
Abstract
Laryngeal schwannomas are rare benign neurogenic tumors of the larynx. They cannot be detected in the early stages because disease onset is asymptomatic. This case of laryngeal schwannoma provided a reference for clinical diagnosis and treatment strategy. A 24-year-old man presented with a 3-year history of hoarseness and sore throat for 6 months. Laryngoscopy and computed tomography showed submucosal bulging of the right ventricular fold in the right paraglottic space. The patient underwent tracheotomy first, followed by laryngotomy. The edema of the laryngeal mucosa was significantly alleviated, with normal movement of the bilateral vocal cords on the 10th day after surgery. The tracheal tube was removed at the time of discharge. The hoarseness had disappeared at the end of the first month after surgery. The effective treatment of laryngeal schwannoma involves complete resection with surgery while protecting the integrity of the larynx and restoring laryngeal function. The indication for surgery should be strictly controlled to avoid damage to the mucosa and structures of the larynx.
Introduction
Laryngeal schwannomas are rare neurogenic benign tumors that develop in Schwann cells. Most laryngeal schwannomas originate from the superior laryngeal nerve, with those originating from the recurrent laryngeal nerve accounting for only 0.1-1.5% of benign tumors of the larynx. 1,2 Laryngeal schwannoma cannot be detected in the early stages because it shows no symptoms at disease onset. As the tumor enlarges, patients often experience hoarseness, cough, pharyngeal foreign body sensation, sore throat, and difficulty swallowing. 3 Further tumor enlargement may block the glottis and cause laryngeal stridor and dyspnea. 4,5 A case of laryngeal schwannoma, and its diagnosis, and treatment strategy are reported below. Ethical approval to report this case was obtained from the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University. Informed consent was obtained from the patient for the publication of the case.
Case report
A 24-year-old man presented to the otolaryngology clinic with a 3-year history of hoarseness and sore throat for 6 months. This patient did not have fever, cough, dyspnea, or recent respiratory tract infection. He had no family history of laryngeal tumors or hereditary diseases. Fiber laryngoscopy showed submucosal bulging of the right ventricular fold and ventricle of the larynx. The bulging squeezed the right vocal fold to the glottis, and weakened the movement of the right vocal cord, which led to poor glottic closure (Figure 1A). Cervical enhanced computed tomography (CT) revealed a mass in the right paraglottic gap characterized by a solid cystic appearance and a clear edge without cartilage erosion. There was no abnormal enlargement of the cervical lymph nodes (Figure 1B). (A) Preoperative fiber laryngoscopy, (B) preoperative neck enhanced computed tomography (CT), and (C and D) intraoperative discovery.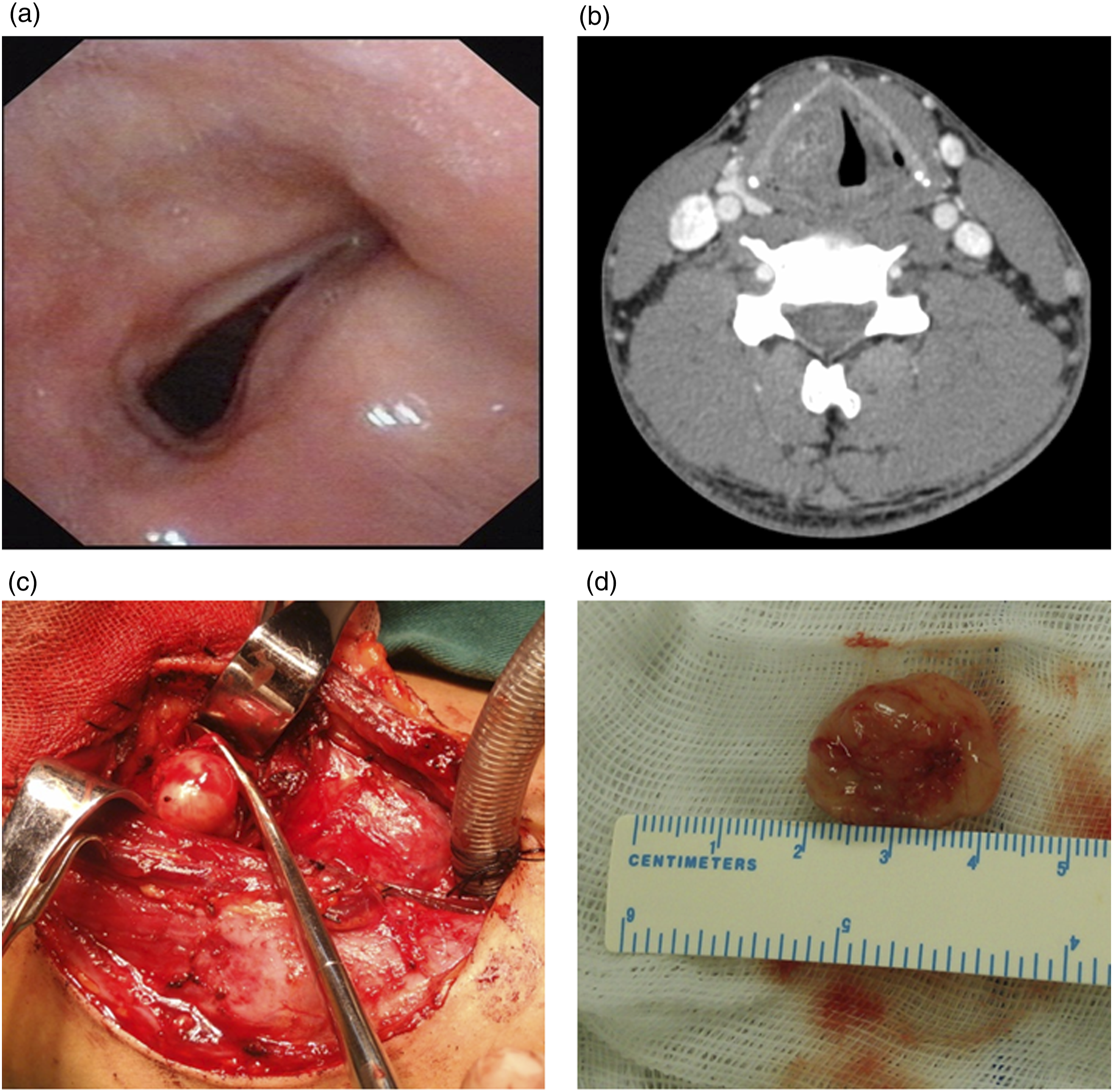
