
Abstract
Objective
To evaluate and compare the results of the excision and bleomycin injection treatment methods for adult laryngeal hemangiomas (ALHs) located on the arytenoids.
Methods
Twenty-six ALH patients in 29 different cases were enrolled in the study at our department between June 2012 and March 2021. Some patients were treated more than once. Twenty-nine cases of ALH treated with either bleomycin injection or excision were studied to assess the efficacy of both treatments. A lumen constriction score (from 1 to 4) was used to evaluate the therapeutic effect three months later.
Results
The ALHs in the ALH excision group were resected successfully, and the ALHs did not recur. The mean lumen constriction score for the bleomycin injection group was 2.95. The lumen constriction score for the ALH excision group was higher than that of the bleomycin injection group.
Conclusions
Both bleomycin injection and excision are safe and effective treatments for ALHs located on the arytenoids. On the condition that the ALH is well exposed and can be completely removed, ALH excision surgery is the preferable method to treat ALHs located on the arytenoids.
Introduction
Laryngeal hemangiomas are relatively rare in the head and neck area. Most infantile laryngeal hemangiomas resolve on their own, but adult laryngeal hemangiomas (ALHs) do not tend to spontaneously resolve. Those located on the arytenoids are a special kind of ALH because of the location and the morphological characteristics of the arytenoids. Compared to laryngeal hemangiomas in other areas, the loose connective tissue of the arytenoids can cause the base of ALHs to be more fully exposed. The arytenoids are adjacent to the pyriform fossa, where food often passes through, so there is a risk of hard food puncturing ALHs located on the arytenoids. A ruptured tumor can induce serious bleeding, causing blood to flow into the respiratory tract; this can result in death. Many methods have been used to treat ALHs. The optimal surgical approach remains controversial. Some authors advise against ALH excision. 1 However, Steiner and Ambrosch 2 state that ALHs can be successfully removed if they are pedunculated or limited to specific areas. In this study, we review the results of 29 cases of ALHs located on the arytenoids to evaluate and compare the treatment methods of excision and conventional bleomycin injection.
Patients and Methods
