
Abstract
Importance
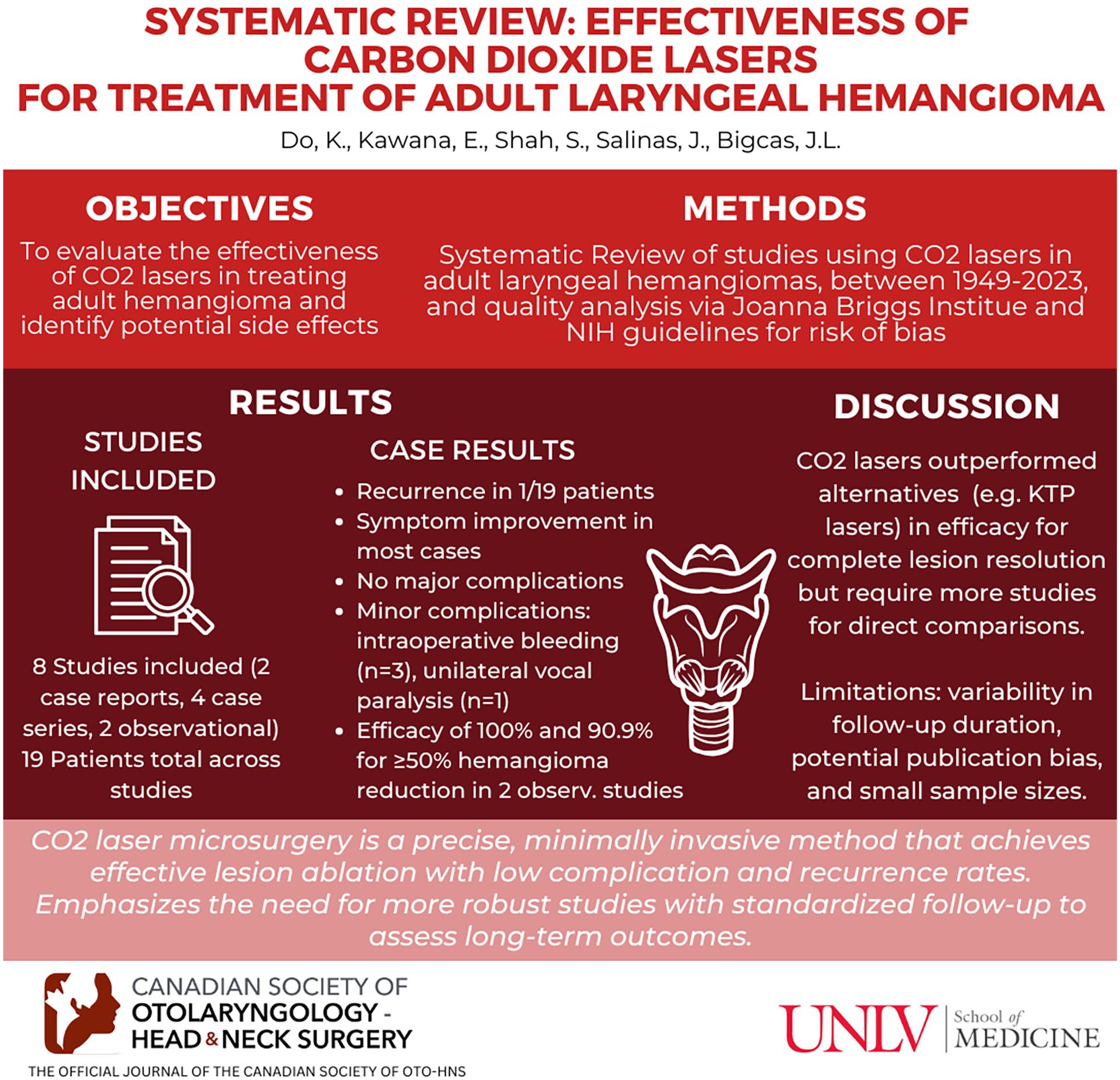
Adult laryngeal hemangiomas are rare and may cause symptoms such as dysphonia, dysphagia, and dyspnea. Carbon dioxide (CO2) lasers offer an alternative approach to managing this rare condition.
Objective
The objective of this study is to evaluate the effectiveness of CO2 lasers in treating adult hemangioma and to identify potential side effects associated with this treatment modality.
