
Abstract
India is one of the top 10 countries in CO2 emissions and it is considered one of the countries with the highest infant mortality rate. For these reasons, the state of health of population has become the object of studies and monitoring by many organizations and experts. In this study we try to analyze the short and long run relationship between neonatal mortality rate, economic growth, energy consumption (renewable and non-renewable), female literacy, and air pollution in India during 1970–2021 periods by using ARDL approach and VECM method. It appears that female literacy, economic growth and renewable energy consumption have an important role in reducing neonatal mortality rate. By contrast, non-renewable energy consumption, CO2 emissions and working mother's strongly increase neonatal mortality. From these results, Indian government is required to provide for the basic needs of mothers by guaranteeing her right to education and improving their standard of living. The Indian government should also reduce air pollution by launching projects, using clean and environmentally friendly energy, and constructing industrial areas away from population centers. Also, it is necessary to Also, it is necessary to reduce the dependance on energy sources polluting due to the high cost and instability of prices in the traditional energy market, as well as reducing of the global warming and the danger it poses to continuous heat and climate change.
Keywords
Introduction
Recent data published by international institutions like the World Health Organization (WHO) and the United Nations International Children's Emergency Fund (UNICEF) show that a large numbers of children die soon after birth: many of them in the first four weeks of life (neonatal deaths), and most of those during the first week. For every baby who dies in the first week after birth, another is born dead (fetal deaths or stillbirths). That for that reason, neonatal mortality remains a major public health concern especially in low- resource countries. In 2020, WHO declines that for 130 million children born each year worldwide, 14 million die in the first 28 days of life. Moreover, it is estimated that more than 3.3 million babies are stillborn every year; one in three of these deaths occurs during delivery and could largely be prevented according to WHO; 2022. Around 75% of neonatal deaths occur in the first week, and more than one-quarter occur in the first day. Neonatal deaths account for 40% of deaths under the age of 5 years worldwide (WHO, 2022). Consequently, neonatal mortality emerges as an increasingly prominent component of overall under-five mortality and is thus receiving additional attention. Recent investigations show that the worldwide neonatal mortality rate fell by 47 per cent between 1980 and 2020 from 36 to 19 deaths per 1000 live births (UNICEF and WHO, 2022). Over the same period, the number of newborn babies who died within the first 28 days of life declined from 5.1 million to 2.7 million, and more than ninety-eight per cent of the neonatal deaths occurred in developing world, where the risk of death in the neonatal period is six times greater than in developed countries; (UNICEF and WHO, 2022). In the least developed countries it is over eight times higher; while it is more than three-quarters in sub-Saharan Africa and south Asia; (UNICEF and WHO, 2022).
As one of top 10 countries in CO2 emissions in the world and the biggest country in number of population, it becomes necessary to make the grade the health sector in India. As example, we try to identify the neonatal mortality problem. In this country, neonatal mortality rate (NM) per 1000 live births dropped considerably from 70% to 28,6% between 1980 and 2020; whose the number of neonatal mortality was more than 1,8 million in 1980; and it becomes 522,250 thousands in 2020 according to the report of UNICEF; 2022. These results confirm the well-known vulnerability of the first week of life, particularly the first 24 h. The high NM rate underlines the importance to identify and to prevent the risk factors and the underlying causes of NM to reduce infant mortality. Understanding of the social and geographical pattern of NM is thus crucial for policy makers and planners to expand access to effective interventions that will improve neonatal survival.
The recent investigations show that nearly two thirds of the neonatal deaths in India are due to affections of prenatal origin. Fetus and newborn affected by maternal factors and by complications of pregnancy, labor and delivery represented on the whole about 37% of underlying causes of neonatal death; (UNICEF and WHO, 2022). Most other neonatal deaths can be avoided with effective low-cost interventions, such as clean delivery practices, exclusive breastfeeding, and access to emergency obstetric and neonatal care.
Empirical studies done in the case of India on the subject showed that generally, the rate of neonatal deaths and stillbirths stem from inadequate care during pregnancy, inappropriate management of complications during pregnancy and delivery, poor hygiene during delivery and the first critical hours after birth, and lack of newborn care. Several factors such as women's status in society, their nutritional status at the time of conception, birth spacing, mother's stature, antenatal care visits, early childbearing, too many closely spaced pregnancies and harmful practices. We think that various other causes may influence neonatal deaths. These include factors such as women's education which may be an important instrument for combating neonatal and infant mortality insofar as literate mothers are more likely to immunize their children and improve their nutritional status. Acquiring knowledge on improved child feeding practices, food preservation and better sanitation is as a key to breaking the cycle of malnutrition. It is within this framework that our paper seeks to examine the impact of female literacy on neonatal deaths and stillbirths in India. As we discussed earlier, the rise in neonatal mortality urges us to identify such relationship to search for short-run and long run correlation because it is of critical importance in the evaluation of perinatal programs designed to reduce mortality. So how can energy consumption (renewable and non-renewable), economic growth, working mother and female literacy effect neonatal mortality in India?. It appears that non-renewable energy consumption increase CO2 emissions, which means the amplify of pollution and effect positively the neonatal mortality rate. However, CO2 emissions is typically reduced if governments use more renewable energy resources.
To answer the previous question and to verify the proposed hypotheses, we employed ARDL bound testing approach suggested by Pesaran et al. (2001) during the period between 1970 and 2021 for Indian data.
In order to identify the factors that cause neonatal mortality in India and the decisions to be taken to limit this phenomenon as much as possible, we used a quantitative analysis. Our research is structured as follows. In “Literature review”, we identify the literature review recapitulates the recent study outcome on the relationship among neonatal mortality, energy consumption (renewable and non-renewable), economic growth, female literacy and working mothers. “Methodology and data” introduces the methodology and data. “Estimations and results” presents the estimation and results of different tests and the discussions of results is classify in “Discussions”. Finally “Conclusion and policy implications” provides our conclusions and policies implications.
Literature review
According to health economic literature, neonatal mortality is higher among infants born to mothers in rural areas, least wealthy households, and socially disadvantaged castes and ethnic groups. Similarly, neonatal mortality rates are particularly high for babies born to mothers with no education or to mothers who are young (under age 20) or old (over age 35), or who had made few antenatal care visits, and babies who had poor immediate newborn care. Also, neonatal mortality is higher among babies born in households with indoor air pollution or in households without access to improved water and sanitation facilities, and among babies born to mothers who are not exposed to public health broadcast media, Paudel et al. (2013). Aidonojie et al. (2022), Eteng et al. (2022a) and Otto et al. (2022) studied the water consumption as natural resource. They confirm that the amount of water consumed differs between men and women and between different ages. Clean water is important to maintain the good health of the individual and to fight against various diseases and viruses.
High temperature and poor air conditioning are the most prominent problems faced by cities with high population density as a result of industrial progress and globalization, which may negatively affect the health of individuals, including infants. In this context, a study by Modi et al. (2022) confirmed that the growth of the size of the yard positively affects the rise in air temperature, the average radiant temperature in the place and the physiological temperature. Dar and Ahmad (2022) and Maiwada and Jamoh (2022) suppose that technology (technology mobile as example) was an essential element to realize sustainable development goals. Among these goals, technology can develop and save the environment. It appears that technology mobile factory helps to finance health and education sectors and to premature sickness detection.
The evidence in the literature suggests also that female education creates social gains by improving women's and child health through the reduction in fertility rates and school education (Subbarao and Raney, 1992). Educated women may get greater opportunities in decision making process in family matters, along with getting permission by household members to develop strategies for improvement of their children health (D'Souza and Bhuiya, 1982). Terra De Souza et al. (1999) and Adhikari and Sawangdee (2011) show that investments in female education would have substantial positive effects on reducing neonatal mortality rate.
