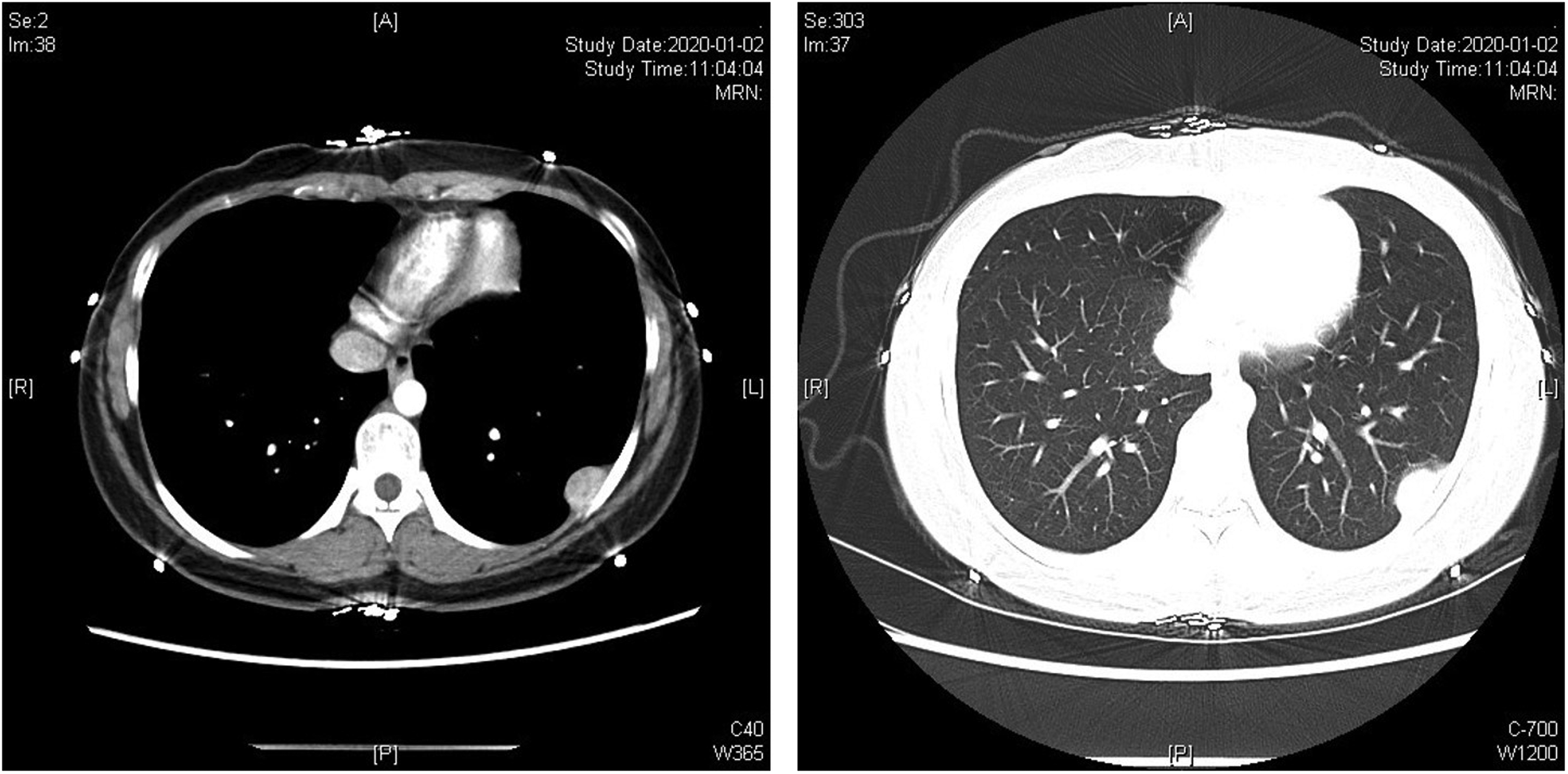
Contrast-enhanced computed tomography showed a dense mass on the left pleura, approximately 2.5 × 1.6 cm in size, with clear borders and with no obvious destruction of adjacent bone. The left panel shows the mediastinal window (showing chest wall and pleura) and the right panel shows the lung window (showing lung tissue in detail, including areas of consolidation and pulmonary vascular structures).
A CT-guided transthoracic core needle biopsy demonstrated SFTP with proliferation of fibrous connective tissue, tumor cells distributed in nests, and no necrosis. Pathological results of percutaneous puncture in the chest suggested the possibility of solitary fibroma.
The patient underwent thoracoscopic surgery. The mass was 2.5 × 1.5 × 1.5 cm and composed of gray-white nodules with a soft texture and complete envelope on the surface. Postoperative histopathological features included spindle cells with mild atypia, <4 mitoses per 10 high-power fields, vascular hyperplasia, and collagenous stroma (Figure 2). Immunohistochemical analysis revealed that the tumor cells were strongly positive for CD34 (Figure 2) and STAT6 (Figure 2), and negative for S-100, ETS-related gene (ERG), SRY box 10 (SOX10), smooth muscle actin (SMA), desmin, cytokeratin (CK), and epithelial membrane antigen (EMA). Approximately 5% of cells were positive for Ki67 (Figure 2). The above results were consistent with solitary fibrous tumor of the pleura.

Microscopic specimen of the tumor showed spindle cells with mild atypia, vascular hyperplasia, and collagenous stroma (top left; hematoxylin and eosin, 200×). Immunohistochemical results showed strong positive staining for CD34 (top right) and STAT6 (bottom left) in tumor cells (diaminobenzidene, 200×). Approximately 5% of cells were positive for Ki67 (bottom right).