Design/Methods
The study utilizes the PRISMA model to systematically collect articles available in the current literature. The numbers obtained from each academic manuscript were then used to calculate the effectiveness of CO2 laser therapy in patients with laryngeal hemangiomas. Articles from 1949 to 2023 were gathered using the PRISMA systematic review method.
Setting
Not applicable
Participants
Adult patients with laryngeal hemangioma who were treated with CO2 lasers.
Intervention or Exposures
Surgical management with CO2 lasers.
Main Outcome Measures
Number of patients with at least a 50% reduction in laryngeal hemangioma size.
Results
Two case reports, 4 case series, and 2 observational studies were included in this systematic review. For the case reports and series, only 1 out of the 19 patients experienced recurrence following CO2 laser treatment. However, some studies did not have adequate follow-up time. In the 2 observational studies, efficacy rates of 100% and 90.9% were reported by the authors respectively.
Conclusion and Relevance
Adult laryngeal hemangioma can be safely and successfully treated with CO2 laser microsurgery in well-selected cases. More studies, as well as longer patient follow-ups, are needed to truly assess the efficacy of CO2 laser in treating laryngeal hemangioma. This method provides a minimally invasive technique for adult patients with this rare disease.
Introduction
Hemangiomas consist of blood vessels that form benign vascular tumors.1,2 These tumors represent the most prevalent type of benign tumors seen at birth. 3 Although close to 60% of hemangiomas are detected in the head and neck area, it is uncommon for them to present in the larynx.1,4 Laryngeal hemangiomas occur more frequently in pediatric patients, with an incidence of around 4% to 5%, where they are often benign and spontaneously regresses during toddler years.5,6 However, laryngeal hemangiomas are even rarer in adults, and their exact incidence is unknown due to the rare nature of the disease. 7 Unlike the infantile variant, adult laryngeal hemangiomas typically do not regress on their own and they typically present in the supraglottic region. 8 Adult patients who experience laryngeal hemangiomas may experience symptoms of dysphonia, dysphagia, shortness of breath, and hemorrhages.2,9
Some of the common treatment modalities for adult laryngeal hemangioma include laser resection, cryosurgery, corticosteroid injections, and cold steel surgery. 10 Carbon dioxide (CO2) laser microsurgery has been widely used in otolaryngology and is an alternate technique to traditional cold steel procedures.11,12 This type of laser operates by using CO2 gas as a medium to produce precisely focused light energy at 10,600 nm wavelength, which can easily slice, coagulate, and vaporize water-rich soft tissue.12,13
The CO2 laser has been extensively used, having been the primary laser used to surgically excise laryngeal masses.14,15 With flexible laryngoscopy, otolaryngologists have begun using CO2 laser during office-based procedures under local anesthesia. 15 Complications with the CO2 laser are rare but have been reported to include infection, postoperative bleeding, dyspnea, and dysphagia. However, most patients respond without problems and experience immediate relief following therapy. 16 In this systematic review, we hope to address the following question: is surgery with CO2 laser efficacious for adult patients with laryngeal hemangioma? The primary outcome to determine the success of the CO2 laser is a 50% or greater reduction in size of the hemangioma, as well as the recurrence rate.
Review of the Literature
Methods
Study Design
PRISMA review model was employed to collect articles for this study. 17 The PubMed and EMBASE databases were searched for articles on “laryngeal hemangioma” using PRISMA guidelines. PubMed yielded 745 articles (1949-2023) and EMBASE 521 articles (1974-2023). Inclusion criteria focused on the use of lasers in treating laryngeal hemangioma, while exclusions included non-CO2 lasers, patients under 18, and non-English articles. Figure 1 outlines these criteria.