This is a retrospective study. Twenty-six ALH patients who underwent 29 different procedures between them—either conventional bleomycin injection or ALH excision—at our department between June 2012 and March 2021 were enrolled in the study. The research ethics board of our hospital approved the study and waived the requirement for informed consent due to its retrospective nature. The patients were divided into 2 groups—the ALH excision group (9 cases) and the conventional bleomycin injection group (20 cases). The 20 cases in the conventional bleomycin injection group received bleomycin injections. In the ALH excision group, 3 cases underwent “cold as a surgical instrument” therapy (which included the use of microlaryngeal forceps and microlaryngeal microscissors); 2 cases underwent holmium laser therapy; and 4 cases underwent CO2 laser therapy.
ALH diagnoses were made based on patient history, laryngoscopic findings, and contrast-enhanced computed tomography (CT) (Figure 1). All the surgeries were performed under general anesthesia using a suspension microlaryngoscope. In the ALH excision group, hemangioma classification was done based on histopathological examination. However, in the conventional bleomycin injection group, hemangioma classification was done based on morphology, according to the classification of tracheal hemangiomas.3,4
The ALH was mainly located at the left arytenoid by laryngoscope. B: The ALH was mainly located at the left arytenoid by contrast-enhanced CT.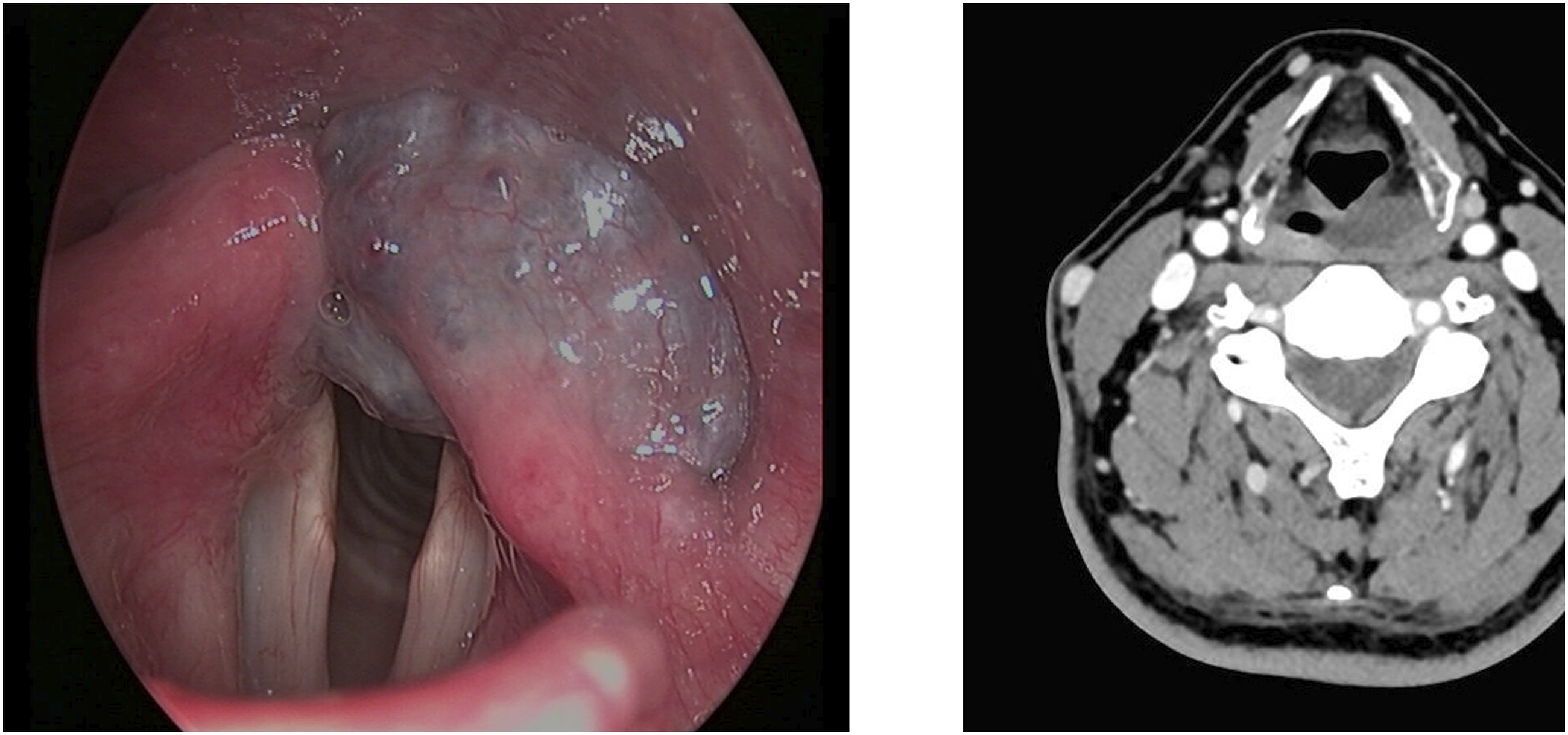
Surgical Procedures
A complete preoperative examination was performed prior to surgery to exclude systemic diseases. This included chest radiography, an electrocardiogram, hepatic and renal function tests, and other routine clinical tests. The ALH patients in the bleomycin injection group were treated with bleomycin (1.5 million units/bottle) (Tianjin Tai-He Pharmaceutical, Tianjin, China). However, the ALH patients in the ALH excision group were treated using several different methods (including CO2 laser excision, holmium laser excision, and excision using cold microsurgical instruments).
Resection of ALHs Located on the Arytenoids Under a Microlaryngoscope Using Cold Microsurgical Instruments
After general anesthesia, the ALH patients were placed in a supine position, and a direct laryngoscope was used to expose the lesions. The microscope was then used to examine each patient’s ALH, which was located on the arytenoids. After the base of the ALH was explored, microlaryngeal forceps were used to elevate the ALH. Next, laryngeal microscissors were used to separate the base of the ALH from the normal tissue. Epinephrine-soaked cotton balls were used if the wound was bleeding.
