
Abstract
Introduction
The incidence of adult laryngeal hemangiomas (ALH) is very low. It is necessary to study these tumors because only a few case reports have been published.1,2 Adult laryngeal hemangiomas, which are often bluish red and clearly defined, commonly occur in the supraglottic area of the larynx. 3 Hoarseness, hemoptysis, and dysphagia are commonly reported adult symptoms. 1 ALH are different from other hemangiomas due to their positioning and the risk of bleeding and apnea, biopsy and excision are not appropriate. Thus, the ALH could be divided into capillary, cavernous, and capillary–cavernous type in the study. This classification has been adopted 4 for the treatment of ALH rather than classification from pathological examination.
Different surgical approaches have been used to treat hemangiomas; however, all of these different procedures can mainly be classed as injection therapy and laser radiation. The reagent for the injection methods includes pingyangmycin or bleomycin, vincristine or cyclophosphamide, absolute alcohol, and a sclerosing agent. Among these reagents, vincristine or cyclophosphamide injection can cause complications, such as anemia, peripheral neuropathy, and motor delay. Moreover, absolute alcohol and sclerosing agent injection can cause pain and the risk of tumor breakage.5-7 Laser therapy includes potassium titanyl phosphate (KTP) laser (wavelength = 532 nm), Neodymium-doped Yttrium