Study flow chart. 17
Study Selection
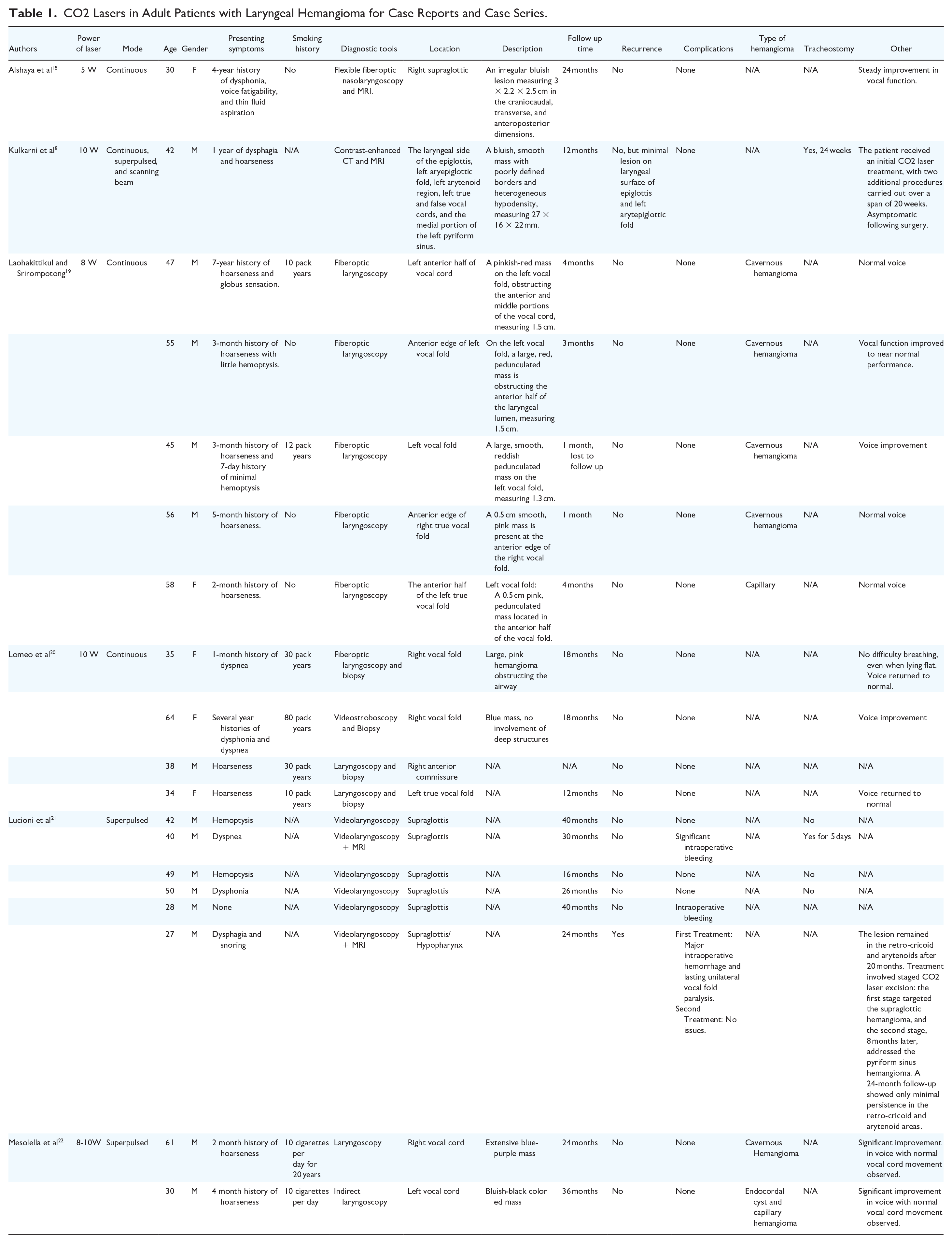
The 5-stage screening process began by evaluating article titles for relevance. Relevant titles were then screened for their abstracts, and those with pertinent information were assessed in full. These stages are shown in Figure 1. Ultimately, reviewers extracted data from 8 relevant articles for the systematic review. Table 1 summarizes the titles, year, type of CO2 laser, outcomes, and keynotes for the case reports and series included in this study. Table 2 summarizes the results of the 2 observational studies included in this systematic review.
CO2 Lasers in Adult Patients with Laryngeal Hemangioma for Case Reports and Case Series.
CO2 Lasers in Adult Patients with Laryngeal Hemangioma for Observational Studies.

Quality Assessment and Data Abstraction
The Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports was used to assess the quality and risk of bias for the 2 case reports included in this review. 25 There were 8 criteria for this assessment tool, where scores between 7 and 8 were considered good quality, 4 to 6 were considered fair quality, and 0 to 5 were considered poor quality (Table 3). The two reviewers (K.D. and E.K.) independently examined whether each study fulfilled the criteria outlined by the study quality assessment tool. A senior investigator (J.L.B.) supervised this review process and intervened if there were discrepancies in evaluations. 25
Risk of Bias Assessment of Case Reports.