Resection of ALHs Located on Aarytenoids Under a Microlaryngoscope Using a CO2 Laser
After the larynges and adjacent sites were exposed using the laryngoscope, a WILD Heerbrugg M 655 microscope (WILD Heerbrugg, Jena, Germany) and a 400 mm focal lens, coupled with a LUMENISTM 40 model CO2 laser (Lumenis Ltd., Yokneam, Israel), were used. Two-hundred-and-seventy micron spots with the super-pulse mode at 5-7 W were used. After the ALHs were elevated using the microlaryngeal forceps, the CO2 laser was used to remove the ALHs along the base of the lesions. One of the ALH patients had a tumor with a limited base and high volume. For this one, the CO2 laser was applied after the volume of the ALH was reduced by siphoning off blood from the ALH using a 23-gauge needle.
Resection of ALHs Located on Arytenoids Under a Microlaryngoscope Using a Holmium Laser
A holmium laser (Lumenis VersaPulse PowerSuiteTM 20 Watt, Lumenis, Yokneam, Israel), with a 550 micron end-firing fiber to deliver the laser beam, was used. En bloc resection was performed at the base of the ALHs. The laser was set to deliver 3 W of energy. The holmium laser fiber held by a laser handle can reach the base of the ALHs through a direct laryngoscope (Figure 2). The holmium laser used for ALHs. A: Main unit of the holmium laser. B: Laser handles of the holmium laser. The inside of the laser handles are hollow, the laser fiber can be passed through them, and the fiber can be fixed behind the handles. C: Laser fiber of the holmium laser.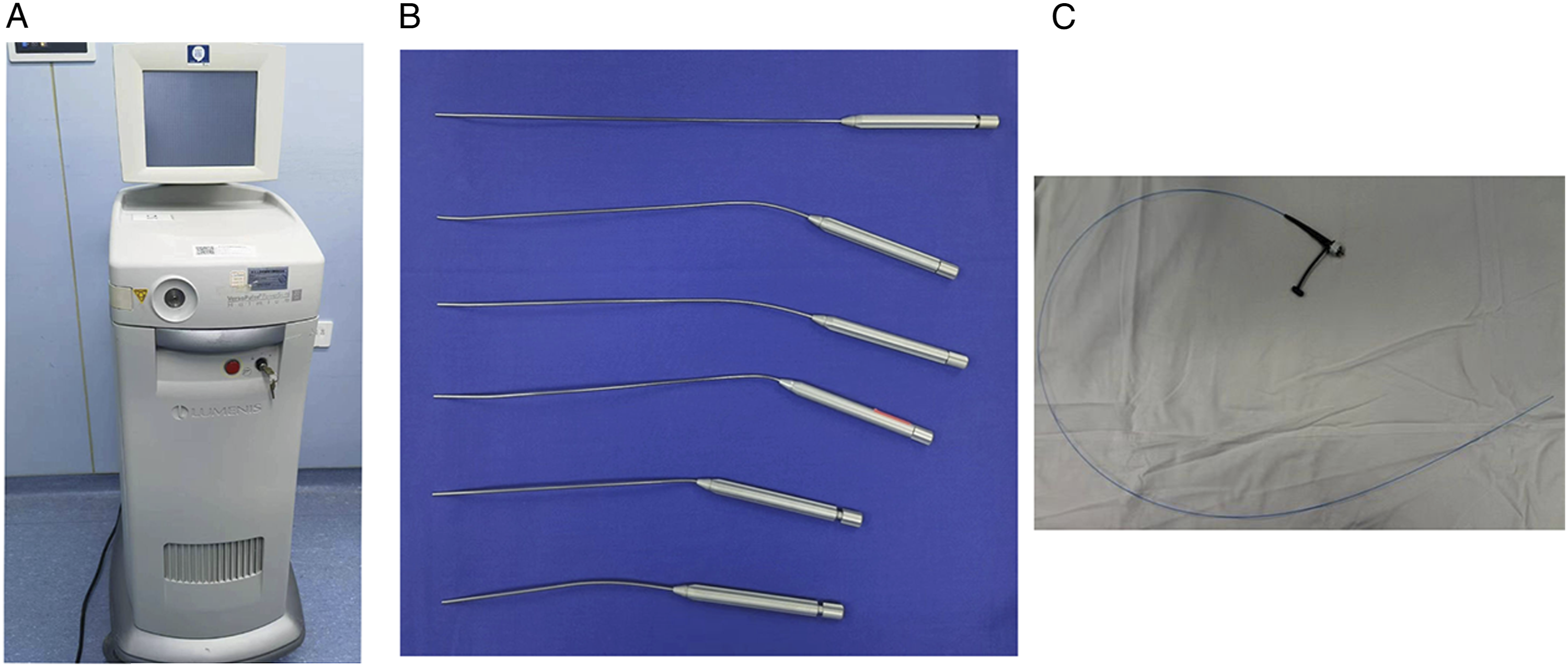
Bleomycin Injection for ALHs