A more empirical set of papers done on the subject suggest that mother's education is a significant determinant of neonatal mortality. Schultz (1993) finds that, a one-year increase in women's education is associated with a 5% decline in childhood mortality. A related literature finds that mothers’ schooling leads to decline in child mortality; presumably because they better manage child care by more effectively administering food and medical care. As suggested by Cutler et al. (2006), the importance of female literacy is likely a result of the fact that as primary care takers, they are most likely to implement the health behaviors that can improve their children's health. To the extent that education improves an individual's ability to undertake these changes, more educated mothers will have healthier babies. Audrey et al. (2014) show that in long term, infant mortality has a significant and positive effect on fertility rate. They find that women's child behavior decisions are not affected by their employment state. A study conducted in 28 Indian states, Anil and Shraddha (2014) analyze the affect of female literacy on infant mortality. The two authors check that states which have advanced more on the female literacy front minimize infant mortality at a nearer step and this should stimulate and inspire smaller literate states to develop and strengthen their efforts to increase female literacy. Studying the Sub-Africa countries case, Shapiro and Tenikue (2017) prove that an increase of women literacy by 54% causes a reducing in mortality of children by 30% in urban areas. In rural areas, an increase of woman literacy on average by 30% can reduce children mortality on average by 35%. This empirical result confirms clearly the important role of women's education and literacy rate in general to survive humanity and to stimulate economic growth (inconsistent with the findings of Ndem et al., 2022).
In another hand, several researchers have examined the relationships between energy consumption (renewable and non-renewable) and economic growth. In this area, Alsaleh et al. (2021) have founded that bioenergy consumption effect positively the economic growth of EU-28 region and the relationship among this two variables is stable in long term. During 1990–2018 periods and using Generalized Least Squares (GLS) on EU-28 region data, Alsaleh et al. (2021) have confirmed that the increase of bioenergy consumption boost the adult mortality rate more intensively in the EU-15 developed regions than in the underdeveloped EU-13 regions. The use of hydropower energy as renewable energy has efficiently reduced the carbon dioxide emissions in European Union. This result was founded by Alsaleh and Abdul-Rahim (2022). In addition, Alsaleh et al. (2021) confirm that renewable energy utilization indicated by bioenergy can negatively affect the carbon dioxide emission (case of 28 countries of EU). CO2 emissions increase by1.3% and 0.23% during 1990–2020 periods in Russia respectively if energy consumption and industry increase by 1%. In addition, CO2 emissions decrease by 4.29% if forest area capacity enlarge by 1% in the long term (Raihan and Tuspekova 2022).
We note that most, if not all of the previous research (which we mentioned earlier) were studied the impact of excessive use of non-renewable energy on the economy (in terms of efficiency, cost and sustainability) and on the environment (in terms of greenhouse gas emissions and their impact on the environment). Most studies have confirmed a strong correlation relationships between non-renewable energy consumption and the economy, and they have proven the negative impact of non-renewable energy consumption on the environment through increased carbon dioxide emissions. In Jordan case, Adebanjo and Adeoye (2022) confirm that economic growth has in same time a positive and negative consequences on air pollution; and by using of Granger causality test; the researchers are founded a causal relationship from economic growth to air pollution. The use of non-renewable energy can sway negatively the economic growth in ten of Sub-Saharan Africa, and this negative effect can be explain by the depletion of this resources; Adebanjo and Shakiru (2022). Studying the relationships among energy consumption and economic progress, Jamil (2022) shows that oil; gas and electricity are an important factors in long and short term for the economic and a unidirectional causality relationship exists running from energy to economic progress. The increase in costs of these energies can cause some economic problems; so the use of renewable energy like nuclear power, wind and solar can be considered as a solution for these problems. Jeon (2022) has studied the relationships between CO2 emissions, renewable energy and economic growth in 48 American states. He was confirmed that economic growth has a direct impact on environmental degradation by the increase of CO2 emissions. Banerjee (2022) discus on the importance of Foreign Direct Investment course in energy sector in the midst of different Asian regions.
In addition, many of studies have confirmed that renewable energies have a positive effect on reducing carbon dioxide emissions and their effective role in the economy. But not all of these works have mentioned a very important issue, which is the effect of these factors on the health and lives of infants in the short and long term. Therefore, we think that it is important to address this issue through this research.
Methodology and data
The objective of this paper is to analyze the impacts of renewable energy consumption, non-renewable energy consumption, economic growth, working mother, female literacy (as exogenous variables) and neonatal mortality (as endogenous variable) in India using annual data over the period of 1970–2021. Earlier, most existing literature generally supposes that female literacy would likely lead to reduction in child mortality. It has also established that parental education on general is often a key determinant of infant mortality.
Data
In specifying the child mortality model, a set of explanatory variables, drawing on the existing literature on the determinants of neonatal and stillbirth deaths, includes, in addition to female literacy variable, six other variables which are identified by health economics literature as key determinants of child health: this the quality of institutions measured by control of corruption compiled by International Country Risk Guide. The medical density, which is defined by physicians as per thousand populations and used to account for the supply of healthcare, can be considered as a key determinant of NM rate. Renewable energy consumption was used in model as an exogenous variable because it has an impact on reducing CO2 emissions (Grodzicki and Jankiewicz 2022) and then it can ameliorate mothers health. However, economic growth, CO2 emissions and non-renewable energy consumption represents as three exogenous variables serve to increase pollution (Li and Haneklaus 2021) which means they serve to aggravate living conditions cleanliness of the environment (environment is necessary condition for human development capital; Eteng et al., 2022b). We have choosing the educated woman, firstly because she is the primarily responsible for the child life, and secondly the educated woman is usually able to take better care of her health and that of her young child. Finally, we have introducing the variable defined by working mother and more precisely in agriculture sector, for the reason that agriculture sector is a very hard work and it requires a lot of physical effort which may adversely affect the health of the fetus.
This study aims to analyze the short and long run relationships between neonatal mortality, energy consumption, female literacy, CO2E and working mother in India during 1970–2021 periods. Our endogenous variable was defined by neonatal mortality (Jemal et al., 2022), and the rest of variables represent the exogenous variables.
Methodology
To empirically investigate the relationships between our different variables, an ARDL bound testing approach suggested by Pesaran et al. (2001) is employed to investigate the short-run dynamics and long run relationship. The specification of this model is consistent with the literature and allows for the identification of the channels through which mother's education and other variables affect neonatal mortality.
we prefer to use the ARDL technique for economic and econometric reasons. In econometric terms, the ARDL allows us to make estimates for reduced samples and for variables that have the same or different order of integration provided that these variables should be integrated of order zero and/or order one. In economic terms; the ARDL approach allows us to detect the short and long term effects of the independent variables (renewable energy consumption, non-renewable energy consumption, economic growth, working mother, female literacy) on the dependent variable (neonatal mortality).
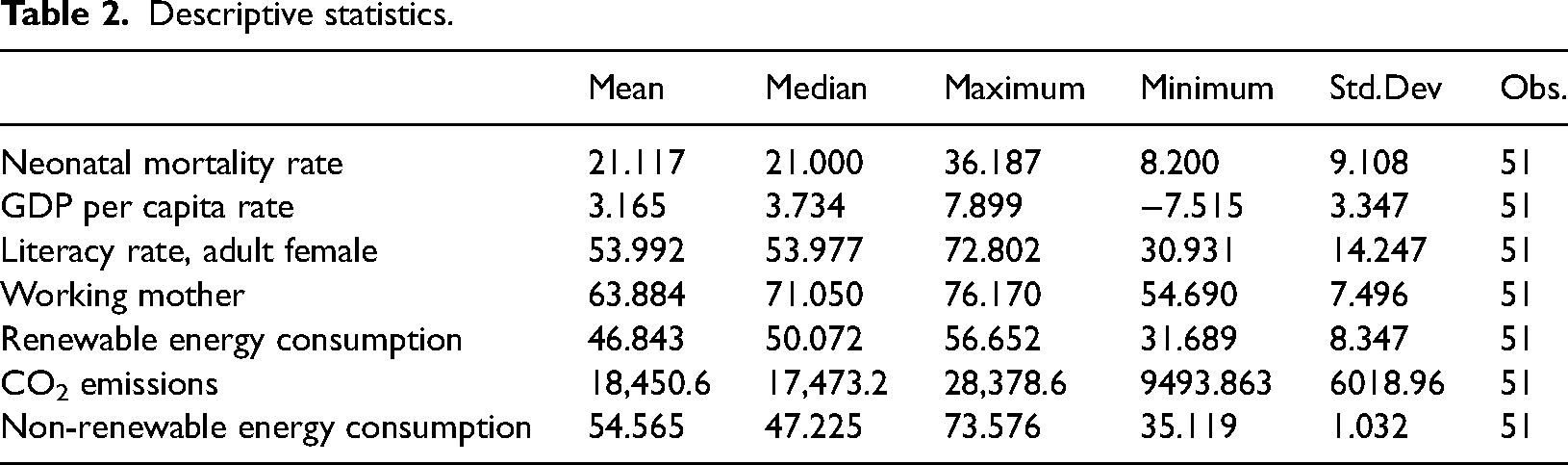
We start our study by description data (mean, median, maximum, minimum). In second step, we defined the econometric model by writing the ARDL and VECM models. The results of tests and estimates are designed in step three.