The Joanna Briggs Institute Critical Appraisal Checklist for Case Reports.
The National Institute of Health (NIH) recommended tool was implemented in this systematic review to assess the quality and risk of bias for the 4 case series and 2 observational studies included in this review (Tables 4 and 5). 26 In accordance with this tool, case series were evaluated based on 9 questions, where scores 7-9 were considered good quality, 5 to 6 were considered fair quality, and 0 to 4 were considered poor quality. Observational studies were evaluated based on 14 questions, where scores between 11 and 14 were considered good quality, 7 to 10 were considered fair quality, and 0 to 6 were considered poor quality. 26
Risk of Bias Assessment of Case Series.

Quality Assessment Tool for Clinical Case Series (https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools).
Risk of Bias Assessment for Observational Studies.

Quality Assessment Tool for Observational Studies (https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools).
Definitions
The lumen constriction score was referenced by Wu et al to assess the therapeutic outcomes of patients who had undergone different treatment options, including CO2 laser combined with pingyangmycin injection. 24 According to Wu et al, this is a 4-point scale, where the numeric scale employed for evaluation had distinct interpretations: “1” denoted absence of size change, “2” represented a 50% reduction in lesion size, “3” indicated a reduction between 51% and 100%, while “4” signified a complete cure, with the lesion disappearing and not recurring for at least 1 year. 24
Results
Study Quality
The quality and risk of bias for studies included in this systematic review were evaluated based on criteria outlined by the Joanna Briggs Institute Appraisal Checklist for Case Reports and the National Institutes of Health study quality assessment tool. After evaluation, it was determined that 6 of the studies included in this study were considered good quality and 2 were considered fair quality.25,26
Case Reports and Series Patient Characteristics
Two case reports8,18 and four case series19-22 were aggregated for this systematic review. A total of 19 patients were included across these 6 studies, which consisted of 14 male and 5 female patients. The average age of these patients was 43.7 years old with a standard deviation of 11.5 years. The presenting symptoms of the 19 patients included 13 (68.4%) with hoarseness or dysphonia, 4 (21.1%) with hemoptysis, and 3 (15.8%) with dyspnea. Additionally, 2 (10.5%) presented with dysphagia, while 1 (5.3%) each had voice fatigability, thin fluid aspiration, globus sensation, or snoring. One patient (5.3%) had no presenting symptoms. Some patients presented with more than one symptom.
Among the studies that explicitly reported patients’ smoking status, 8 out of 12 patients had a significant smoking history. The number of cigarettes smoked or the pack years is detailed in Table 1.
The supraglottic region was the most common site for hemangiomas, with 7 out of 19 patients (36.8%) having lesions in this area. Among these patients, one individual (5.3%) had additional involvement in the hypopharynx. The left vocal fold was affected in 6 out of 19 patients (31.6%), while 4 out of 19 patients (21.1%) had lesions on the right vocal fold. Additionally, one patient (5.3%) had widespread involvement including the laryngeal surface of the epiglottis, left aryepiglottic fold, left arytenoid, left true/false cords, and left medial wall of the pyriform sinus. Another patient (5.3%) had involvement at the right anterior commissure.