Aluminum Garnet, Nd:Y3Al5O12 (Nd:YAG) laser (wavelength = 1064 nm), pulsed dye laser (PDL; wavelength = 585-600 nm), and CO2 laser. Several authors have considered that CO2 laser excision is not advisable for adult cavernous hemangioma in view of the great diameter of vascular spaces and the significant diameter of vessels. 8 The Nd:YAG laser could cause wide range of thermal damage, which limits its application for small discrete lesions. The limited penetration of PDL is approximately 1.5 mm, whereas the penetration depth is 2 mm for the KTP laser.9,10 With these characteristics taken into account, the retrospective study was taken to assess the treatment of ALH by KTP laser and pingyangmycin injection and compared the treatment results of different surgical approaches.
Materials and Methods
The retrospective review comprised medical records of 44 patients with ALH who underwent 51 procedures with a KTP laser or pingyangmycin injection from September 2005 to November 2020. Some patients in the study were treated twice or three times because of unsatisfactory therapeutic results. Nineteen cases were treated with the KTP laser, while 32 cases received pingyangmycin injections. A comparison was made of the two major groups according to the clinical data. All patients were diagnosed based on medical history, laryngoscopic, and radiographic outcomes (15 received enhanced CT or MRI; Figures 1A and B). The ALH were confirmed via