Data and their descriptive statistics are represented in Table 1 as follows:
Variables descriptions.
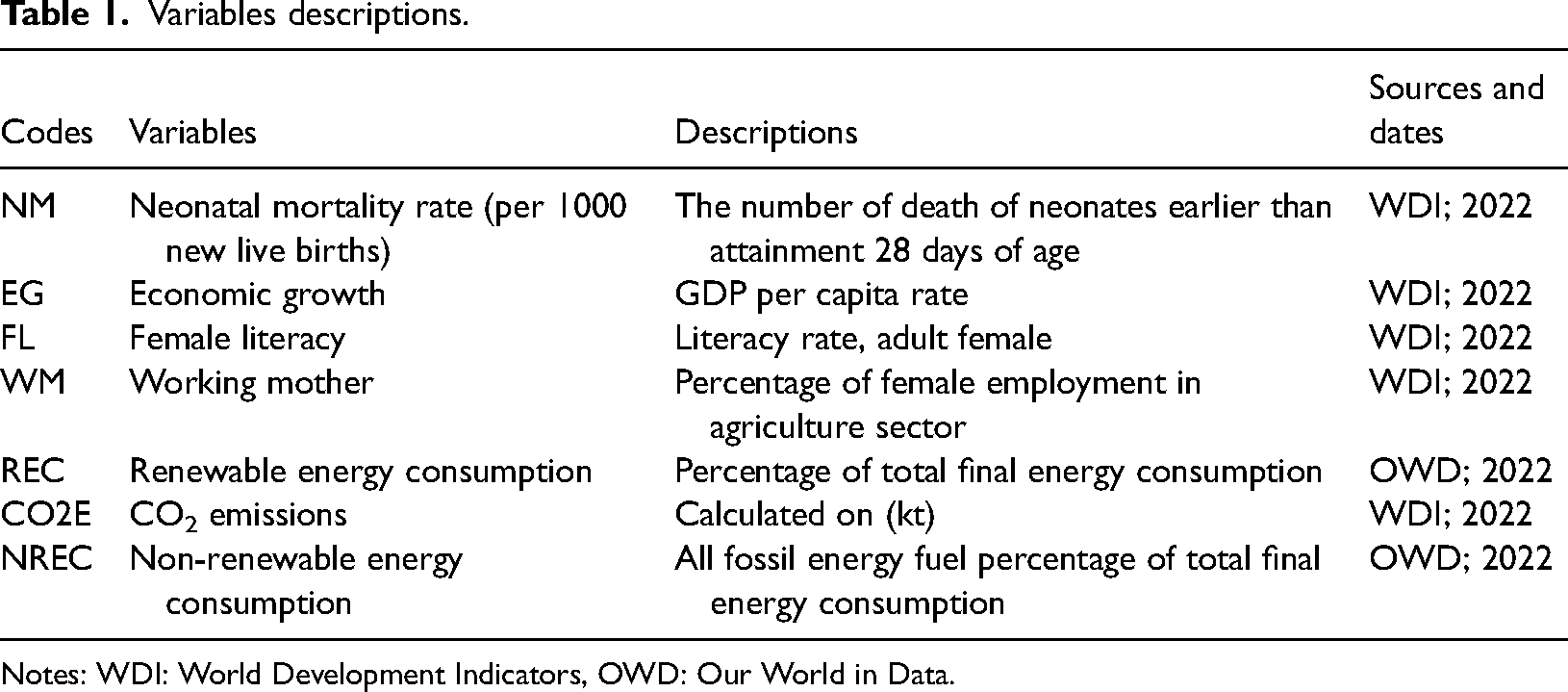
Notes: WDI: World Development Indicators, OWD: Our World in Data.
Descriptive statistics.
We developed the empirical model based on the production function having constant returns and the combined output function with time t, can be displayed as follows:
The econometric model used to examine becomes in the following form: t: White-noise disturbance term.
NM is neonatal mortality rate; FL is female literacy rate (adult); WM is working mother; NREC is non-renewable energy consumption (%GDP); EG is economic growth rate; REC is renewable energy consumption gap at $1.90 a day and finally CO2E is CO2 emissions, expressed as a logarithm function. The variables are from World Health Organization (2021), World Bank (2021), Indian Education Ministry (2021a) and Indian Health Ministry (2021b).
In order to analyze the impacts of different exogenous variables on the endogenous variable, we rely on ARDL bounds testing approach (Pesaran et al., 2001; Pesaran and Shin, 1999). Our standard empirical model was inspired from the study of Jebli and Youssef (2015) and Wang et al. (2020) in which we use the standard Cobb-Douglas production function to approximation the practical model through constant returns and time t as combined output of function.
In the condition of existence of long-term cointegration, the ARDL model is written in the following form: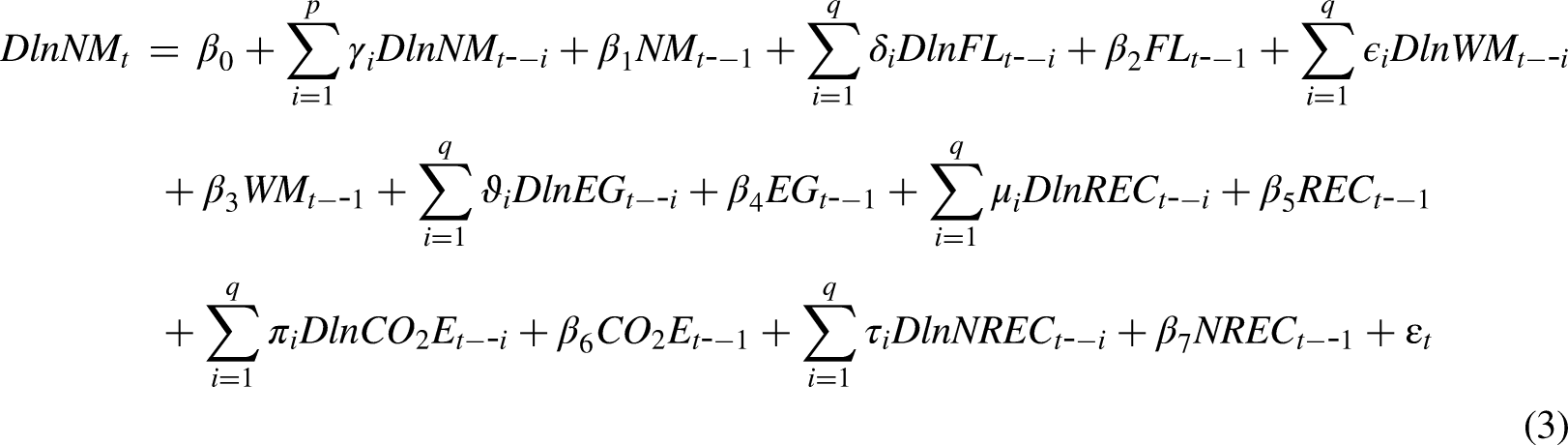
γ, δ, ɛ, θ, ϑ, μ, π and τ are error correction dynamics.