Patient follow-up time also varied across case reports8,18 and series19-22. Seven patients (36.8%) had a follow-up time of a year or less, six patients (31.6%) had a follow-up time of between 1 and 2 years, five patients (26.3%) had a follow-up time of more than 2 years, and 1 patient (5.3%) had an unknown follow-up time. Out of these 19 patients, only Lucioni et al reported recurrence of the disease in 1 patient. 21 Although Kulkarni et al. did not report a recurrence of the hemangioma, a small residual lesion was present on the epiglottis and aryepiglottic fold because complete removal was not feasible. 8
Across the 19 patients, complications were only noted by Lucioni et al, who reported 3 cases of significant intraoperative bleeding. 21 The authors did not quantify the bleeding. Furthermore, the authors reported 1 case of permanent unilateral vocal cord paresis at 24-month follow-up. 21
Case Reports
Alshaya et al presented a 30-year-old female patient who underwent continuous CO2 laser excision at 5 Watts (W). 18 The lesion was excised successfully, and the patient’s vocal functions improved. The patient was regularly checked for 2 years, and there was no recurrence of the hemangioma. She did not experience any adverse effects from the procedure. 18
Kulkarni et al reported a 42-year-old male patient who initially was given a polidocanol injection. 8 However, the mass did not respond to the treatment, where a continuous CO2 laser at 10 W was performed 20 days later. The patient underwent two more episodes of laser therapy over the course of 5 months. Twelve months later, a follow-up examination revealed that while the mass was not entirely removed due to a conservative approach, the patient continued to show no symptoms, and there were no significant obstructions of the airway. 8
Case Series
Laohakittikul and Srirompotong followed 5 patients with ages ranging from 45 to 58 years old. 19 Four male and one female patients were diagnosed with laryngeal hemangiomas, each presenting with hoarseness and distinct locations within the larynx. In all cases, the patients underwent excision using an 8-watt CO2 laser therapy, resulting in normal vocal cord function, absence of bleeding, unobstructed airway, and no tumor recurrence. 19
Four patients were treated with CO2 in the case series by Lomeo et al. 20 The patients were a 35-year-old women, a 64-year-old women, a 34-year-old men, and a 38-year-old men. All patients had a significant smoking history, with the pack years ranging from 10 to 80. All of the patients underwent a CO2 laser excision of their laryngeal hemangiomas at 10 W under the continuous mode. Their lesions responded completely to the therapies. No recurrence and no significant complications were observed following the procedures. 20
Lucioni et al examined 6 male patients who presented with laryngeal hemangioma. 21 Their median age was 41.0 years. They were treated with a super-pulsed CO2 laser at 1 to 8 W. Following the procedures, 5 out of the 6 patients experienced no recurrence at a median follow-up time of 29 months. It is important to note that 3 patients experienced blood loss during the operation, and 1 experienced permanent unilateral vocal fold paralysis. 21
The case series by Mesolella et al examined a 61-year-old male patient and a 30-year-old male patient who presented with hemangioma to their right and left vocal cords respectively. 22 At 8 weeks, both patients’ voices improved significantly. In both patients, no serious complications occurred and there was no recurrence of the hemangioma. 22
Observational Studies
Two studies by Fang et al 23 and Wu et al 24 were observational studies and did not detail the demographics specifically for the subgroup of patients who had laryngeal hemangioma and underwent CO2 therapy, as these studies also included other treatment options and patients with hypopharyngeal involvement. Fang et al examined 68 patients who presented with laryngeal or hypopharyngeal hemangioma. 23 Depending on the size and morphology of the lesions, patients were treated with CO2 laser excision, CO2 laser coagulation + bleomycin injection, or potassium-titanyl-phosphate (KTP) laser + bleomycin injection. For our systematic review, we only assessed the efficacy of the CO2 lasers in patients with laryngeal hemangioma. There were 3 patients in the group who solely received CO2 laser excision. The power of the CO2 laser used in the excision group was 2 W. The authors in this study found that all 3 patients in the CO2 laser excision group experienced complete remission of the hemangiomas, defined as the total absence of the lesion on the laryngoscopic view. The mean follow-up time of CO2 laser patients, which included both laryngeal and hypopharyngeal patients, was 9.9 months. The study did not report any major postoperative complications for the treated patients. 23 It is important to note that Fang et al also studied one group with CO2 laser coagulation + bleomycin injection, and there were 10 laryngeal and 10 hypopharyngeal patients with an average age of 47.5 years old. However, although 9 patients had complete remission, 9 had partial remission, and 2 had stable disease, we were not able to differentiate the responses to CO2 laser between the laryngeal and hypopharyngeal hemangioma patients. 23 As a result, the patients in the CO2 laser coagulation + bleomycin injection were not included in the quantitative synthesis of this systematic review.