suspension microlaryngoscope examination under general anesthesia. Surgical approaches were adopted for patients with symptoms or enlarged lesions. A: Enhanced computed tomography of adult laryngeal hemangioma. B: Enhanced magnetic resonance imaging of adult laryngeal hemangioma.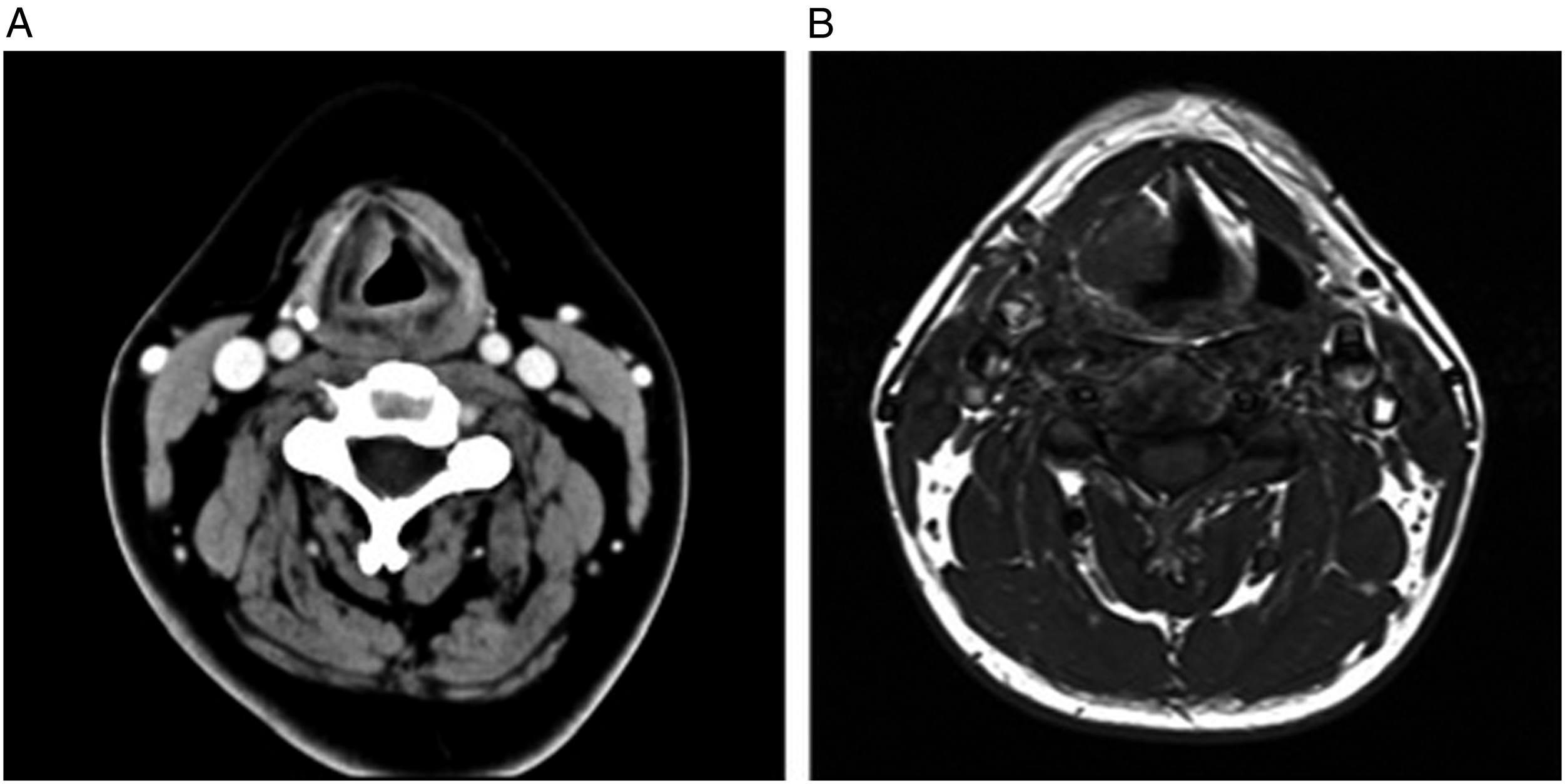
The shape, size, and classification of the hemangioma may affect the treatment results.
11
Therefore, according to the previous studies, the classification, the tumors’ bases, and the tumor shape were analyzed.12-14 The ALH were classified as capillary (plane, planotuberous, and tuberonodal) or cavernous (submucosal, intramural, transmural, and extramural) according to their morphology (Figure 2).
12
However, we did not find any transmural or extramural types among the patients in our study. Types and appearance of adult laryngeal hemangiomas.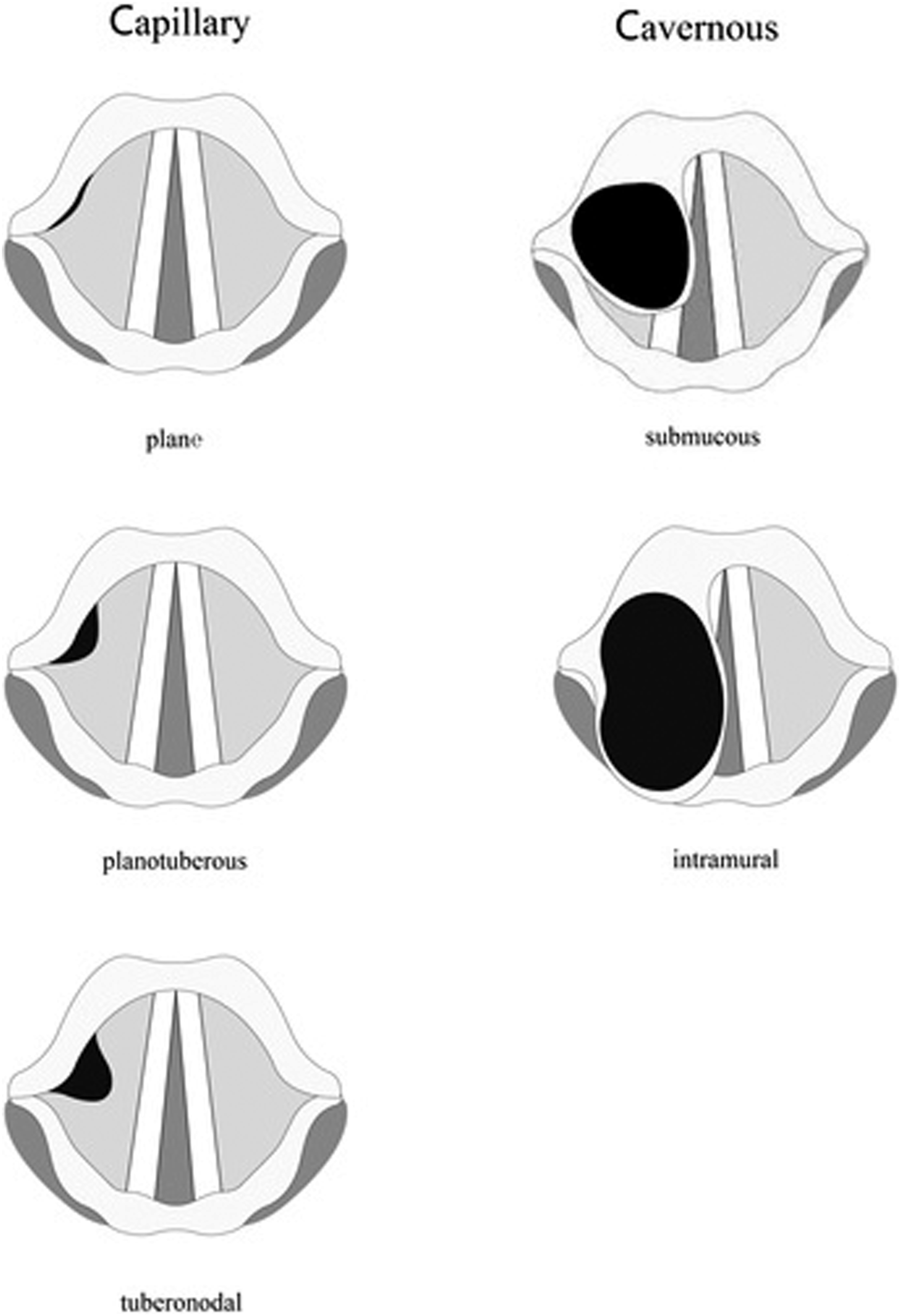
The bases of the tumors were analyzed using the semiquantitative method, and they were classified based on the major axis of their bases, as follows:
13
• Grade 1: Major axis of their bases smaller than arytenoid cartilage, or less than half a vocal cord in size. • Grade 2: Less than one vocal cord. • Grade 3: More than one vocal cord.
In a manner similar to Derkay’s staging scheme for papillomas, the tumor shape was classified using a grade of I–III (I = plane type, II = raised type, and III = bulky type) (Figure 3A, D, and G).