The test of cointegration is carried out using the autoregressive distributive lag model (ARDL) approach due to Pesaran et al. (2001) where we estimate five unrestricted error correction considering each variable as a dependent variable. It follows the ARDL bounds testing approach to cointegration developed by Pesaran et al. (2000), and latter on by Pesaran et al. (2001). Haug (2002) has argued that ARDL approach to cointegration provides better results for small sample data set such as in our case as compared to traditional approaches to cointegration i.e. Engle and Granger (1987); Johansen and Juselius (1990) and Phillips and Hansen (1990). Another advantage of ARDL bounds testing is that unrestricted model of ECM seems to take satisfactory lags that captures the data generating process in a general-to-specific framework of specification (Laurenceson and Chai, 2003). This method avoids the classification of variables as I (1) and I (0) by developing bands of critical values which identifies the variables as being stationary or non-stationary processes. Unlike other cointegration techniques (e.g. Johansen's procedure) which require certain pre-testing for unit roots and that the underlying variables to be integrated are the same order, the ARDL model provides an alternative test for examining a long-run relationship regardless of whether the underlying variables are purely I (0) or I (1), even fractionally integrated. Therefore, the previous unit root testing of the variables is unnecessary. Moreover, traditional cointegration method may also suffer from the problems of endogeneity while the ARDL method can distinguish dependent and explanatory variables. Thus, estimates obtained from the ARDL method of cointegration analysis are unbiased and efficient, since they avoid the problems that may arise in the presence serial correlation and endogeneity. Note also that the ARDL procedure allows for uneven lag orders, while the Johansen's VECM does not. However, Pesaran and Shin (1999) contented that, appropriate modification of the orders of ARDL model is sufficient to simultaneously correct for residual serial correlation and problem of endogenous variables.
One the presence of cointegration between the variables is verified, we practice the VECM Granger causality approach in order to explore the direction of causality between variables.
The VECM is a restriction of VAR. The ECT (error correction term) represent a cointegration term and it makes the endogenous variables to converge to the cointegration relationships whereas agreeing for short-term dynamic adjustments. By using The VECM, it can be possible to estimate the short-term relationships and the ECT gives the opportunity to verify the existence of long-term relationships.
The short-run causal relationships will be modeled by using a vector autoregressive framework (VAR) as follows (Narayan and Smyth, 2006):

Estimations and results
The first step in our study before determinate the relationship between variables, it is to check the stationarity of each variables in order to define their order of integration. To do this, we have used ADF and DF-GLS unit root test. The null hypothesis (H0) indicates the presence of unit root. If H0 was not verified, so our econometric study can be progressed. In second step, we employ the Wald test and the Bounds test to detect the cointegration in long term between variables. This test was based on calculate of F-statistic and to compare it with the critical values. Then the optimum lag is choosing by minimizing the Akaike Information Criterion (AIC) and Shwarz Criteria (SIC). For the four models, we founded that lag 2 is the optimal lag length for our research. The results of Bounds test (Table 3) show F-statistics lies above, at least, the 10% upper bound. In this case, we can confirm the existence of cointegration in long run between variables.
Bounds test for cointegration.
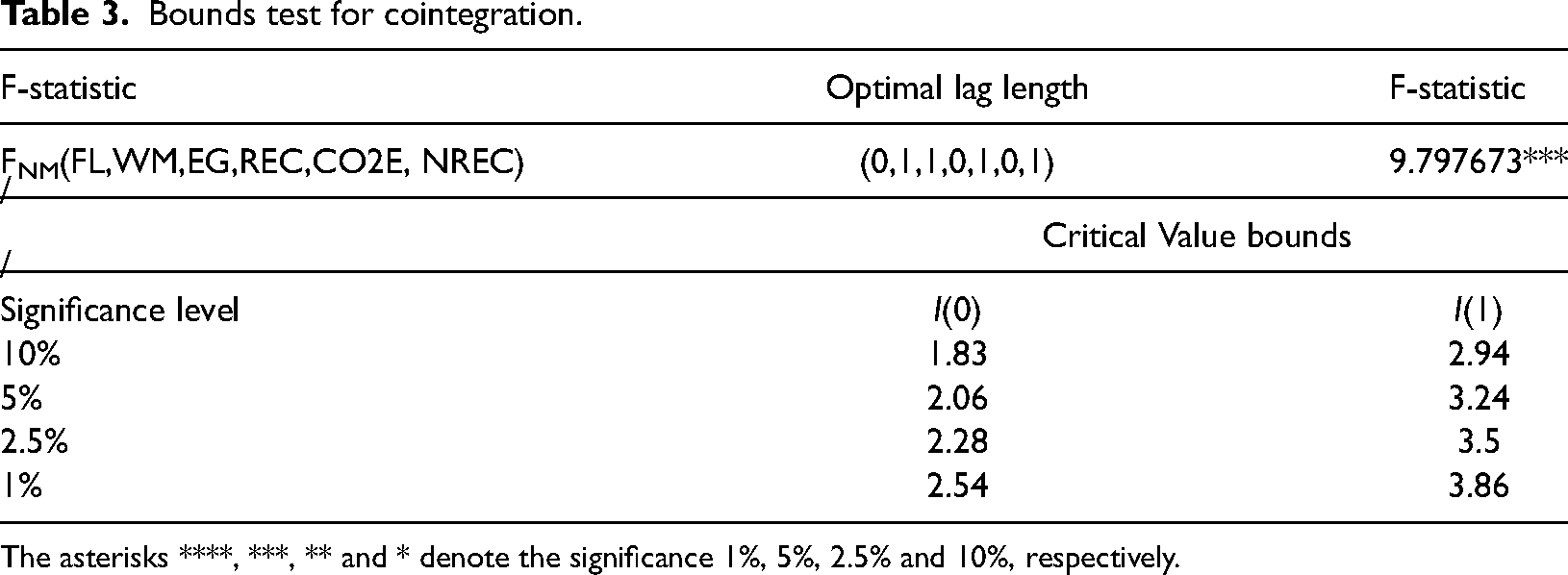
The asterisks ****, ***, ** and * denote the significance 1%, 5%, 2.5% and 10%, respectively.
Integration order
The unit roots tests was used in order to define the order of integration of each variables. The results in Table 4 indicate that all of our variables are stationary in first difference which means that the null hypothesis was rejected in this case.
Results of unit root tests.