Based on the tumor dimensions, the patient underwent surgery with an external approach. The procedure was preceded by tracheotomy, followed by laryngotomy. The normal structure of the larynx was protected during the operation, especially the vocal cord mucosa. A hard tumor was observed in the paraglottic gap of the right thyroid cartilage plate measuring 2.0 cm × 1.5 cm × 1.0 cm, which originated from the branch of the superior laryngeal nerve. The tumor was covered with a smooth membrane and had a clear boundary (Figure 1C and 1D). Postoperative pathological diagnosis indicated a schwannoma.
The patient’s laryngeal mucosa showed edema on the third day after surgery (Figure 2A and 2B). On the 10th day after surgery, the edema was significantly alleviated, with normal movement of the bilateral vocal cord (Figure 2C and 2D). The tracheal tube was successfully removed at the time of discharge. The hoarseness had disappeared at the end of the first month after surgery. (A and B) Fiber laryngoscopy on the third day after surgery and (C and D) fiber laryngoscopy on the 10th day after surgery.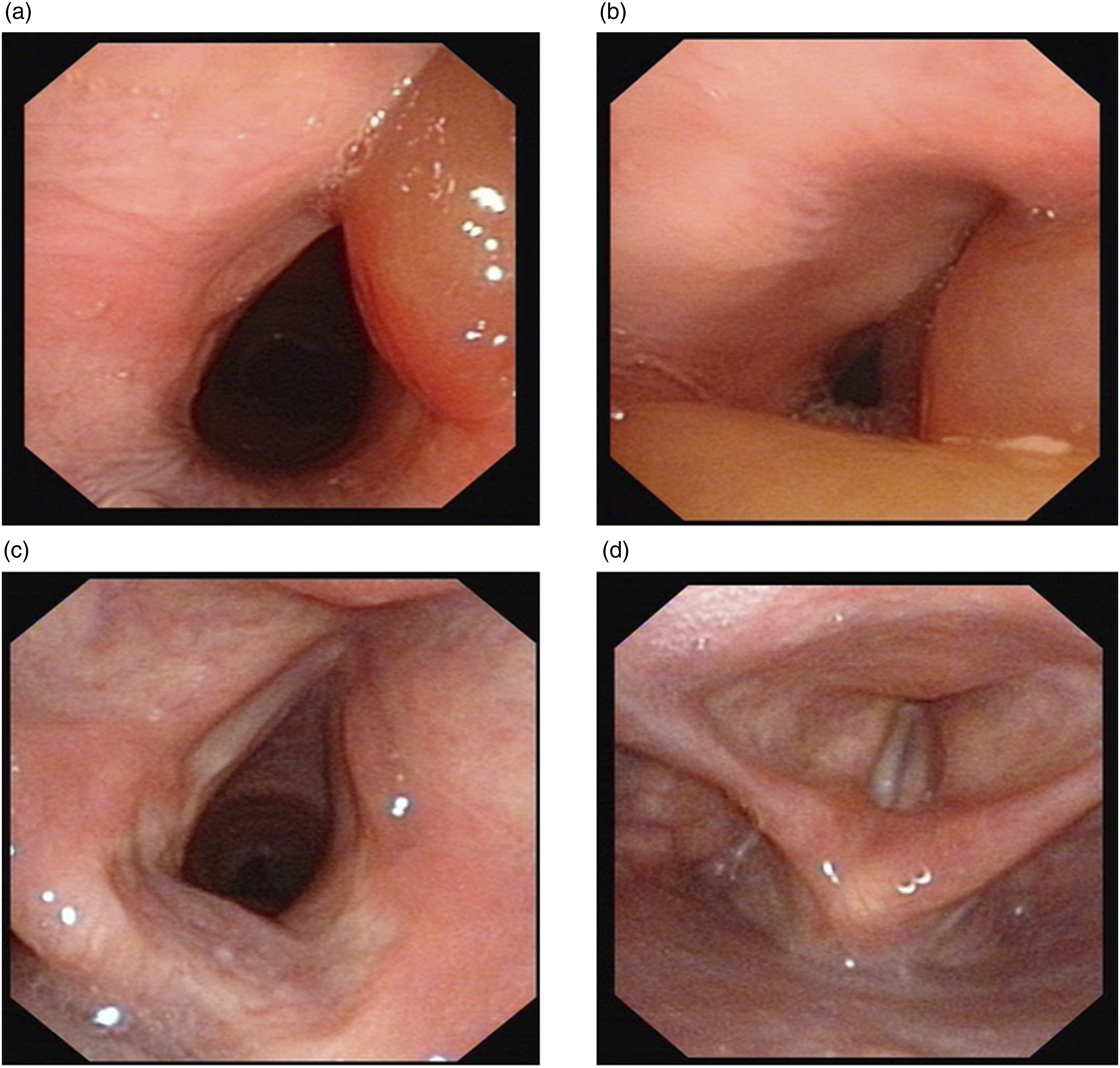
Discussion
Laryngeal schwannomas often present as single round, oval, or lobulated tumors with smooth membranes. They can be asymptomatic in the early stage and grow slowly; thus, the medical history can last for years to decades. During laryngoscopy, most laryngeal schwannomas are detected in the posterior aryepiglottic fold, which may involve the ventricular fold, arytenoid, and vocal cord; they may also extend into the pyriform fossa, which causes the ventricle of the larynx to bulge or disappear. In more severe cases, laryngeal schwannoma can squeeze the vocal cords inward, even causing pseudo-fixation of the ipsilateral cricoarytenoid joint. This condition may lead to misdiagnosis before surgery or the development of an inappropriate surgical plan.
CT and magnetic resonance imaging (MRI) are the preferred methods of examination for laryngeal schwannomas. 6 The tumor often manifests as an inflated growth with a clear boundary, no infiltration, and no cartilage damage. Its characteristic appearance is a circular or oval mass with a low density. Irregular high-density enhancement images are intermingled inside the tumor and are related to the inconsistent distribution of chronic hemorrhage and cystic changes. 7 Laryngeal schwannomas must be differentiated from laryngeal chondroma, laryngeal adenoma, laryngeal cyst, or laryngocele. 8 The diagnosis of laryngeal schwannoma depends on the results of a pathological examination, as they are generally distinguishable from leiomyomas, fibroids, or vascular-derived spindle cell tumors.
