
Abstract
Introduction:
The hemangioma is the most common vascular tumor, involving the head and neck in 60% of cases. It is rare in the larynx. In children, hemangiomas are more frequent on the subglottis, whereas in adults the most common site is the supraglottis. Laryngeal hemangioma with cavernous features isolated to the free edge of the vocal fold is a very rare clinical finding. We present 2 cases of glottic hemangioma. Both patients reported severe hoarseness.
Cases:
In the first patient, an extensive blue-purple mass was seen on the right vocal cord. The patient was posted for microlaryngeal surgery with carbon dioxide (CO2) laser. Second patient had a large, smooth, flesh-colored polypoid mass emanating from the left vocal cord. The patient was posted for microlaryngeal surgery. After 2 months, both patients showed a considerable voice improvement.
Discussion:
Vocal cord hemangiomas are very rare, and they usually cause problem in the voice of the patient. A vascular lesion that may mimic a hemangioma may sometimes result from an organizing hematoma following a hemorrhage on the vocal cords due to voice abuse. Laryngeal hemangiomas also need to be distinguished pathologically from polypoidal vascular granulation tissue that may be produced by laryngeal biopsy, intubation, or trauma. Indirect endoscopy is enough to diagnosis. No active treatment is advised for adult laryngeal hemangiomas unless the lesions are symptomatic or show a tendency to involve other parts. There is no uniformly accepted treatment of head and neck hemangiomas. Surgical excision with laser CO2 microlaryngoscopic techniques gives satisfactory results.
Introduction
Laryngeal hemangiomas are slowly progressing benign vascular tumors of endothelial origin which are commonly diagnosed in children but are rarer in adults. The incidence of the laryngeal hemangioma in infants is 4% to 5%, however incidence in adults is unknown due to the scarcity of case reports. 1
Usually adult hemangioma does not regress spontaneously and mainly affecting the male sex; only seldom in adult laryngeal hemangioma is simultaneous with cutaneous head and neck localizations. 2
In children, it is usually located at the subglottic level causing dyspnea. In adults, it can be seen in different location such as the epiglottis, aryepiglottic folds, arytenoids, and false and true vocal cords, causing hoarseness. 3
Mulliken proposed a classification based on clinical and endothelial cell characteristics. This classification provided the first fundamental separation of vascular anomalies into lesion with a proliferative component (vascular tumors) versus relatively static vascular malformations (based on principal anomalous vasculature).
From a histologic aspect, it is mainly of cavernous type, capillary type, or mixed with a thin and friable mucosa covering the vascular stroma. Cavernous hemangioma is a benign, but sometimes locally destructive lesion composed of enlarged and dilated vascular spaces. The gross appearance is dependent on the depth of the lesion. Superficially located tumors tend to appear blue. Microscopically, these tumors are identified by the presence of large irregularly sized vascular channel that may be arranged haphazardly through the tissue. Capillary type hemangioma is characterized by a proliferation of small, capillary-sized blood vessels.
Currently, there is no consensus regarding the treatment of hemangiomas due to their rarity. For small laryngeal hemangiomas, observation is the preferable treatment because it is not often a progressive tumor. However, large hemangiomas require treatment and this can include surgical resection, corticosteroid injections, ethanol injections, cryosurgery, and interferon treatment. Potential complications consist of growth along with alteration of the laryngeal functionality. In the present study, we described 2 cases, 1 patient with hemangioma of the right vocal cord and 1 patient with hemangioma of the left vocal cord. Also we have described the strategies and controversies in the treatment of laryngeal hemangioma and reviewed the literature.
Case Report
Patients in this study were seen at the Unit of Otorhinolaryngology, Department on Neuroscience, Federico II University of Naples, Italy. The study has been conducted by respecting the role of Helsinki declaration and authorized by the institutional review board committee of Federico II University of Naples.