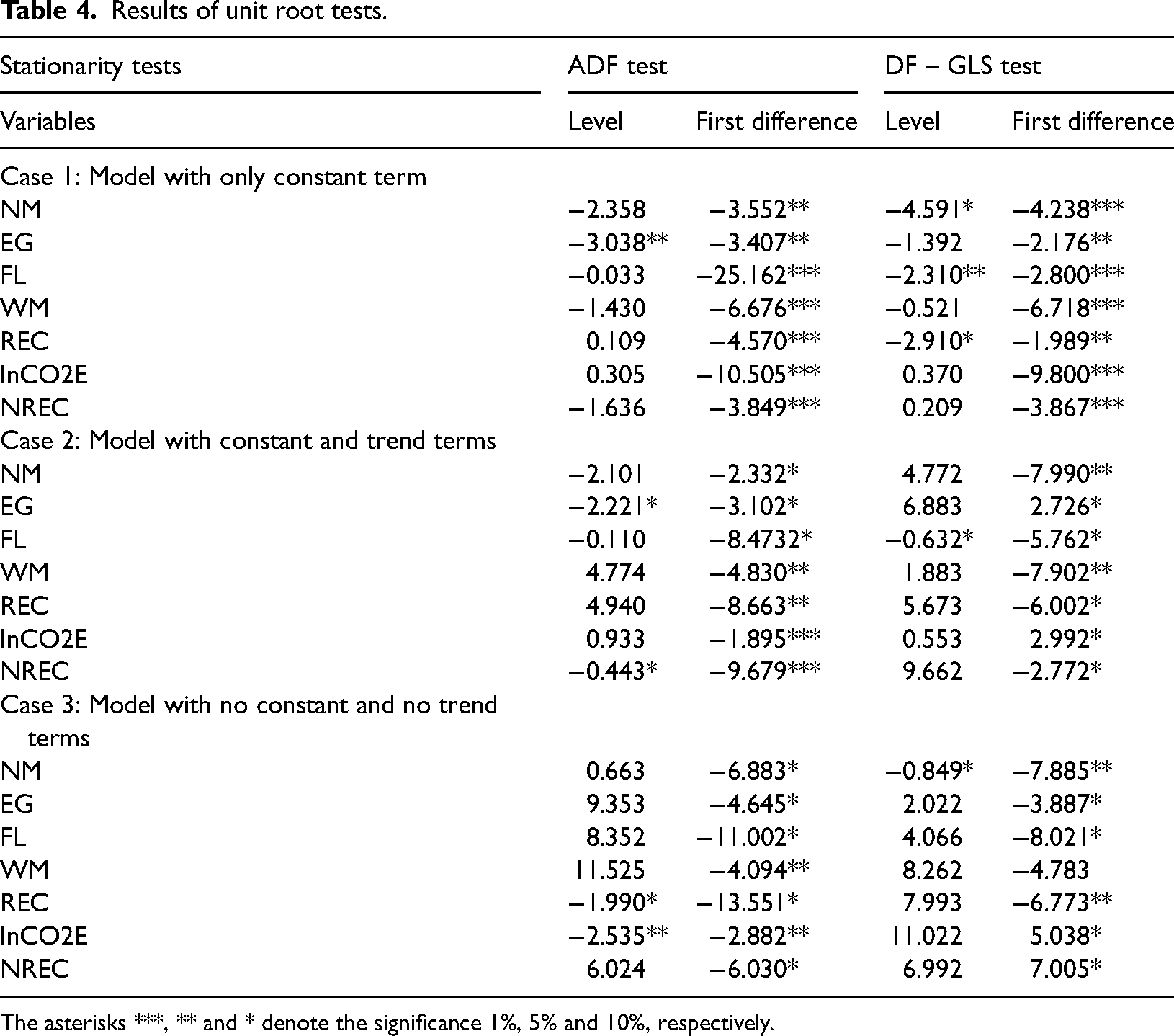
The asterisks ***, ** and * denote the significance 1%, 5% and 10%, respectively.
Wald test
The Wald test was applied in order to verify to existence of long-run cointegration relationship between neonatal mortality and the six explicative variables.
The test is based on two hypotheses H0 and H1 as follow:
H0 means the absence of long-run cointegration relationships between our variables, while H1 indicates the existence of long-run cointegration relationships.
The results indicated in Table 5 show that the F-statistic value is significant at the 10% and 5% thresholds whish confirm the existence of long-term cointegration relationships between the endogenous variable and the exogenous variables.
Wald test.
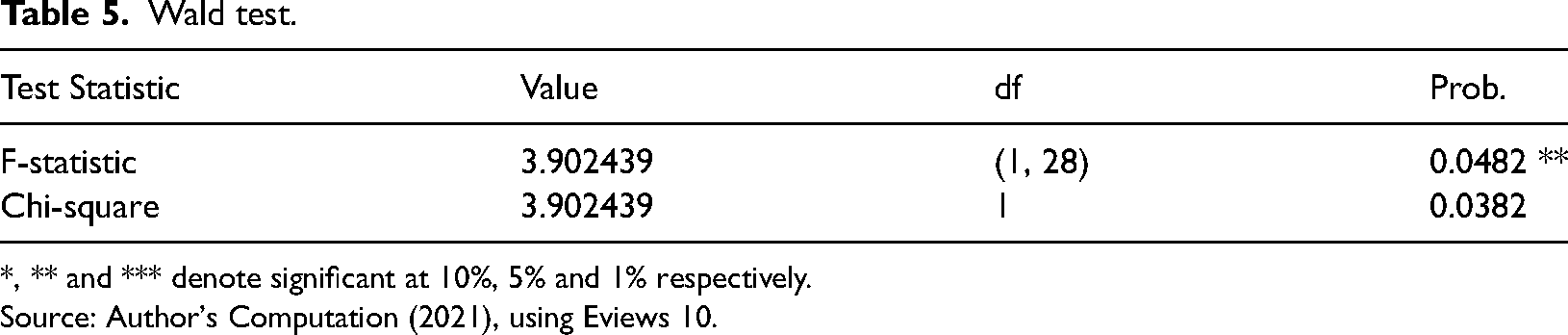
*, ** and *** denote significant at 10%, 5% and 1% respectively.
Source: Author's Computation (2021), using Eviews 10.
Bounds test
The Bounds test is used to verify the existence of long run relationships between all variables of econometric model. The results indicated in Table 3 indicate that the value of F-statistic is significant at the 10%, 5%, 2.5% and 1% thresholds whish confirm the existence of long-term relationships between variables.
Null Hypothesis: No long-run relationships exist.
CUSUM and CUSUMSQ tests
We have employed the CUSUM and CUSUMSQ tests to verify the stability of ARDL model. The results appeared in form of two figures where statistics should be between the critical bounds and this is the case of our study (Figures 1 and 2)
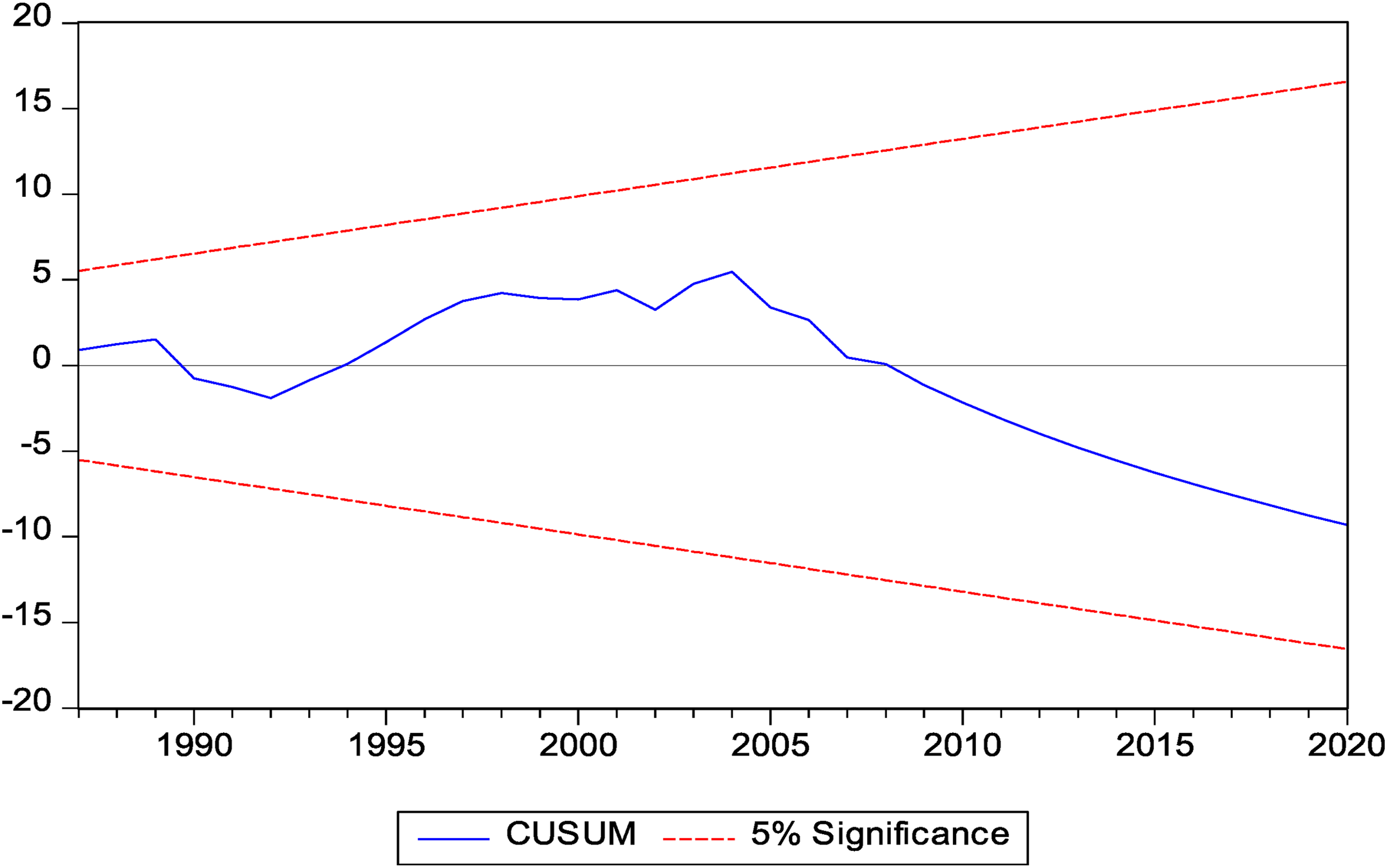
CUSUM test.