Bleomycin (1.5 million units/bottle; 15 mg/bottle) (Tianjin Tai-He Pharmaceutical) was dissolved in 5 mL of normal saline solution. A 23-gauge needle was used to inject the bleomycin into the ALHs until their surfaces became slightly pale. Multipoint injections were advised. Finally, epinephrine-soaked cotton balls were used to apply pressure to the ALHs for five minutes. The maximum dose of bleomycin used in one patient in our study was 24 mg. The laryngoscope was performed to investigate the treatment results of ALHs in the bleomycin injection group a few weeks later.
Evaluation of the Therapeutic Effect
The 4-point scale used in previous studies was adopted to grade the therapeutic effect. A lumen constriction score (from 1 to 4) was used to evaluate the therapeutic effect, as follows: • Grade I (1 point): The volume of hemangiomas had not changed after the surgery. • Grade II (2 points): A decrease in the volume of hemangiomas was less than or equal to 50% after the surgery. • Grade III (3 points): A decrease in the volume of hemangiomas was more than 50% but less than 100% after the surgery. • Grade IV (4 points): Disappearance of the lesion and no recurrence for at least 1 year.5,6
Statistical Analysis
SPSS 21.0 (SPSS Inc., Chicago, USA) software was used for the statistical analysis. An independent t-test was used to analyze the continuous variables. A Mann–Whitney U test was used to analyze the categorical variables. A P value less than .050 was considered to be statistically significant.
Results
This study included 26 patients (10 males: 38.5%; 16 females: 61.53%). Patients ranged in age from 19 to 77 years of age, and the average age was 54.73 ± 14.44 years. The presenting symptoms of the 26 cases were studied, and the occurrence rates were arranged from high to low. These symptoms included a globus sensation, blood-stained sputum, hemoptysis, pharyngalgia, and no symptoms at all.
Comparison of Baseline Characteristics, Locations, Classification, ALH Size, and Grade of Lumen Constriction in 2 Groups.