14
A: Plane type of adult laryngeal hemangioma before treatment. B: Two months after the KTP laser treatment of the plane-type tumor. C: Five months after the KTP laser treatment of the plane-type tumor. D: Raised type of adult laryngeal hemangioma before treatment. E: One month after the KTP laser treatment of the raised-type tumor. F: Four months after the KTP laser treatment of the raised-type tumor. G: Bulky type of adult laryngeal hemangioma before treatment. H: Four months after the pingyangmycin injection of the bulky-type tumor. I: Three months after the KTP laser treatment of the bulky-type tumor.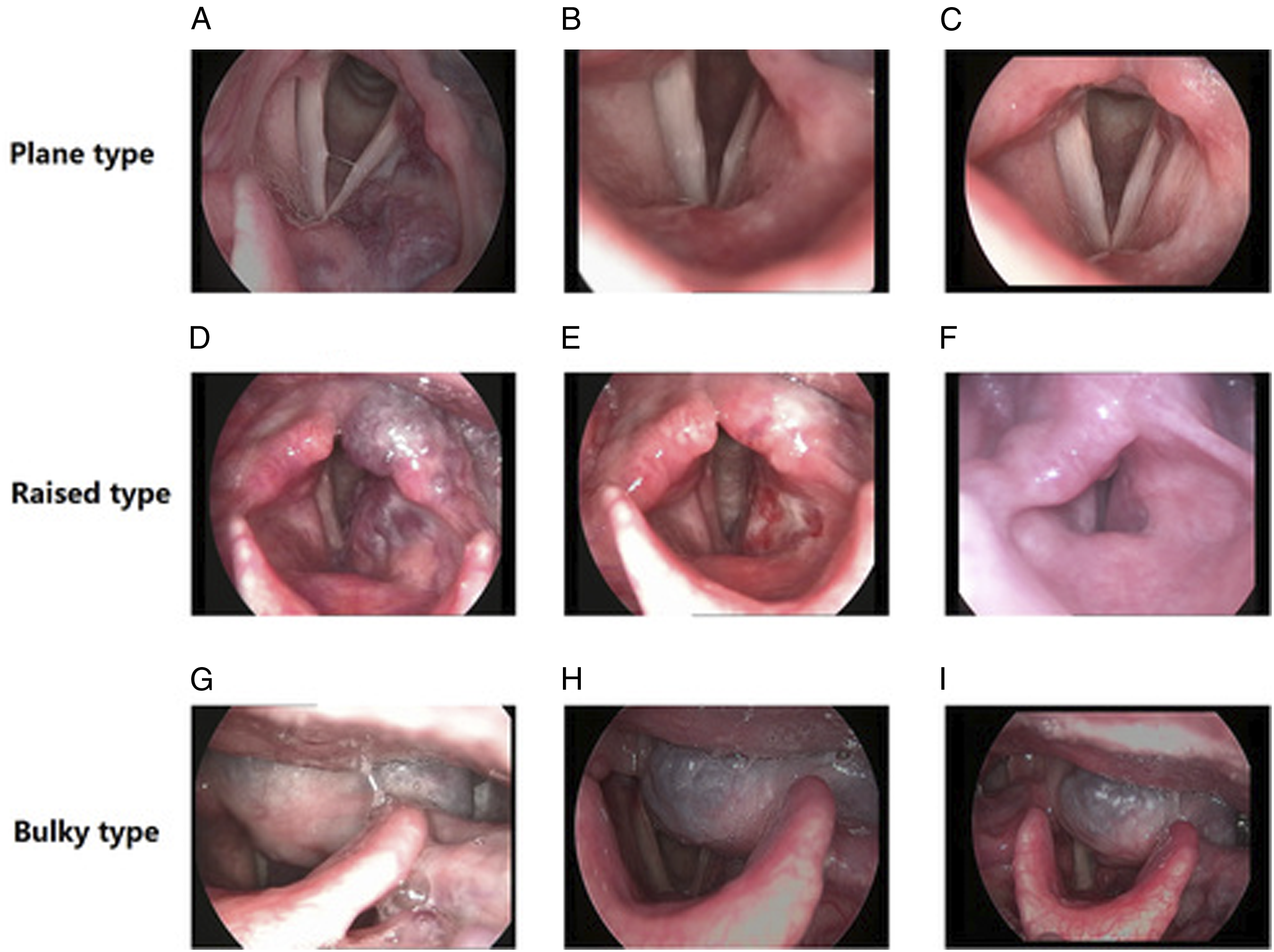
Surgical Procedures
Blood routine, coagulation function, electrocardiogram, chest radiographs, hepatic and renal function, blood glucose, and other examinations were examined to exclude systemic diseases. An ampoule of 8 mg Pingyangmycin (Tianjin Tai-He Pharmaceutical, Tianjin, China) was diluted in 5 ml 0.9% saline before the surgery. The pingyangmycin was injected into the ALH until the color of the ALH became slightly pale by a 23-gauge needle. The total dosage of one patient was less than 24 mg.
The quartz fiber of the KTP laser (Laserscope, San Jose, USA) was performed in a noncontact manner. To increase the convenience of surgery, the quartz fiber was put in a suction tube before the surgery. KTP treatments were performed at 6 W (pulsed mode, pulse width is 60 ms), which was shown to create consistent epithelial “blanching” without obvious eschar formation. The power density varied between 8 and 12 W/mm2. Total energy delivered was 100–120 J. Laser pulses were delivered in a non-overlapping fashion until blanching of the targeted angeioma was observed.