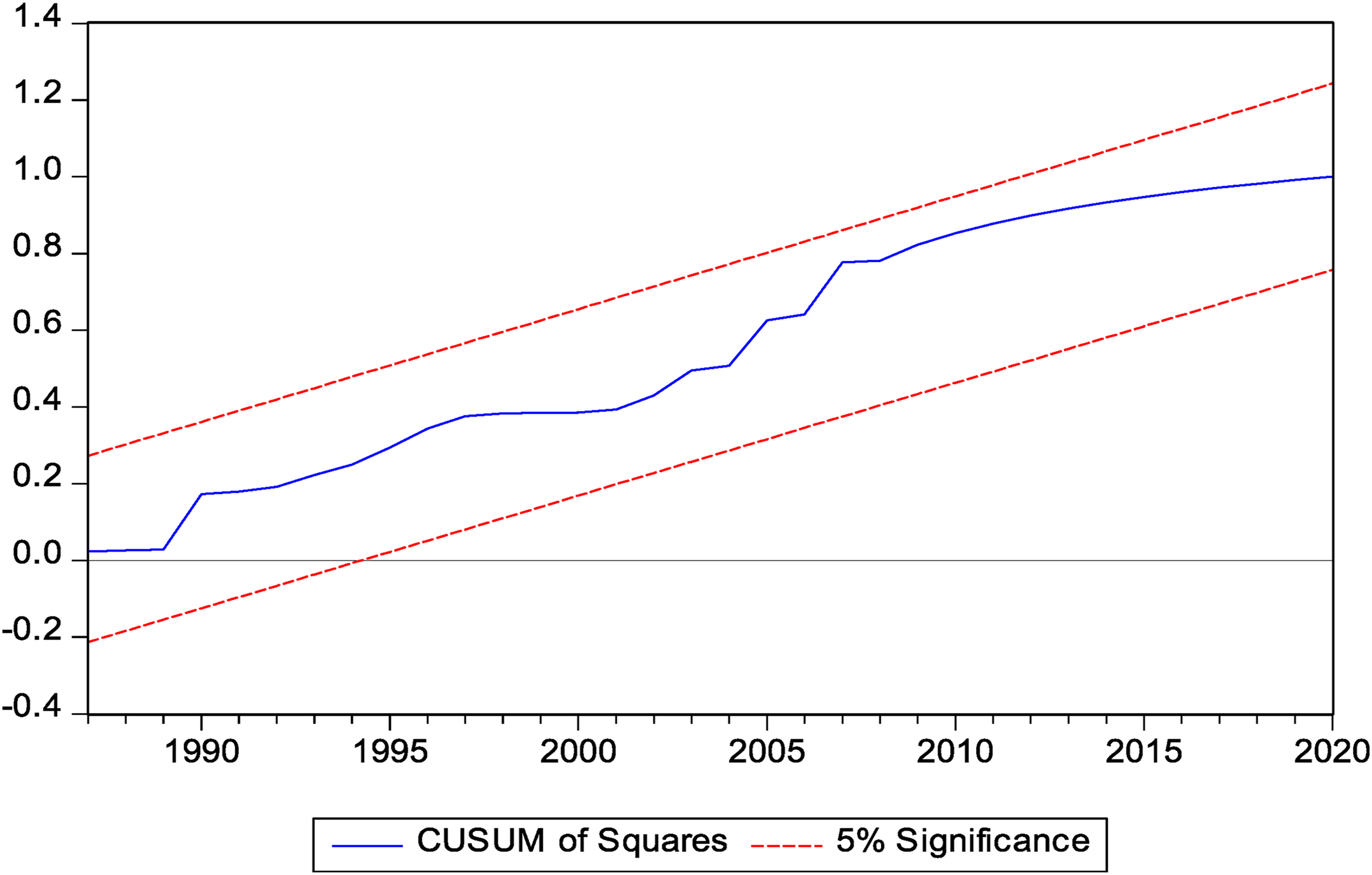
CUSUMSQ test.
Diagnostic tests
In Table 6 we have employed Breusch-Godfrey serial correlation LM test in order to detect the correlation of residuals. The results of each models show that there is no serial correlation for residuals in both models. The results of ARCH test indicate that the four models are free from heteroscedasticity and the normal distribution characterizes the distributions of error terms.
Diagnostic tests.

ARDL short-run dynamic estimation
After confirmation the existence of cointegration for all four models according to results of Bounds test, we can now estimate the long and short-run coefficients.
In Table 7, we found the different results of short-term estimation. It appears the existence of three positive relationships between FL, NREC, CO2E (at date t and at date t-1) and NM and also four negative relationships between FL (at date t-1), WM (at date t-1), EG (at date t-1), REC and NN.
ARDL short-run dynamic estimation.