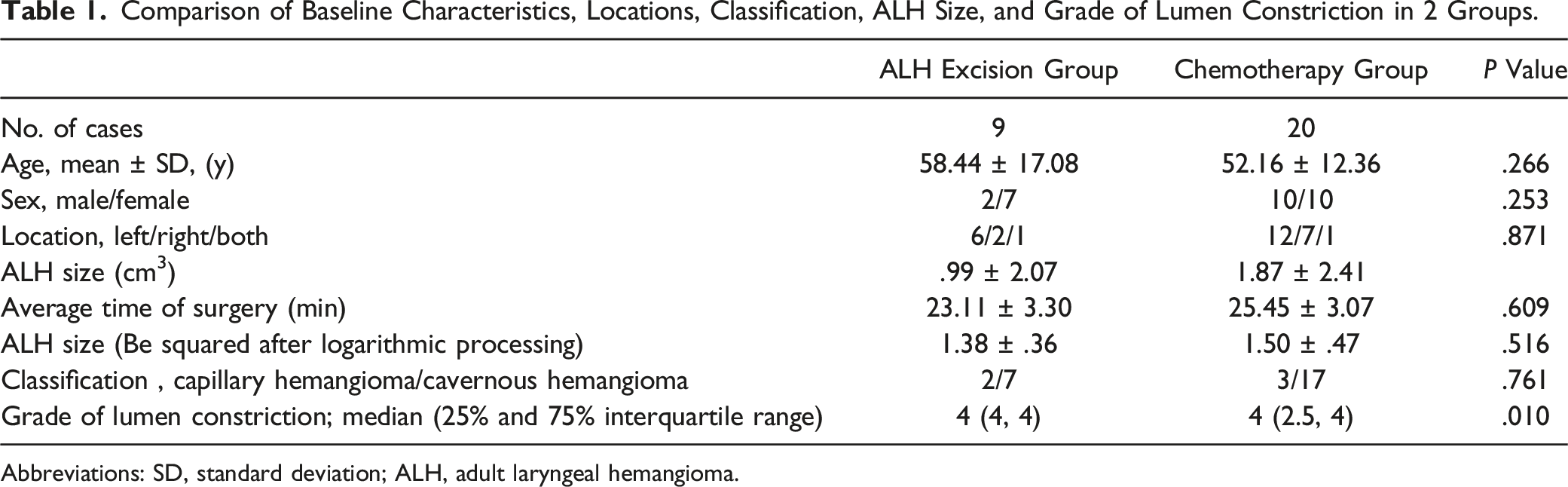
Abbreviations: SD, standard deviation; ALH, adult laryngeal hemangioma.
All the patients in the ALH excision group were cured and experienced no recurrence. The mean lumen constriction score in the bleomycin injection group was 2.95. The score in the ALH excision group was higher than in the bleomycin injection group according to a Mann–Whitney U test (Table 1; Figure 3). Side effects such as alopecia, tumor ruptures, ulcers, and pulmonary fibrosis were not observed in this study. Any mild bleeding could be controlled by gargling with ice-cold water. A: The ALH was mainly located at the right arytenoid by laryngoscope before the bleomycin injection. B: Two weeks after the bleomycin injection. C: Seven weeks after the bleomycin injection. D: The after the bleomycin injection. F: Seven weeks after the bleomycin injection. G: The ALH was mainly located at the right arytenoid by laryngoscope before the CO2 excision. H: Ten months after the CO2 excision.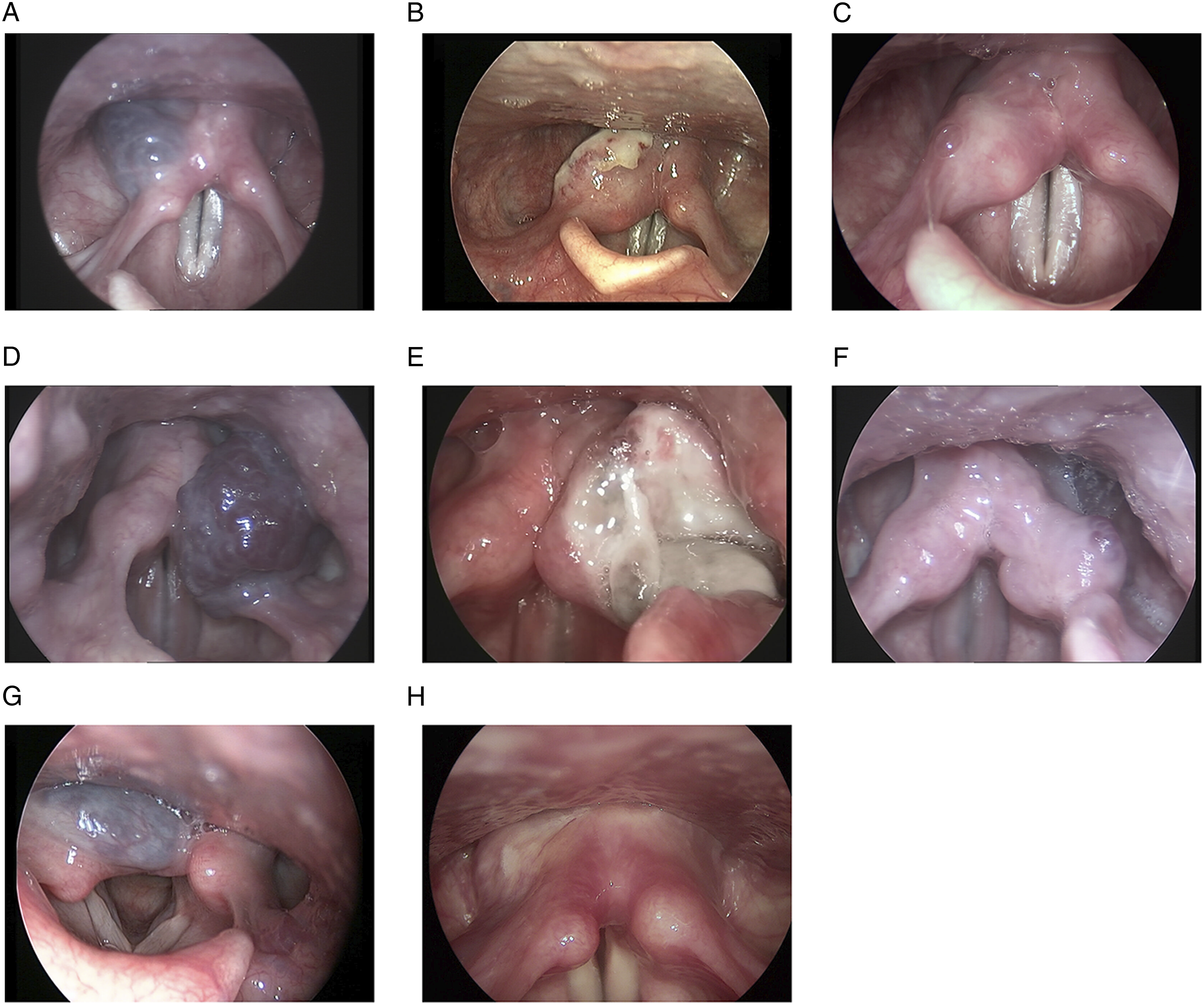
In our study, 3 patients were treated twice. One patient was treated by CO2 excision after the bleomycin injection was unsuccessful. Two patients were treated with a repeat of the bleomycin injection (Figure 4). A: The ALH was mainly located at the left arytenoid by laryngoscope before