Evaluation of the Therapeutic Effect
A 4-point scale from previous studies was adopted to grade the therapeutic effect. A lumen constriction score (from 1 to 4) was used to evaluate the therapeutic effect.
Statistical Analysis
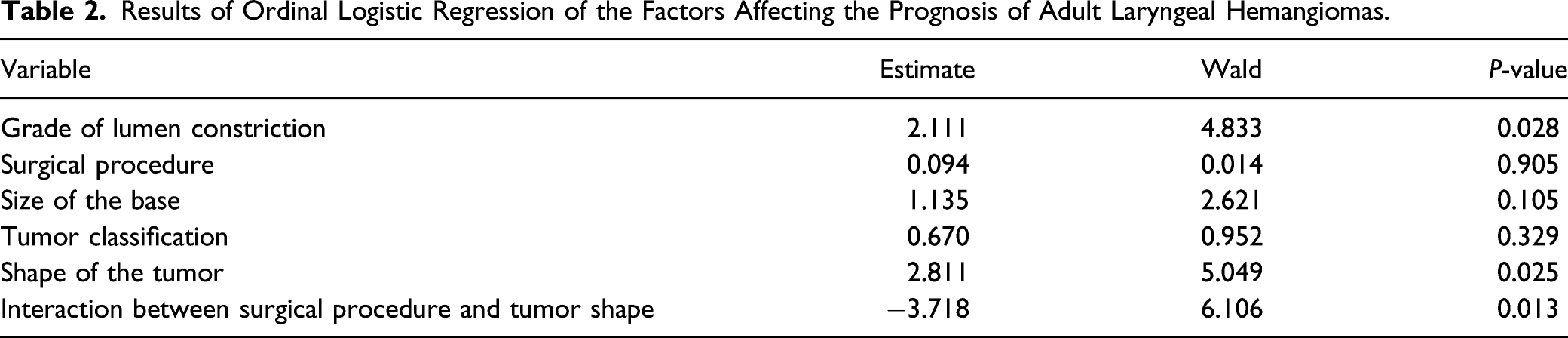
The data were analyzed by SPSS® 20.0 (SPSS Inc., Chicago, USA). An ordinal logistic regression was used to determine the influence of multivariate factors on the treatment outcomes of ALH. The Cochran–Mantel–Haenszel test was performed to assess the interaction between surgical procedure and ALH shape. A P-value less than .050 was considered to be statistically significant.
Results
The data of 28 male and 16 female patients were collected in this study. Treatment was performed in patients aged 13-69 years, with a mean age of 47.3 years. The presenting symptoms included hoarseness, globus sensation, and laryngeal obstruction.
Selection of Factors Included in the Ordinal Logistic Regression Models.
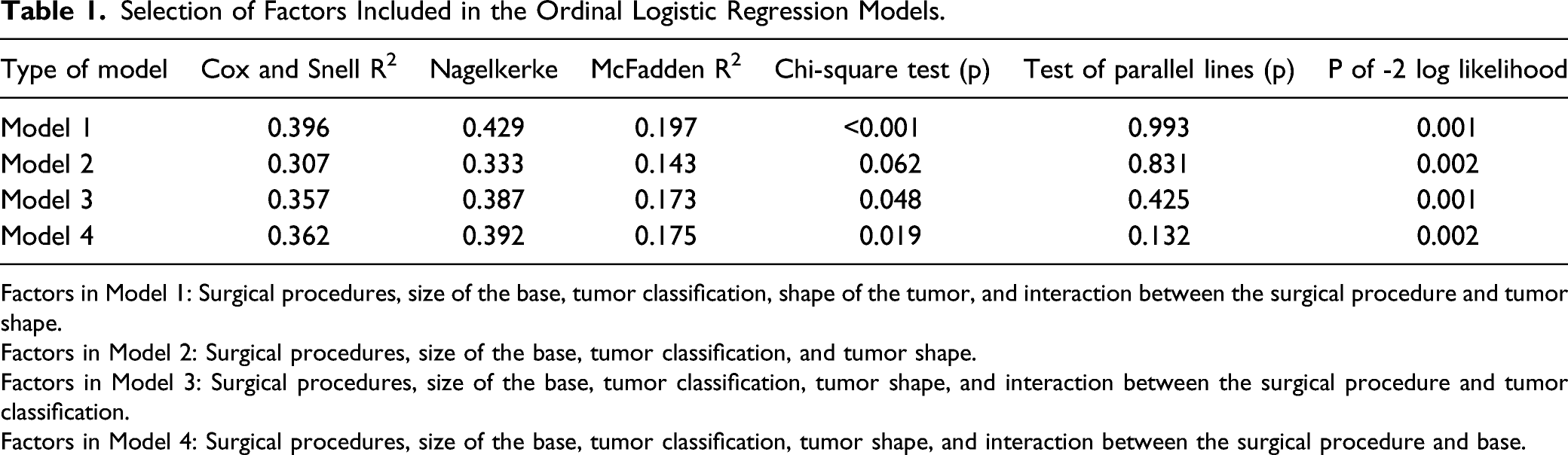
Factors in Model 1: Surgical procedures, size of the base, tumor classification, shape of the tumor, and interaction between the surgical procedure and tumor shape.