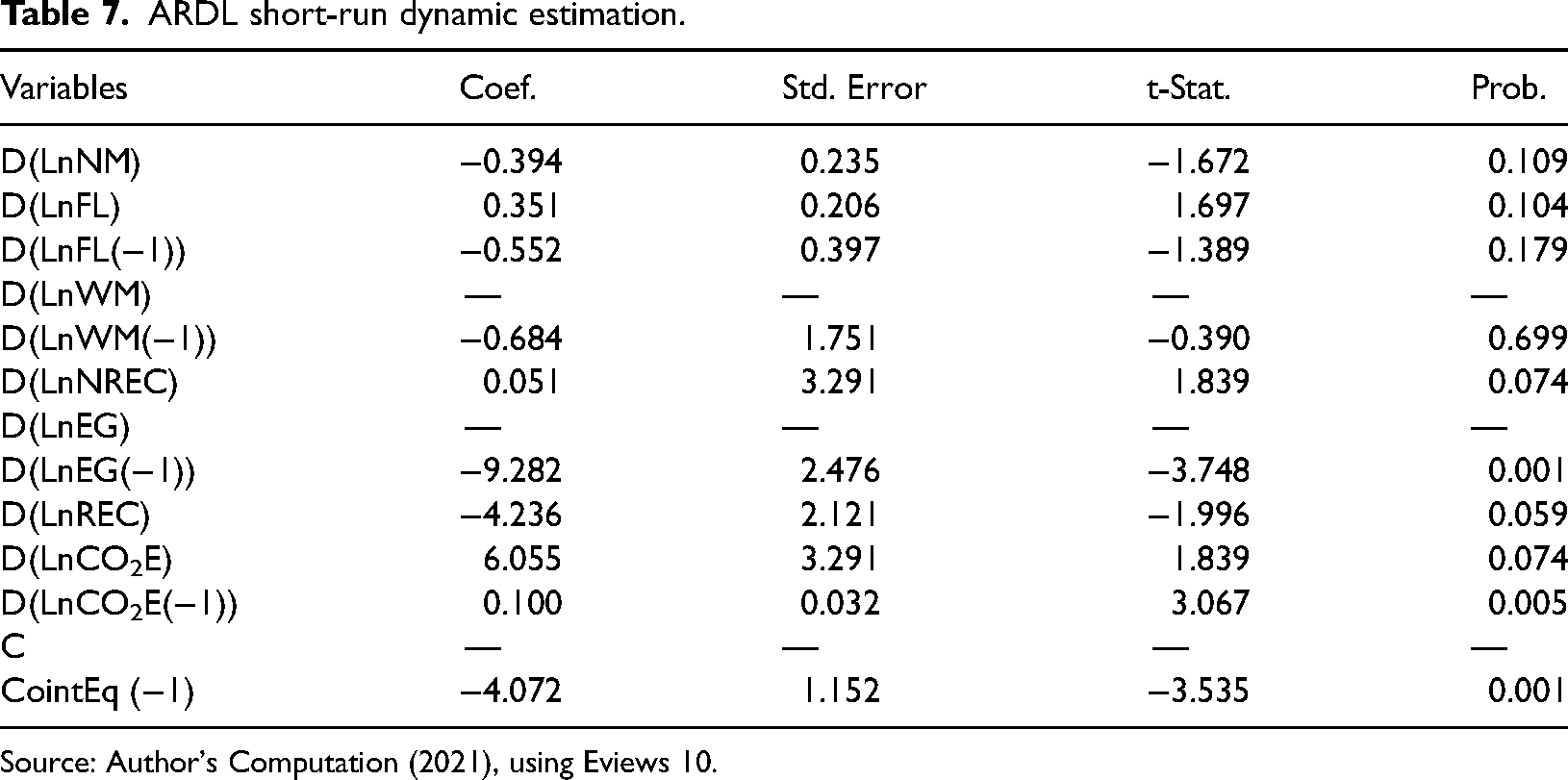
Source: Author's Computation (2021), using Eviews 10.
The notion CointEq (−1) identify the delayed residue creating from our equation of the equilibrium in long-run. The negative coefficient and its significance verify the existence of an error correction tool. The coefficient of cointegration makes clear the arrangement will be mobilized towards the long-term object. In our case, this coefficient is equal to - 4.072, thus defined a utilization to the proportionally quick long-term target.
ARDL long-run dynamic estimation
The different results of ARDL long-run coefficients are situated in Table 8. We show that FL, EG and REC have negative and significant impacts on Indian NM. An increase by 1% of these three variables leads to decrease NM respectively by 2.39%, 0.18% and 2.65% in the long-run. The finding confirms that education (Lai et al., 2015), economic growth (Erdoğan et al., 2013; Van Den Berg et al., 2020) and the use of renewable energy (confirmed by Mohammed and Akuoko, 2022 and contradictory by Alsaleh et al., 2021; case of 15 developed regions of EU) have a major role in reducing of NM in India.
Long-run estimated coefficient.
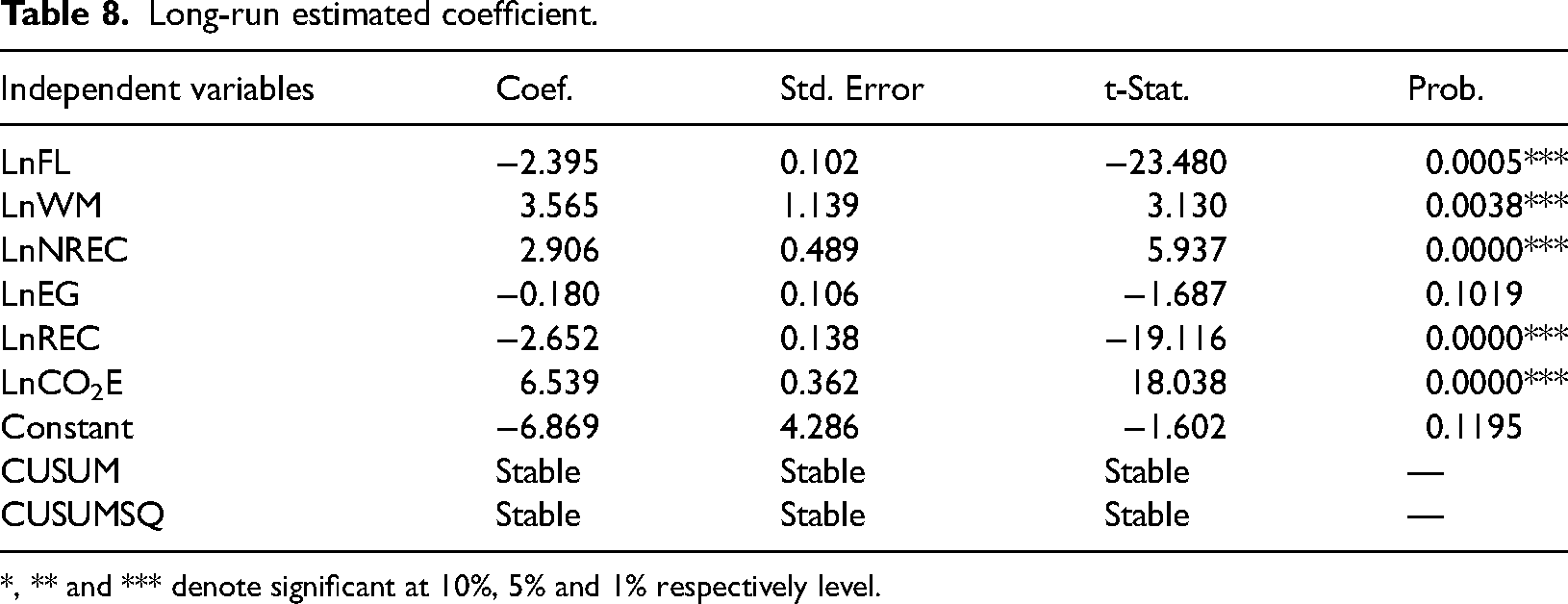
*, ** and *** denote significant at 10%, 5% and 1% respectively level.
By contrast, an increase by 1% in WM 1% in NREC and in 1% in CO2E (Stine et al., 2019; Cañadas et al., 2021) will lead to increase of NM respectively by 3.56%, by 2.9% and 6.53%. This result shows that mother working, pollution and non-renewable energy consumption strongly and positively affect NM whish threaten infant's lives.