the bleomycin injection. B: Eight months after the first bleomycin injection. C: One month after the twice bleomycin injection. D: The ALH was mainly located at two sides arytenoids by laryngoscope before the bleomycin injection. E: Two months after the first bleomycin injection. F: Three months after the twice bleomycin.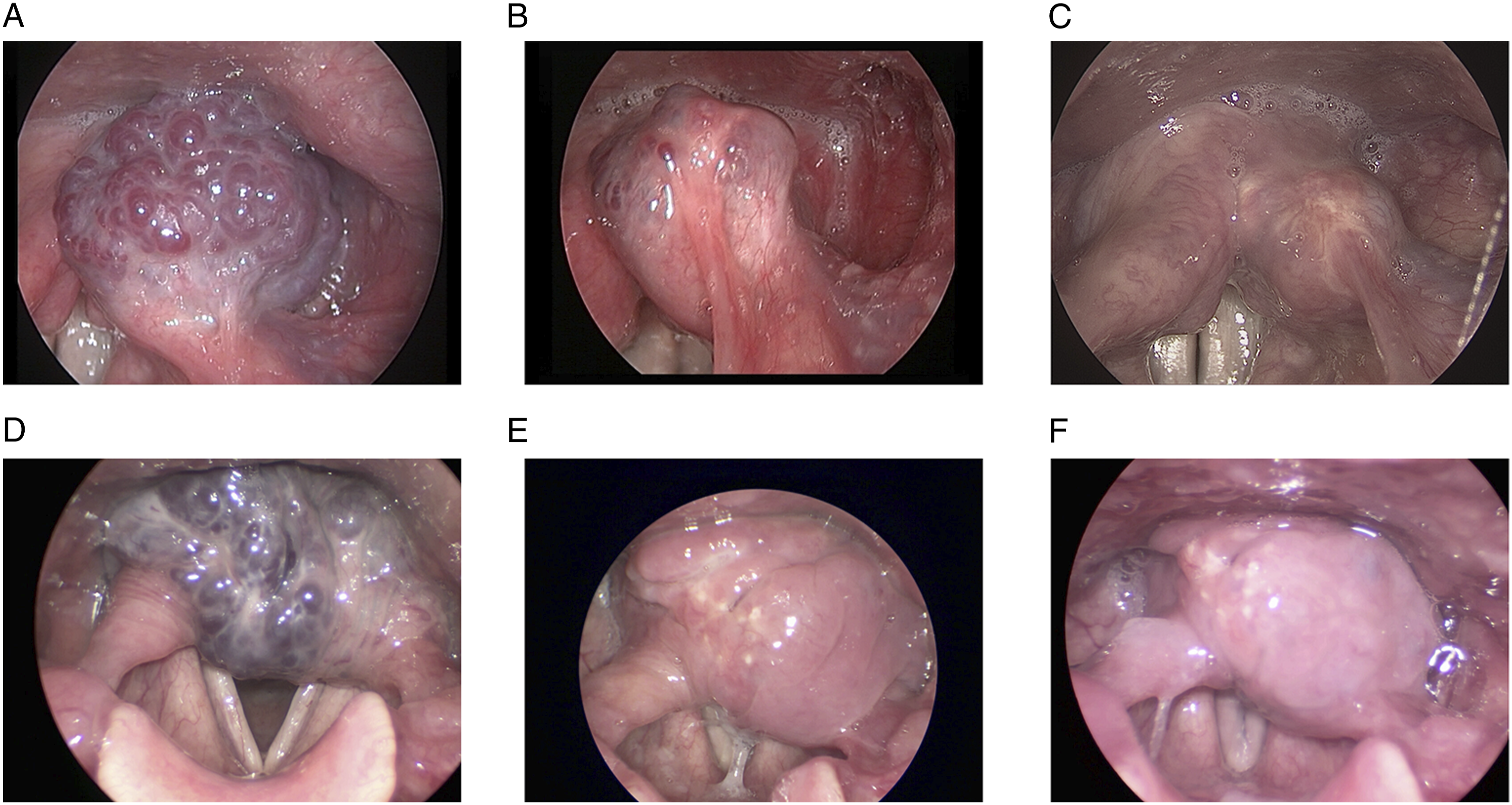
Discussion
ALHs that appeared to be bluish-red were commonly observed at or above the true vocal cords. 7 Adult hemangiomas can be located on the laryngeal ventricle, the false vocal cords, the epiglottis, the arytenoids, the laryngeal vestibule, the aryepiglottic fold, or the pyriform sinus. Hemangiomas may be found in one or more locations, making treatment of the lesions more complicated. Active treatment is advised if the lesions are symptomatic or if they are growing. There is a risk of hemangiomas rupturing, which may induce serious bleeding and can result in death, as food may go through the arytenoids. Therefore, ALHs located on the arytenoids should be treated.
The optimal approach to treat ALHs is still debated. Bleomycin injection is an effective and safe method to treat hemangiomas. 