Case 1
A 61-year-old man reporting hoarseness since 2 months. He didn’t report dysphagia or dyspnea. He was exsmoker for about 20 years of 10 cigarettes per day. He had no story of alcohol use.
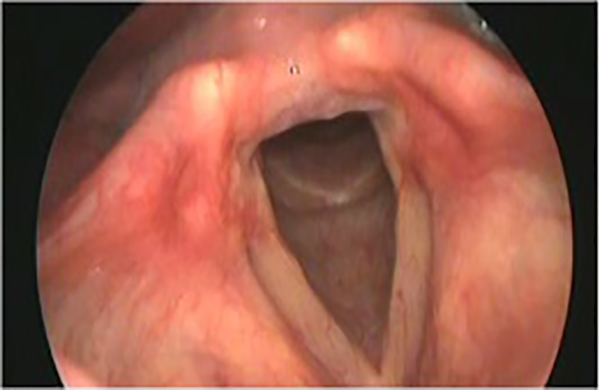
On physical examination, an extensive blue-purple mass was seen on the right vocal cord (Figure 1). By rhinoscopy, oropharyngoscopic and otoscopic findings are regular. The patient was posted for mycrolaryngeal surgery with carbon dioxide (CO2) laser (type 2 cordectomy).We used an operating microscope (Sensera/S7 Carl Zeiss with 415 mm focal lenses), associated with a CO2 laser system (LumenisSharplan 40 C). The laser was set in the superpulse laser emission mode and with an intensity power of 8 to 10 W.
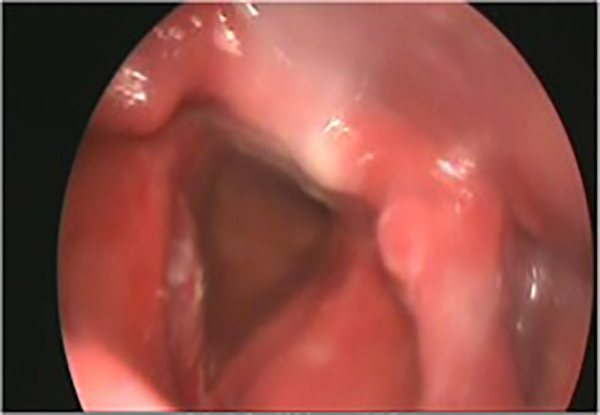
Case 1 endoscopic view: hemangioma in the right vocal cord.
An incision was made between the normal mucosa and the margin of the hemangioma. No difficulty was encountered during dissection of the lesion.