The retrospective observational study by Wu et al 24 reviewed 38 patients with an average age of 47.7 years who had undergone 48 procedures, including conventional chemotherapy, potassium-titanyl-phosphate (KTP) laser, and CO2 laser combined with chemotherapy. 24 The number of cases for the CO2 laser group combined with pingyangmycin was 12, although 1 patient was lost to follow-up. A continuous CO2 laser approach at 6 W was used on these patients, and the study found a 90.9% efficacy rate for the patients who were in this group. The mean lumen constriction score was 3.18. The authors reported no major adverse effects following the operations. 24
Discussion
The precise etiology of adult laryngeal hemangiomas remains uncertain, though potential contributors include vocal cord injury, intubation, trauma, and smoking. 2 In our case report and case series section, the smoking status of 12 patients was revealed, where 8 of them had an extensive smoking history. Smoking likely contributes to chronic inflammation, irritation, and cellular damage to the larynx, leading to the development of laryngeal hemangioma. 27
The most common presenting symptoms reported by patients in this systematic review were hoarseness or dysphonia. Generally, the primary goal is to completely remove the lesion during surgery. 28 However, due to the complex anatomy and the risk of functional impairment, it is crucial to monitor potential complications like bleeding or vocal cord paralysis when resecting laryngeal hemangimoma.28,29 A variety of tools can be used to identify and diagnose laryngeal hemangiomas. Previous studies have shown that laryngoscopy is effective for detecting the lesion, while MRI and CT scans are valuable for evaluating the anatomical impact, size, vascular characteristics, and morphology of the hemangioma. 30 In the case report and series section of our study, 5 out of the 19 received MRI evaluation, where 1 of these patients also underwent CT evaluation. Sixteen patients in Wu et al 24 also received either an MRI or CT evaluation.
The individual articles included in this systematic review treated patients who had capillary or cavernous hemangioma in the larynx. The main differentiating factor between these two types of hemangiomas is that cavernous hemangiomas are typically larger than capillary hemangiomas.31,32 Cavernous hemangiomas are made up of larger blood vessels and blood-filled spaces, which makes them usually blue or purple in color and can be located deeper within the skin or internal organs. Capillary hemangiomas are composed of smaller capillary vessels, which make them smaller and red or pink in color, and are mostly found on the surface of the skin.19,31,32 It is believed that for adult laryngeal hemangioma, the cavernous type is more common. 33 Although Wu et al 24 and Fang et al 23 did not provide clear details, the case reports and series that did specify the type of hemangioma included 5 cases of cavernous hemangioma and 3 cases of capillary hemangioma.
The output power of 10,600-nm CO2 is typically measured in watts. The wattage of low-power CO2 lasers typically ranges from 1 to 30 watts, and in this systematic review, the power ranged from 5 to 10 watts. 34 It is also important to note that CO2 microsurgery can be performed in a continuous or pulsatile manner. Continuous CO2 lasers produce a constant flow of energy, leading to the ablation of tissue without interruption at a specific output power. In contrast, pulsed or super-pulsed CO2 lasers produce high-energy pulses in brief intervals, where this limits damage to the surrounding tissue and offers better control over the targeted lesions. 14
The primary goal of CO2 laser microsurgery is to achieve elevated tissue temperatures through the absorption of laser energy, which is highly absorbed by water in tissues, rapidly heating and vaporizing both intracellular and extracellular water. This process leads to tissue ablation as vaporization builds pressure, causing cell membranes to rupture and allowing for precise removal, layer by layer. The heat also affects nearby tissues, causing blood vessels to coagulate, which aids in controlling bleeding during the procedure. 14 In contrast to conventional surgical methods, the laser’s pinpoint accuracy ensures precise targeting of tissues while safeguarding surrounding areas from harm. This results in the effective removal and resection of tissue, along with instant hemostatic coagulation. 14
First invented in 1964, CO2 lasers have been used in multiple specialties and in various otolaryngology pathologies, although there have been few reports reviewing the outcomes and safety of CO2 laser treatment for adult laryngeal hemangioma given the rare nature of the disease. For patients with small laryngeal lesions, initial steps may involve general observation, whereas those with bigger masses may need medical intervention. 10 Treatment modalities other than CO2 lasers have been used in treating adult and pediatric patients with laryngeal hemangioma, including the use of propranolol, corticosteroid injections, cold steel surgery, cryosurgery, and radiofrequency ablation.10,12,28,35 However, the exact efficacies of these treatment modalities are uncertain because of a lack of randomized control trials and systematic reviews addressing laryngeal hemangioma specific to adult patients. Additionally, there is no standardized protocol for treating the disease.