8 In our study, .3 million units/mL bleomycin was used. Bleomycin can affect the G2 and S phases of fast-dividing cells and can induce DNA degradation in undercoiled chromatin regions.9,10 ALH excision surgery can be performed using many different methods, such as using cold instruments, a holmium laser, and a CO2 laser. Some authors consider excision to be inadvisable for adult cavernous hemangiomas in view of the large diameter of vascular spaces and the significant diameter of vessels. 1 However, Steiner and Ambrosch 2 state that laryngeal cavernous hemangiomas can be successfully removed if they are pedunculated or limited to circumscribed areas. The excision surgery method was adopted if the ALHs were pedunculated or limited to circumscribed areas. Different surgery methods have been used in previous studies.1,2 In our study, the bases of the lesions were evaluated by the laryngoscope and contrast-enhanced CT before this surgery. When the bases of ALHs were shallow and could be identified under direct vision, cold microsurgical instruments were chosen. When the bases of ALHs were deep and the basal planes of the ALHs were relatively parallel to the visual field through the direct laryngoscope, the CO2 laser was chosen. However, when the bases of the ALHs were deep and the basal planes of the ALHs were not parallel to the visual field through the direct laryngoscope, the holmium laser was chosen because the energy of the holmium laser could be transferred though a fiber.