The histopathologic examination indicated cavernous hemangioma (Figure 2). At control examinations, the patient shows no subjective discomforts and has regular local findings with no sign of local recurrence.
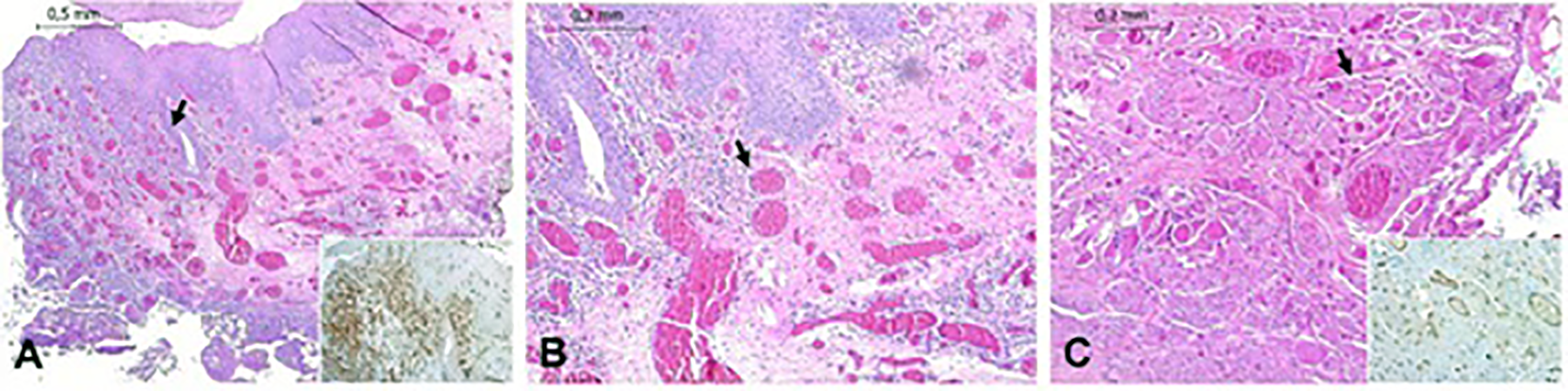
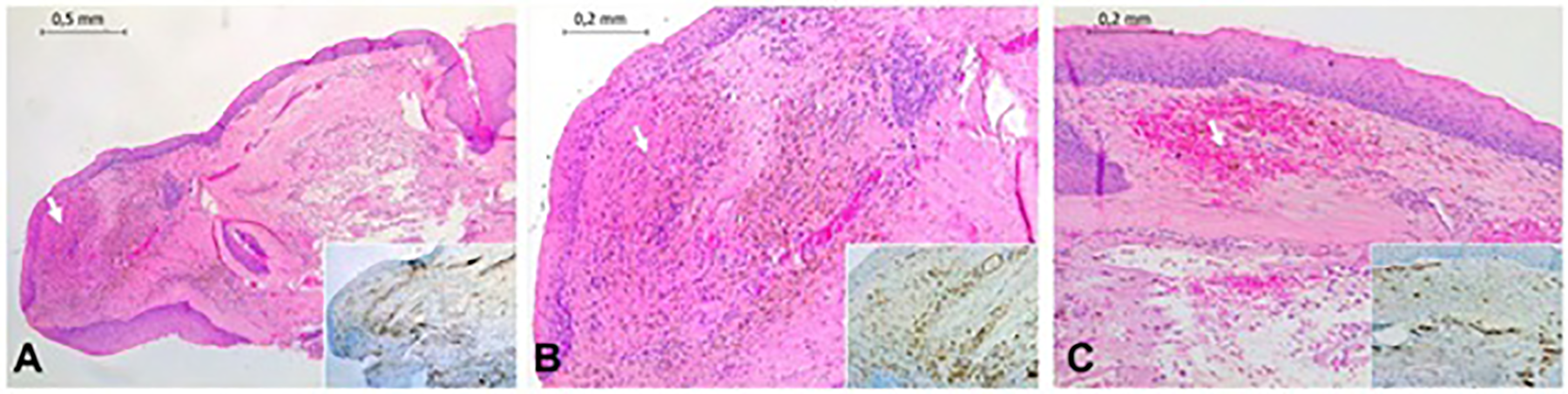
Case 1 image shows laryngeal mucosa with hyperplastic epithelium and a vascular proliferation with lacunar aspect in the corium (black arrow; H/E staining, ×4 magnification). Vascular proliferation is highlighted by immunostaining for CD31, a vascular marker (see insert, ×4 magnification). B, Detail of (A): Vascular proliferation has infiltrative pattern (black arrow; H/E staining, ×10 magnification). C, Involvement of striate muscle (black arrow; H/E staining, ×10 magnification). Insert shows immunoreactivity for CD31 (×10 magnification). Scale bar at left top of each image. H/E indicates hematoxylin and eosin.
After 2 months, there was a good improvement in the voice and, on the examination, the vocal cord movements were normal (Figure 3).