Factors in Model 2: Surgical procedures, size of the base, tumor classification, and tumor shape.
Factors in Model 3: Surgical procedures, size of the base, tumor classification, tumor shape, and interaction between the surgical procedure and tumor classification.
Factors in Model 4: Surgical procedures, size of the base, tumor classification, tumor shape, and interaction between the surgical procedure and base.
Results of Ordinal Logistic Regression of the Factors Affecting the Prognosis of Adult Laryngeal Hemangiomas.
According to the results, the relationship between the surgical methods and ALH shape was studied. To figure this out, we studied the ALH shape as a stratification variable, and the Cochran–Mantel–Haenszel test was adopted. According to the Cochran–Mantel–Haenszel test, the patients were divided into two groups (the bulky type and the plane and raised types). For the plane and raised ALH, the grade of lumen constriction in the KTP group exhibited better results than that of the pingyangmycin group (Figures 3 and 4). In the patients whose ALH shapes were plane or raised types, the KTP method has better results than the pingyangmycin injection method (P = 0.001). However, in the patients whose shapes of the lesions were bulky type, no differences were found in the two methods (KTP laser and pingyangmycin injection methods) (P = 0.770). Treatment results in the four groups (KTP laser for the plane and raised types, KTP laser for the bulky type, pingyangmycin injection for the plane and raised types, and pingyangmycin injection for the bulky type).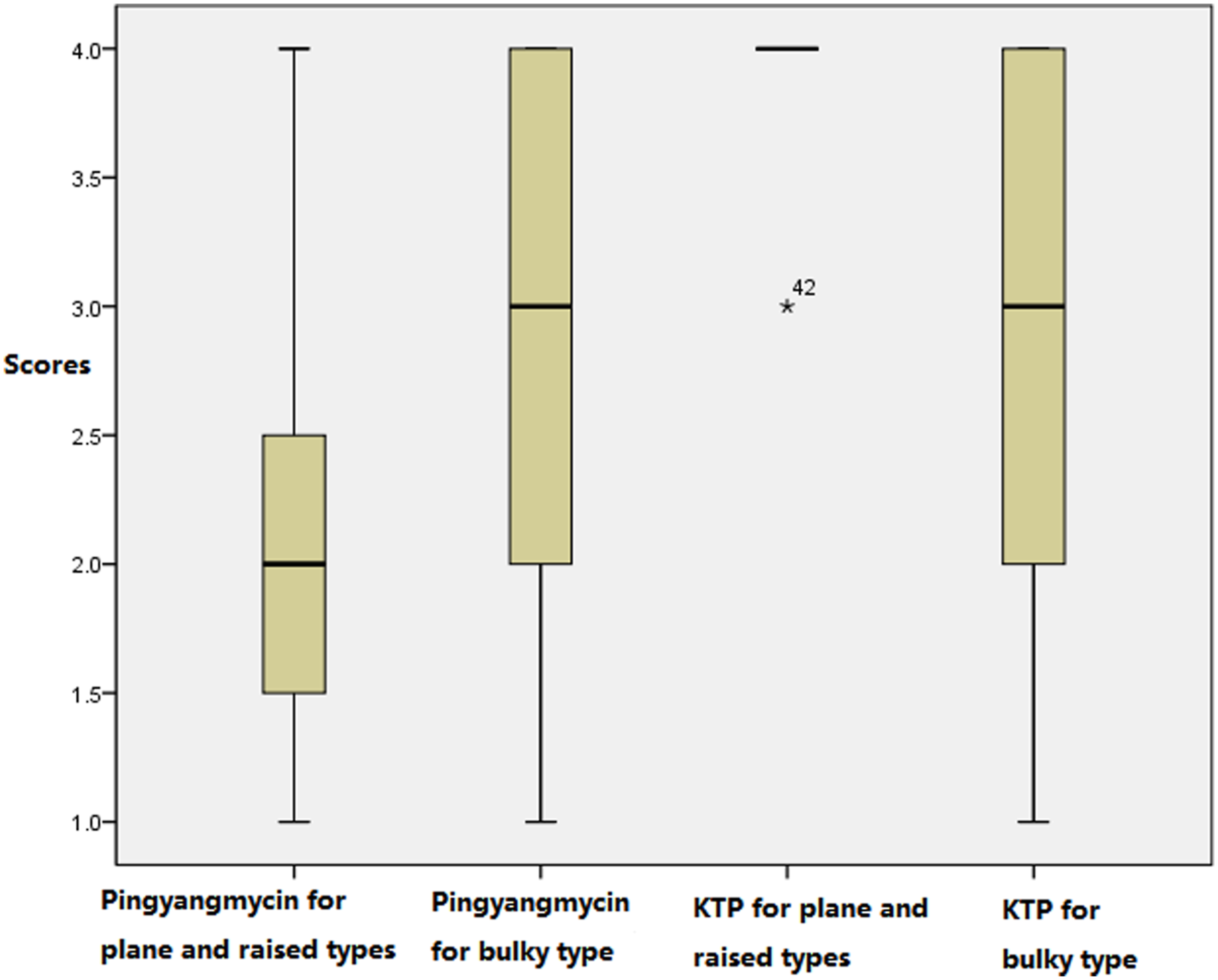
There were no serious side effects of the pingyangmycin injection, like alopecia, shock, fever, cutaneous adverse reactions, low white blood cell counts, and toxicity of the body organs. Similarly, tumor rupture and ulcers were not found in the KTP laser group. Any mild bleeding could be controlled by gargling with ice-cold water.
Discussions