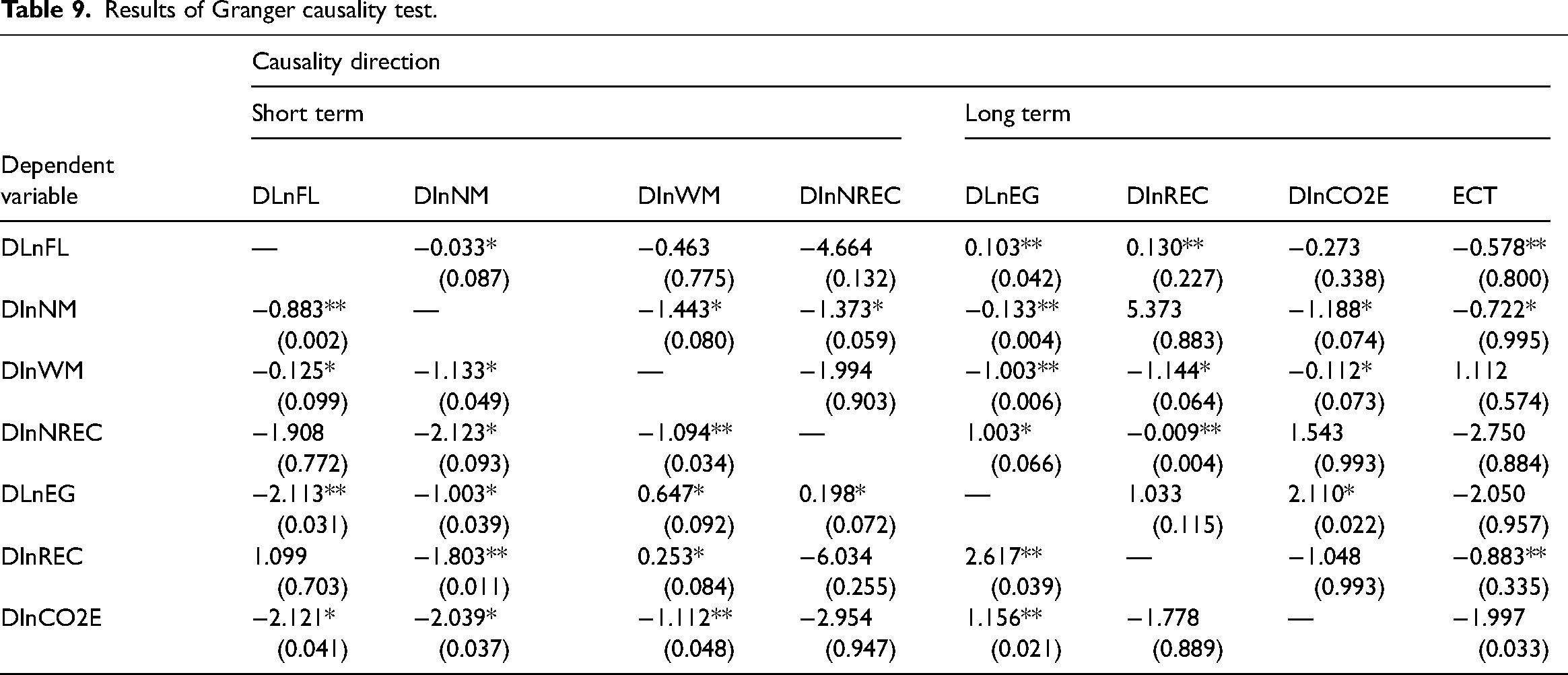
Granger causality and ECT tests
After determining the long-run coefficients by using ARDL approach, we move on to the next step to find the short-run relationship and the rate of long-run adjustment by using the Granger causality technique. Table 8 recapitulates the different results of Granger causality estimate. As results, we show that NM has four bidirectional causal relationships with FL, NREC, EG and CO2E. In addition, there is one negative unidirectional causal relationship when WM affects NM. The FL variable has one bidirectional relationship with NM and it was influenced by four negative unidirectional relationships from WM, NREC, EG and CO2E and by one negative unidirectional causal from REC. There are three bidirectional relationships between WM and NM, between WM and EG and between WM and CO2E. Also there are two negative unidirectional relations where WM influences FL and REC. NREC has two bidirectional relations with NM and EG and two negative unidirectional relations with WM and REC. Concerning the EG variable, we find that this variable has two bidirectional causal relationships with FL and NREC and two positive unidirectional causal relationships with WM and CO2E. The Granger causality estimate shows that REC positively affects and EG and it negatively affects NM. However, this variable has a bidirectional relation with WM. Finally, CO2E has three bidirectional relations with NM, WM and EG and only one negative unidirectional relation with FL. The different results of Granger causality estimate are located in Table 9.
Results of Granger causality test.
Discussions
The results of short-run and long-run estimations show that FL, REC and EG effect negatively NM rate in India during 1970–2020 periods. Economically, educated mother can take care of herself and her baby, for example by following a healthy diet for herself and her baby, also by knowing the dates of control and vaccinations and by following the instructions of specialist doctors. Reliance on non-renewable energies has catastrophic effects on the health of individuals and the environment through the increase in emissions of toxic and greenhouse gases such as carbon dioxide (CO2), resulting in high temperatures and high poisoning cases. Usually, infants and pregnant women are the most prominent victims. On the other hand, we see that economic growth and the exploitation of renewable energy sources contribute to reducing the infant mortality rate (This result is inconsistent with the findings of Alsaleh et al., 2021; case of 28 developed regions of EU. The use of clean energies reduces the emission of toxic gases, and at the same time, economic growth contributes to an improvement in the standard of living through improved health, education and nutrition.
Conclusion and policy implications
The main objective of this research study is to explore the causes of neonatal mortality in India and to define the causal relationships between neonatal mortality, female literacy, energy consumption and fertility. In order to attain our goal, we have performed in first part of study a spatial analysis using maps. In second part of study, we have used annual data from 1970 to 2020. Assumed a multi-step process, we started from stationarity tests to Bound tests for Cointegration, to ARDL approach and finished to VECM method. We observe that neonatal mortality rate increases as function of rural rate and it decreases as function of female literacy rate. In second part of study, the ADF and DF-GLS results show that all variables are stationary in first difference. The Bounds test results confirm that there is a long run cointegration between variables. The ARDL estimate proves that FL, WM, NREC and EG have significant roles in reducing of NM rate in India. By contrast, REC and CO2E strongly serve to increase NM.
The VECM results give mixed results for Indian country. The overall results indicate that NM variable has bidirectional causal relationships with all of these variables FL, NREC, EG and CO2 emission. In addition, we find a negative unidirectional causal relationship running from REC to NM.
To summarize, the results of short and long-run show and confirm that FL, EG and REC are an essential elements in reducing of NM rate in India. So, it is important to note that it is necessary to provide the basic necessities of life for mothers, such as education and health care in order to reduce neonatal mortality. By contrast WM, NREC and CO2E favorite the increases of NM rate. From these results and conclusions, we can suggest that mother's education, mother's health, investment in new resource of energy with zero emissions of CO2 and clean environment are considered as keys and prominent determinants of child survival in India.
The empirical results obtained in our study and the discussion that followed from them have several important lessons and policy implications for those involved in designing health programs to improve the health status in general: The multi-factorial nature of neonatal mortality implies a multidisciplinary intervention strategy, involving pre and perinatal prevention. Government and donors should focus their programs to address causes and determinants of neonatal deaths, primarily in the early neonatal period, and should focus on improving the utilization of maternal health care services because it has been established that child survival depends on improved quality of clinical care for mothers, emergency obstetric care and emergency neonatal care. Also, neonatal intensive care units with qualified personnel must be developed because it would contribute to reducing neonatal mortality especially in premature newborn.
To identify the factors behind neonatal mortality in India, we suggest that it is necessary to improve female literacy rates, to more invest in social sector programs, to improve access to clean air especially in New Delhy capital. Also, it is necessary to set up an efficient training system, covering all health care professions, to invest in the pharmaceutical industry and in the thalassotherapy. We think also that Indian government should support the poor and middle class by providing grants and financial aid; especially compulsory and free vaccinations for the newborns. Through the results obtained in this scientific research, it is imperative for the Indian government and politicians to focus on how to discover and make a good use of renewable energy through the increase in the percentage of investments in this field. On the other hand, it's time to think seriously about how to reduce dependance on energy sources polluting for several political and economic reasons. Some of these reasons is including the reduction of dependance on exporting energies countries (like OPEC+), the high cost and instability of prices in the traditional energy market (while the renewable energy market is a promising market), as well as reducing of the global warming and the danger it poses to continuous heat and climate change. As for the humanitarian reasons, the most prominent of them is to preserve the safety of humanity from diseases and dangers. Finally, we can see clearly that economic growth can be considered as an essential factor to save infant's live. So, for this reasons, we can suggest that is possible for Indian government to maintain its pace of economic growth and at the same time to protect infant lives as a vulnerable group of society. We point out that we could have done a deeper study if we had available data related to each part of India. We hope that it will be available in the future, so that we can conduct a spatial regional study of this country.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.