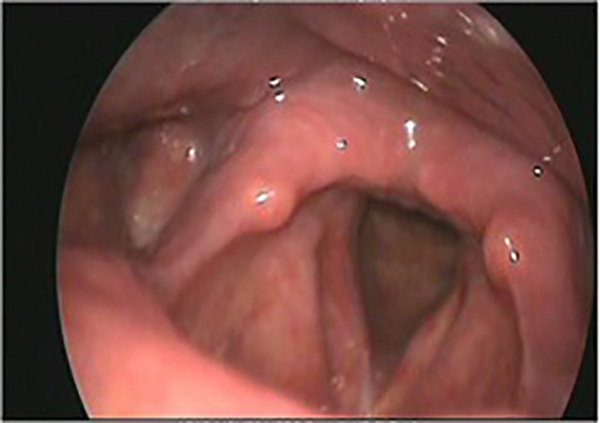
Case 1 endoscopic view after 2 months.
Furthermore, no recurrence of the hemangioma was detected during a 2-year follow-up period.
Case 2
A 30-year-old man reporting hoarseness since 4 months. He didn’t report dysphagia or dyspnea. He was a smoker of 10 cigarettes per day. Indirect laryngoscopy revealed a voluminous blue-black-colored neoformation on the left vocal cord (Figure 4). The patient was posted for mycrolaryngeal surgery with CO2 laser (type 2 cordectomy).
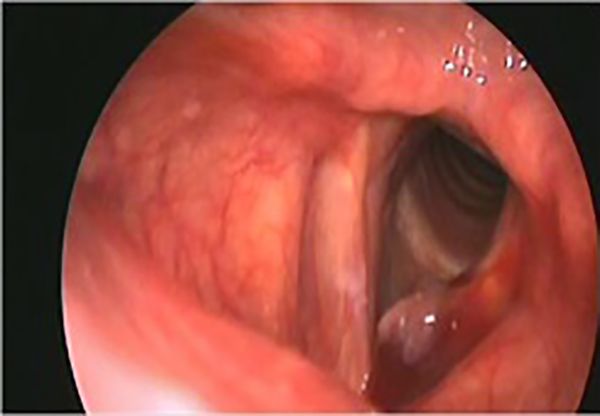
Case 2 endoscopic view: hemangioma in the left vocal cord.
We used an operating microscope (Sensera/S7 Carl Zeiss with 415 mm focal lenses) associated with a CO2 laser system (LumenisSharplan 40 C). The laser was set in the superpulse laser emission mode and with an intensity power of 8 to 10 W. The minimal bleed that occurred was controlled with application of local pressure by cotton swabs soaked in 1/50.000 adrenalin solution.
The histopathologic examination indicated an endocordal cyst and capillary hemangioma (Figure 5). At control examinations, the patient shows no subjective discomforts and has regular local findings with no sign of local recurrence.
Case 2: A, Image shows laryngeal mucosa with a proliferation of small vascular structures, arranged in a capillary lobular architecture (white arrow; H/E staining, ×4 magnification). Vascular proliferation is highlighted by immunostaining for CD31, a vascular marker (see insert, ×4 magnification). B, Detail of (A): This vascular proliferation is composed of small capillaries. Extravasation of erythrocytes and hemosiderin deposits are also present in the corium (white arrow; H/E staining, ×10 magnification). Capillaries are marked by CD31 immunostaining (see insert, ×10 magnification). C, Other different area shows extravasation (white arrow; H/E staining, ×10 magnification). Insert shows immunoreactivity for CD31 (×10 magnification). H/E indicates hematoxylin and eosin.
After 2 months, there was considerable improvement in the voice and, on the examination, the movements of vocal cords were normal (Figure 6). No recurrence of the hemangioma was detected during a 3-year follow-up period.
Case 2 endoscopic view after 2 months.
Discussion
Hemangiomas are benign vascular tumors commonly seen in the head and neck region. Laryngeal hemangiomas are divided into infantile and adult forms. Infantile hemangiomas are more frequent than adult ones, and they are commonly subglottic. In adults, the occurrence of laryngeal hemangiomas is quite rare, and supraglottic involvement is the most common site for such cases. 4 No causative or predisposing factors have been considerated. 5
Silent from a clinical viewpoint, the principal symptom is hoarseness, occasional hemoptysis, and in advanced cases dysphagia and difficult breathing. 4
It’s important the differential diagnosis between laryngeal hemangiomas and vascular lesion that may mimic a hemangioma may sometimes result from an organizing hematoma following a hemorrhage on the vocal cords due to voice abuse or polypoidal vascular granulation tissue that may be produced by laryngeal biopsy, intubation, or trauma.