For the case reports/series of this systematic review, we found that CO2 laser is efficacious and safe for laryngeal hemangioma patients. Only 1 of the 19 patients had recurrence of the hemangioma. In studies reporting symptom improvement following surgery, 12 out of 13 patients became asymptomatic, showed improvement in vocal function, or fully regained normal voice function. Furthermore, few patients had any complications following CO2 laser treatment, where 3 patients had intraoperative bleeding and 1 had unliteral vocal cord paralysis. Despite not observing any recurrences within this limited timeframe, the follow-up period may be insufficient for a comprehensive assessment. There is a chance that some of these patients may have experienced recurrences several months to years after their last follow-up. Laohakittikul and Srirompotong included follow-up durations of less than a year, with the five participants being monitored for only 1 to 4 months. 19 Although there is no standard follow-up time, given the rare nature of the disease, one study assessing hepatic hemangioma found recurrence in patients between 4 and 17 years following initial resection. 36 Hepatic hemangiomas differ from laryngeal hemangiomas, but this example underscores the importance of extended follow-up periods to accurately assess treatment success.
Similar to CO2 lasers, potassium-titanyl-phosphate (KTP) lasers have been implemented in otolaryngology to treat various lesions in the larynx. KTP lasers use light energy with a wavelength of 532 nm, which is readily absorbed by oxidized hemoglobin.24,37 Fang et al examined 25 adult patients with laryngeal and hypopharyngeal hemangioma who were treated with KTP laser + bleomycin injections. 22 In their study, 10 patients experienced complete remission, 11 experienced partial remission, and 4 experienced stable disease, yielding an efficacy rate of 84.0%. 23 This was lower than the 100% and 90% efficacy rates that were reported for CO2 excision and CO2 coagulation + bleomycin, respectively. In the CO2 laser excision group, which included laryngeal and hypopharyngeal patients, all 7 individuals experienced complete resolution of their lesion while in the CO2 laser coagulation + bleomycin group, 9 had complete resolution (100% shrinkage), 9 had partial resolution (more than 50% shrinkage), and 2 had stable disease (less than 50% shrinkage). 23
Wu et al also assessed 9 patients with adult laryngeal hemangioma who were treated with KTP lasers. 24 Their study found an efficacy rate of 77.8%. 21 This was also lower than the 90.9% efficacy rate associated with CO2 laser combined with pingyangmycin use, although statistical significance was not present. A systematic review comparing CO2 and KTP lasers for respiratory papillomatosis reported that KTP lasers had lower cure and complication rates, but the CO2 laser group experienced a lower remission rate. While KTP lasers have demonstrated effectiveness in treating diverse otolaryngology conditions, their utilization is limited by the cost of the equipment. 38 Although the use of CO2 lasers is more popular in otolaryngology procedures, more studies are needed to directly compare the patient outcomes of CO2 versus KTP lasers for laryngeal hemangioma patients. 39
Limitations
Aside from the power and mode of the CO2 lasers, this study did not compare the time of exposure, use of imaging guidance, and frequency setting of the laser equipment. These different settings may have had an impact on the efficacy of their use of different patients with laryngeal hemangioma across these studies.
Another limitation is the potential for publication bias. Studies that fail to demonstrate improvement or report adverse effects from CO2 treatment may be less likely to publish their results. Only cases suitable for surgery, based on factors such as anatomy, type of vascular malformation, presence of symptoms, or lower surgical risk due to location, may be selected, while many other cases are not treated surgically. Some lesions might be very small and asymptomatic, where providers may still choose CO2 treatment. All of these factors can introduce selection bias. Also, the majority of the studies in this systematic review are case reports or case series, which may limit the generalizability of findings for laryngeal hemangioma. While we recognize these biases, the rarity of adult laryngeal hemangiomas reflects the current state of the literature. Our goal is to provide a thorough overview of CO2 laser treatment for this condition, given the lack of a standard treatment protocol.
Conclusion
CO2 laser excision for adult laryngeal hemangiomas may be appropriate in carefully selected cases. Such cases might include smaller lesions that are accessible endoscopically and located where laser treatment minimizes the risk to nearby structures, like the vocal cords. Lesions with limited depth and superficial involvement could be better suited to complete resection with a lower likelihood of recurrence. Additional considerations, such as the necessity for surgery based on symptom severity—such as hoarseness, airway blockage, or difficulty swallowing—combined with assessments of functional cost versus benefit, resectability, and complication risk, should inform case selection. For patients with health conditions that make more invasive surgery less feasible, CO2 laser excision may offer a viable option. Ultimately, selecting appropriate cases is the surgeon’s responsibility, requiring a careful balance of these factors to ensure a safe and effective treatment approach.
Footnotes
Data Availability Statement
Data is public information and is available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
Not applicable because this is a systematic review and does not involve live human participants.