Discussion
Solitary fibrous tumor is a rare mesenchymal spindle cell neoplasm usually originating from the pleura. It was first described by Klemperer and Rabin in 1931 (republished in 1992). 5 Most solitary fibrous tumors of the pleura are benign. Patients in previous case reports have usually been middle-aged or elderly, and they present because of respiratory symptoms caused by the enlarged tumor compressing the surrounding tissue.6–11 A small number of solitary fibroma cases occur in younger patients; their tumors are small and they usually have no or very slight clinical symptoms that can be easily missed. Thus, these cases are usually discovered on routine physical examination, as in our case in a 22-year-old female patient. However, it is important to pay close attention to younger patients with pleural nodules suspected to be SFTP because of the risk of serious complications in the future. Regular examination by CT and observation of clinical symptoms are important. If a nodule grows rapidly and invades surrounding tissues or if the patient has corresponding clinical symptoms, such as coughing, further pathological and immunohistochemical diagnosis and treatment should be considered. In contrast, if the nodule is indolent and grows slowly and the patient has no relevant clinical symptoms, follow-up monitoring can be considered. Approximately 12% of SFTP are malignant and carry a risk of invasion or metastasis; in these cases, timely intervention is needed. 12 Although larger tumors are more likely to be malignant, the size of the tumor alone does not predict malignancy, as noted in 2003 by Akisue et al. 13
SFTP is often misdiagnosed because the disease lacks obvious clinical features, imaging findings are often nonspecific, and knowledge of this diagnosis among medical professionals is lacking. Effective diagnosis of SFTP depends mainly on imaging results, pathological examination, and immunohistochemistry. A chest CT usually shows an isolated mass in the chest cavity, with a clear, smooth boundary and a dense interior, with mostly mild to moderate enhancement. Histopathologically, spindle-shaped tumor cells and occasionally nucleoli and mitotic figures are observed. In large tumors, focal necrosis, cystic changes, and a small amount of bleeding may be observed. Malignant tumors may have increased mitotic activity (>4 mitoses per 10 high-power fields), necrosis, hemorrhage, infiltrative margins, and positive expression of p53. 14 Immunohistochemically, SFTP stains positive for CD34, which is an important diagnostic marker that plays an important role in distinguishing SFTP from mesotheliomas and other sarcomatous lesions. STAT6 is a specific marker for solitary fibroma, whereas SMA and desmin are common in myogenic tumors and S100 and SOX100 are common in neurogenic tumors.15,16 It is not easy to make a clear diagnosis of SFTP before surgery. At present, although histological and immunohistochemical analysis of materials obtained by transthoracic needle biopsy is a reliable preoperative diagnosis method, it is often limited by the availability of material.
The etiology of SFTP is currently unknown. Miettinen et al. 17 showed that it may be related to genetic variations of environmental or inborn origin. A paracentric inversion on chromosome 12q13 involving the NAB2–STAT6 fusion gene might be a possible mechanism. 18 A study published in the journal Chest reported familial SFTP in a mother and her daughters. 19 Considering that the patient described herein was young, we were able to evaluate her mother’s health status; no abnormality was observed on chest X-ray or CT during physical examination of the patient’s mother. Therefore, the case reported here was considered sporadic. Nevertheless, we informed this patient of the need to watch for similar presentations in her mother and future children (if any).
Although commonly occurring in the pleura, solitary fibroma can occur outside the pleura, in almost every anatomical location. Histologically, extrapleural solitary fibroma and SFTP have similar histological features, manifesting as a random distribution of oval- and spindle-shaped cells in a collagen stroma. In terms of biological behavior, extrapleural fibroids occurring in the mediastinum, retroperitoneum, pelvis, and meninges are more aggressive than SFTP, which might be related to different rearrangement patterns in the NAB2–STAT6 fusion gene. 20
The main treatment for SFTP is to remove the primary lesion. Video-assisted thoracoscopic surgery has clear advantages for removal of small tumors (<5 cm) that do not involve the chest wall, including shorter operative duration, less bleeding during surgery, less chest tube drainage, and faster recovery. The thoracotomic approach is suitable for giant masses, to remove the tumor more completely and reduce the possibility of tumor cell dissemination.21,22 In this case, the patient’s tumor was <5 cm in diameter and the tumor tissue surface was smooth, so we removed the tumor by thoracoscopic surgery. The operation went smoothly, with little bleeding (∼10 mL) and no other complications.
The strongest relationship with prognosis and survival is whether SFTP is benign or malignant. Benign tumors have a high survival rate, whereas malignant tumors that have invaded or metastasized have a poor prognosis. Complete surgical resection, careful postoperative follow-up, and systemic therapy may increase the long-term survival of patients. Because the biological behavior of solitary fibrous tumor is unpredictable, all patients need long-term follow-up for 15 to 20 years. 23 In the patient reported here, the tumor was small with a clear boundary and with no evidence of metastasis. Post-surgical recovery was satisfactory and follow-up was recommended.
In conclusion, SFTP is very rare and the clinical symptoms are not obvious. Imaging, pathology, and immunohistochemistry are valuable tools for diagnosis and differential diagnosis. Surgical resection is an effective treatment, and the prognosis is generally favorable. Although there are few reports, missed diagnosis or misdiagnosis in young people is a potential concern.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethical statement
This article reports a case that discovered incidentally upon physical examination. Ethical approval was unnecessary, and the patient gave verbal consent for publication of this case report.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.