The clinical and surgical experiences reported in the literature regarding hemangioma consist of case reports and small case series (Table 1). There is still no clear and unequivocal treatment and management modality, however, allow us the following considerations. Due to the high risk of hemorrhage, execution of a biopsy and cold excision is not recommended. 6 No active treatment is advised for adult laryngeal hemangiomas unless the lesions are symptomatic or show a tendency to involve other parts.
Review of Literature.
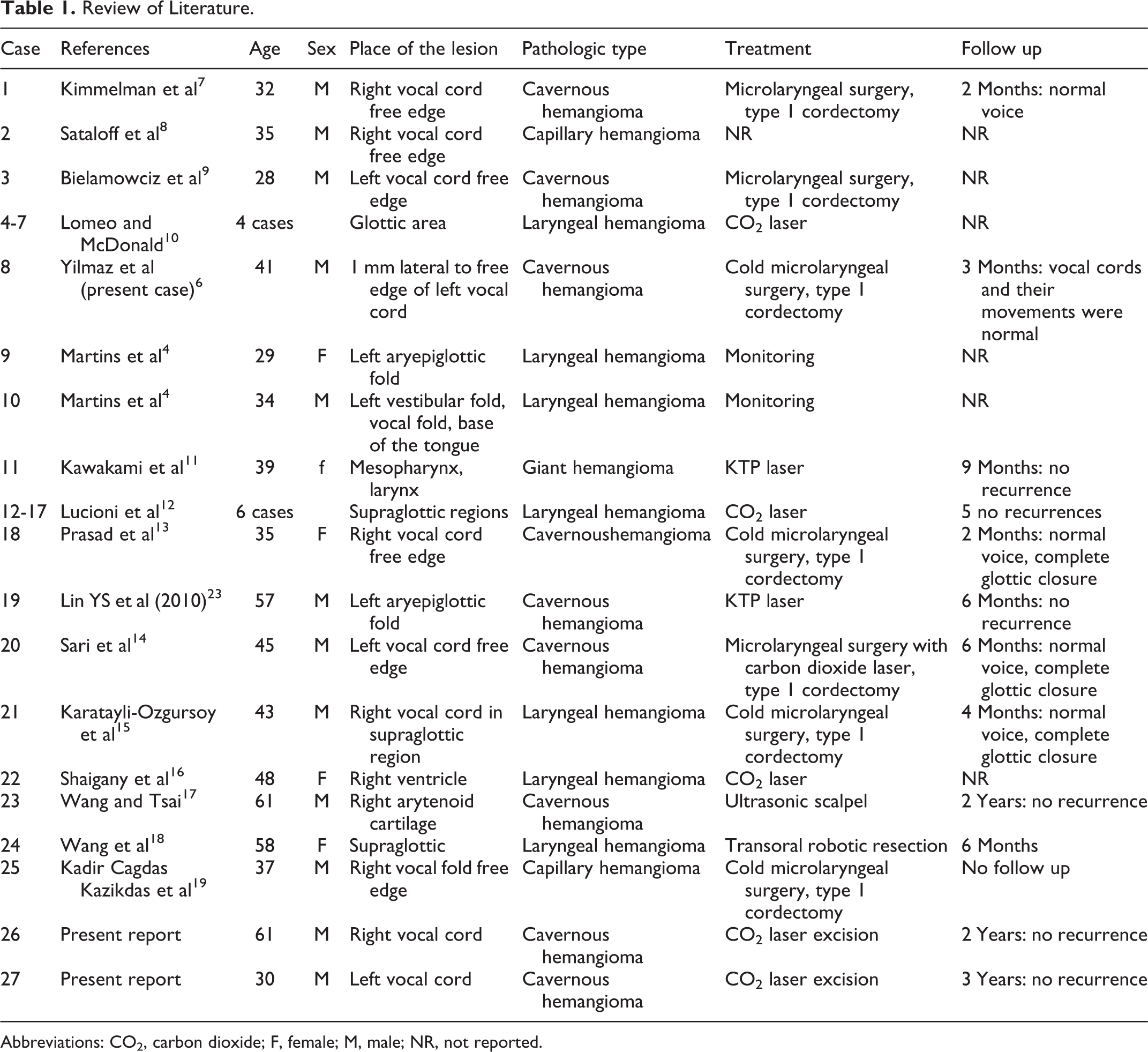
Abbreviations: CO2, carbon dioxide; F, female; M, male; NR, not reported.