Laryngeal schwannomas are not sensitive to radiotherapy or chemotherapy; thus, complete resection with surgery is the only effective treatment. The choice of surgical approach should be based on the tumor size and location. The goal of surgery is complete tumor removal while protecting the integrity of the larynx and restoring the function of the larynx. The tumor must be completely removed; otherwise, tumor growth may be accelerated due to membrane destruction, which may lead to tumor recurrence. 9 -13
The 2 common surgical paths are endoscopic and external. For small tumors, the endoscopic approach is preferred; however, for large tumors, an external approach is advocated owing to better tumor exposure for complete removal. 14 Endoscopic surgery mainly uses laryngeal microinstruments and CO2 lasers to resect schwannomas with pedunculated morphology. 15 -18 Endoscopic surgery has the advantages of leaving no neck incision scar, protecting laryngeal function, and allowing rapid healing. The main disadvantage of endoscopic surgery is that the surgical field is not clear. Thus, this method is mainly suitable for small tumors in the glottic or upper glottic areas, with strict indications and routine follow-up review after surgery. External surgery mainly includes lateral pharyngotomy, laryngotomy, and a cervical path, which can provide a clear surgical field to completely resect the tumor. This surgical method is suitable for patients with large tumors, which are difficult to remove completely with the endoscopic path, as well as tumors located in the paraglottic gap, subglottic area, or extralaryngeal extension. 19 The disadvantages of external paths include scarring of the neck, impaired laryngeal function, and risk of pharyngeal leakage. To ensure patient safety, routine preventive tracheotomy is performed at the beginning of surgery for patients with larger tumors. 15
The patient in the present case had a large tumor located in the right paraglottic gap. Therefore, a laryngotomy was performed to completely remove the tumor. While laryngotomy is conducive to the exploration and resection of tumors in the laryngeal cavity, it damages the structure of the larynx to a certain degree, which may reduce its function. Therefore, the scope of resection should be strictly controlled during surgery to avoid damage to the mucosa and structures of the larynx.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Scientific Research Fund of Sichuan University (grant number: 2017SCU11051) and The Science And Technology Project Of The Health Planning Committee Of Sichuan (grant number: 18PJ076).