Adult laryngeal hemangiomas, which are bluish-red in color, are commonly observed at or above the true vocal cords. It is recommended to treat the tumor when the lesion is symptomatic or when the size is enlarged. 15 ALH are different from other hemangiomas because of their location. Unlike skin hemangioma and pharyngeal hemangioma, whose treatment can be performed using direct vision, the laryngeal hemangioma is treated through a direct laryngoscope. As such, elongated operating instruments are needed, and hemorrhaging must be avoided due to the risk of blood entering the trachea. For anatomical reasons, biopsies and excisions are avoided.
Many factors, including the surgery type, ALH bases, ALH classification, ALH shape, age, and gender, could affect the treatment of ALH. How could we exclude these confounding factors? The ordinal logistic regression test was used to analyze the factors affecting the treatment outcomes of ALH. After these analyses, we found that the shape of the ALH and its interaction with the operative approaches affected the treatment outcomes. How should we analyze the interaction and evaluate the surgical efficacy of each shape of ALH? In our study, the stratification analysis was used. In Cochran–Mantel–Haenszel test, the patients were divided into two groups (the bulky type and the plane and raised types) according to their tumors’ shapes, and the surgical treatment effect of each group was analyzed, so as to control the influence of shape factor on the surgical results. The results showed that the KTP laser approach might be more appropriate for plane and raised ALH.
Approaches like KTP laser and pingyangmycin injection have been used for treating hemangiomas.6,8 Different surgical approaches used to treat hemangiomas can mainly be classed as injection therapy and laser radiation. Pingyangmycin was one of the injection methods, and the KTP laser was one of the laser methods. The two methods were performed in our hospital, and the surgery methods were selected according to the patients’ condition and their wishes.