Regarding the site in our 2 cases, the glottic areas are affected. Hemangioma in adults is generally seen in man and is more often of cavernous form. Cavernous hemangiomas (our case 2) differ from capillary hemangiomas (our case 1) because its vascular channels are larger, less well circumscribed, and usually deeper in submucosal tissue.
In our opinion, these anatomical and pathological data have important repercussions on the surgical approaches to be adopted in the pathological forms in question; in fact, they demonstrate: - the need to intervene early when the lesions are circumscribed to the most superficial submucosa in order to be able to carry out a radical excision of the pathological process without causing injury to the organs designated to the phonation and therefore functional damage; - a higher chance of relapses in cases where lesions are extensive and deeper such in cavernous hemangioma; in fact, it is more difficult to implement a radical excision during the first intervention This depends, in our opinion, on the basis of an imprecise clinical evaluation of the peripheral margins of the lesions. In fact, only the histological confirmation of healthy (or inflammatory) tissue throughout the sampling, and on the margin of the surgical sample, allows the excision to be considered radical.
The only treatment for symptomatic hemangioma is surgical. There are conflicting views on the type, modality, and timing of surgery. 3
There are multiple endoscopic options (microlaryngoscopy with CO2 laser or cold instruments, Potassium Titanyl Phosphate [KTP] laser, etc). To our experience, the choice of technique depends on the location and extent of the lesions.5,20-22 The utility of endoscopic surgery is here demonstrated, underlining the possibility of obtaining a definitive clinical recovery in the 2 cases studied. The CO2 laser surgery is thought to be relatively effective and less invasive than surgical removal. Benefits of this surgery are radical excision of the pathological process with a reduced trauma, better control of hemostasis, excellent postoperative functionality results, short hospitalization, and low sociohealth costs.
The Authors who support the possibility of avoiding the operationin cases with absent symptomatology, carrying out periodicclinical checks to monitor the evolution of the lesions,put—as we said—the patient to the risk of more extensiveand therefore more complex interventions with more seriousanatomical and functional injuries. 1 Based on these considerations, we believe that in cases with symptomatic laryngeal hemangiomas the surgical treatment should be implemented as early as possible because adult laryngeal hemangiomas do not regress spontaneously unlike infantile type.
Endoscopy is almost always enough for the diagnosis of a hemangioma. Other examinations, such as magnetic resonance imaging with contrast and angiography, are reserved for large tumors and for surgical patients with respiratory symptoms. Biopsies are not indicated due to the risk of severe bleeding.3,4,9
The various modalities of treatment are dependent upon the age of the patient, the site and the size of the lesion, and the hemodynamic flow of the hemangioma. 8
Systemic and intralesional steroids, interferon, laser ablation, surgical excision, cryosurgery, radiation therapy, and even temporary tracheotomy can be performed in larger hemangiomas.3,4
In conclusion, vocal cord hemangiomas are very rare, and they usually cause problem in the voice of the patient. Indirect endoscopy is enough to diagnosis. Surgical excision with microlaryngoscopic techniques gives satisfactory results.3,6,7
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.