In the retrospective study, we collected the data of ALHs in the ALH excision group and the bleomycin injection group. We compared the baseline characteristics of ALHs including the following: location, classification, ALH size and demographic characteristics of the patients in 2 groups. No statistically significant between-group differences for either of the primary outcomes were detected. The lack of difference in ALH data meant the ALHs in the bleomycin injection group might also be surgically excisable. This might avoid bias in surgical selection.
A lumen constriction score (from 1 to 4) was used to evaluate the therapeutic effect.5,6 This is an effective method to evaluate the treatment result of hemangiomas. No other indicators have yet been found that evaluate the results as effectively. Our study showed that all the patients in the ALH excision group were cured and experienced no recurrence. The curative effect in the ALH excision group was better than that in the bleomycin injection group. In addition, side effects such as tumor ruptures and hemorrhoea did not occur. Why did the ALH excision surgery have better results? First, ALH excision was used only when the ALH was located on arytenoids that were circumscribed. Second, the histological characteristic of arytenoids makes ALHs located there different from ALHs located elsewhere, as the soft tissue of the arytenoids is loose. Furthermore, the CO2 and holmium lasers can excise the base of hemangiomas if the laryngeal forceps clip the hemangiomas and the surrounding loose, soft tissue. Last, the bases of ALHs located on the arytenoids can be exposed more easily. The basal plane of ALHs located on the arytenoids can be parallel to the line of sight if the laryngeal forceps clip the lesions.
In our study, one patient treated with a bleomycin injection had a poor therapeutic result. The lesion was then excised using a CO2 laser and a holmium laser. The CO2 laser was applied after the volume of the ALH was reduced by siphoning off blood using a 23-gauge needle.
ALH excision is a better method than bleomycin injection to treat ALHs located on the arytenoids. However, there is still a risk of the hemangioma rupturing, leading to hemorrhoea. Before this surgery takes place, it must be determined that the bases of the lesions are limited to the arytenoids by use of the laryngoscope and contrast-enhanced CT. Exploration before lesion resection is also necessary. If lesions cannot be completely removed during the preoperative evaluation, alternative procedures must be used. For successful surgery, it is important to have experienced doctors.
Numerous modalities in the treatment and management of hemangiomas have been proposed, including Nd:YAG laser excision,11,12 CO2 laser excision,13,14 potassium titanyl phosphate (KTP) lasers, 15 electrocautery, cryotherapy, 16 sclerotherapy, interferon alfa-2a, 17 corticosteroids, embolization, and radiation therapy.18,19 These methods can be divided into excision methods and non-excision methods. For ALHs located on the arytenoids, the excision method produces better results. Preoperative evaluation of the base of the ALH and surgical experience are critical. Before the excision, it must be confirmed that the location of the base of the ALH is limited to the arytenoids. However, for ALHs located on the arytenoids whose bases are not limited or invasive, the bleomycin injection is recommended. The bases of the ALHs in our study are limited and not invasive. More studies are needed on patients suffering from ALH.
Conclusions
Both excision and bleomycin injection are safe and effective methods for the treatment of ALHs located on the arytenoids. The ALH excision method may produce better results when the base of an ALH located on the arytenoids is circumscribed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Science and Technology Commission of Shanghai Municipality (CN) (18411965600) and Shanghai Municipal Key Clinical Specialty (shslczdzk00801).
Ethical Statement
The research ethics board of our hospital approved the study and waived the requirement for informed consent due to its retrospective nature.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.