The therapeutic effect of pingyangmycin is derived from its endothelial toxicity when at high target-tissue concentrations. The therapeutic effect of pingyangmycin is due to its endothelial toxicity when at high target-tissue concentrations. Intralesion pingyangmycin injection is often used to manage hemangiomas 16 due to its influence on the G2 and S phases of mitotic cells and the induction of DNA degradation. The endothelial cells appear swollen and vacuolated after the pingyangmycin injection. 6 The wavelength of KTP laser is 532 nm, which could be preferentially absorbed by hemoglobin in the hemangiomas. Although there are many scientific reports on the use of KTP lasers in vascular surgery, 17 their use in treating ALH has seldom been reported. The KTP laser beam wavelength of 532 nm facilitates its application when treating hemangiomas, and the KTP laser energy is transmitted through flexible quartz fibers and delivered to the tissue by handheld instruments, as there is no need for an aiming beam. Many factors could be affected by the treatment of ALH; thus, we quantized many factors, including the shape, bases, and classification of the lesion to evaluate the treatment results.
It is important to select the model from the ordinal logistic regression test because only the most appropriate model could reflect the factors affecting the treatment of hemangiomas. The selection of the models was shown in Table 1. Many parameters were used to select the logistic regression, such as −2 log likelihood, Cox and Snell R2, the Nagelkerke, McFadden R2, and the probability of the Chi-squared test results. According to these parameters, the appropriate logistic model was chosen. (Supplementary Materials). In addition, the ALH shape and interaction between the operative approaches were significantly different between the two groups in the selected model. The result implied that one surgery method might be particularly suitable for one shape of the ALH. To figure this out, the Cochran–Mantel–Haenszel test was adopted. The Cochran––Mantel–Haenszel test is widely used to measure the strength of the association between an exposure and disease or response, after stratifying on the observed covariates. Thus, observed confounders are accounted for in the analysis. In this study, we studied the ALH shape as a stratification variable. In the patients whose ALH shapes were plane or raised types, the KTP method has better results than the pingyangmycin injection method (P = 0.001).
Why the KTP laser was suitable for the plane and raised ALH? The KTP laser could achieve high tissue absorption, attained deep penetration of the hemangiomas, and had a coagulating effect. The tissue penetration of the KTP laser depends on the amount of hemoglobin and blood flow in a lesion. In a rich vascular structure like hemangiomas, the depth of penetration of the KTP laser can reach 2 mm. 9 For the plane and raised ALH, the wave of the KTP laser can reach the base of the ALH. Absorption of the laser energy causes photocoagulation of the blood vessels in the base of the hemangioma. In addition, the 532 nm wavelength is effectively absorbed by oxyhemoglobin, which makes the KTP laser well suited for the ablation of vascular lesions. This selective ablation makes the KTP laser advantageous for treating hemangiomas. In addition, it is difficult to inject pingyangmycin into the plane and raised ALH compared to the bulky type. The resultant low dose (limited by the shape of the ALH) affected the curative effect. This is because the therapeutic effect of pingyangmycin is due to its endothelial toxicity when at high target-tissue concentrations.
Both the KTP laser and pingyangmycin injection are effective methods for treating ALH. No serious side effects were found in the study. The disadvantages of KTP lasers include restricted vision through the direct laryngoscope and the cost. The disadvantage of pingyangmycin is the potential for pulmonary fibrosis when the patients received a high cumulative dose of pingyangmycin.18,19 The disadvantage of pingyangmycin is that it may cause pulmonary fibrosis after reaching a high cumulative poisoning dose.18,19
Conclusions
Both the KTP laser and pingyangmycin injection are successful and relatively safe treatments for ALH. For plane and raised ALH, the KTP laser may be recommended.
Supplemental Material
sj-pdf-1-ear-10.1177_01455613221086534 – Supplemental Material for A Comparison of Potassium Titanyl Phosphate Laser and Pingyangmycin as Treatment for Adult Laryngeal Hemangioma
Supplemental Material, sj-pdf-1-ear-10.1177_01455613221086534 for A Comparison of Potassium Titanyl Phosphate Laser and Pingyangmycin as Treatment for Adult Laryngeal Hemangioma by Xiufa Wu, MD, Jingru Ma, MD, Jing Zhang, and Chunsheng Wei in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.