
Abstract
This study investigated the relationship between consumers’ communication with doctors and their e-Health literacy and healthy behaviors based on the theory of reasoned action. Five communication activities were identified: following doctors’ social media accounts, reading doctors’ posts, responding to doctors’ posts, favoring (clicking “like” of) doctors’ posts, and recommending doctors to other patients. E-Health literacy and healthy behaviors were measured based on instruments used in previous literature. Survey method was used to collect data and a hierarchical regression analysis was used to analyze the relationship between communication activities and consumers’ e-Health literacy and healthy behaviors. We found that following doctors’ accounts (r = 0.127, P < .001), responding to doctors’ posts (r = 0.141, P < .001) and recommending doctors to others (r = 0.133, P < .001) were significantly associated with e-Health literacy, while following doctors’ accounts (r = 0.091, P < .001), responding to doctors’ post (r = 0.072, P < .01), favoring doctors’ posts (r = 0.129, P < .001), and recommending doctors to others (r = 0.220, P < .001) were significantly associated with healthy behaviors. Our study demonstrated that the social network communication between doctors and consumers could be cost-effective in improving intermediary consumers’ health outcomes. To be specific, following doctors’ posts, responding to doctors’ posts, favoring doctors’ posts, and recommending doctors to others were positively associated with consumers’ e-Health literacy and healthy behaviors. The results suggested that leveraging information technology could be an important tool to health policymakers and health providers in order to improve outcomes.
Firstly, more and more patients and doctors use social media to communicate with each other. Secondly, social media can change the communication paradigm between patients and doctors. Thirdly, social media are utilized to influence health outcomes such as health-related emotions, physical conditions, and beliefs.
Communicating with doctors via social media can improve consumers’ e-Health literacy and healthy behaviors. Active usage activities such following doctors’ social media accounts, responding to doctors’ post and recommending doctors to others was associated with e-Health literacy and healthy behaviors. Passive usage activity like reading doctors’ post may not bring benefits to improving e-Health literacy or healthy behaviors.
Firstly, doctors can pay more attention to their communication with patients on social media. Secondly, it is important to motivate patients to communicate with doctors on social media. Thirdly, Policy makers can consider integrating social media into healthcare service provision.
Introduction
E-Health literacy is an ability of using health information from online sources to address their health issues. 1 E-Health literacy has been found to improve hypertension control, 2 health self-efficacy, 3 and medication adherence, 4 etc. Meanwhile, healthy behaviors, including smoking cessation, physical activity, healthy eating, and moderate drinking, can reduce the probability of premature death. 5 Healthy behaviors are found to improve conditions including diabetes, 6 hypertension, 7 stroke, 8 etc. Thus, taking actions to enhance e-Health literacy and healthy behaviors is of great importance.
Social media could provide a novel way to improve consumers’ e-Health literacy and healthy behaviors. Since social media allow users to create and exchange content, they can change the communication paradigm between doctors and consumers from one-to-one communication into many-to-many communication. 9 Several social media communication activities can be conducted by users to communicate with doctors and others on social media. Based on previous literature about communication and usage activities on the social media, these activities include following doctors’ social network accounts (FOL), reading doctors’ posts (REA), responding to doctors’ posts (REP), favoring doctors’ posts (FIK), and recommending doctors to others (REC), etc.10-12 Thus, social media provide ample opportunities for the communication between doctors and consumers. Meanwhile, more and more consumers are using social media to communicate with health professionals or with other consumers, while more than sixty percent of doctors reported to make use of social media for different purposes.13,14 Thus, it is feasible to improve consumers’ e-Health literacy and healthy behaviors by communicating with doctors on social media.
Previous literature has studied the effects of social media on health outcomes such as health-related emotions, physical conditions, and beliefs. However, less is known about the effect of social media usage on e-Health literacy and healthy behaviors. 15 Although the previous literature has revealed the effect of physician-patient communication on patient outcomes including compliance, quality of life and recovery, few of them considered the role of social media context. 16 Although previous literature has implied that several interventions based on social media are useful in improving consumers’ health outcomes, the effect of consumers’ communication activities with doctors on social media on their e-Health literacy and healthy behaviors has not been studied.17-19 Thus, our research question is:
Can communication with doctors on social media influence consumers’ e-Health literacy and healthy behaviors?
In this study, we hypothesize that consumers’ communication activities with doctors on social media influences their e-Health literacy and healthy behaviors based on the theory of reasoned action. 20 According to the theory of reasoned action, one’s actual behaviors and behavioral intentions depends on their attitudes toward the behavior and subjective norm. When a consumer communicates with doctors on social media, they could receive health information, interact with doctors and form positive attitudes toward healthy behaviors by FOL, REA, REP, and FIK, while they could perceive their peers’ opinions by REC. Therefore, all communication activities between consumers and doctors on social media could affect consumers’ healthy behaviors and improve e-Health literacy.
Compared with traditional health promotion approaches that are implemented offline or intentionally, communicating with doctors via social media could be a low-cost and natural health promotion intervention. 21 Meanwhile, given that China has a large number of social media users, 22 consumers in China may have different social media usage patterns since China has different culture values from western countries. 23 Therefore, it is worthwhile to evaluate the effect of consumers’ communicating with doctors on social media on their e-health literacy and healthy behaviors in China. To measure social communication activities, we asked respondents how many doctors’ social network accounts they were following to measure FOL, while we asked respondents to report the frequency they performed aforementioned activities to measure REA, REP, FIK, and REC.11,12 To capture the dependent variables, items for e-Health literacy were adapted from Norman and Skinner, 24 while items for healthy behaviors were adapted from Kelly et al. 25 The specific healthy behaviors involved physical activity and healthy eating.
Materials and Methods
Setting
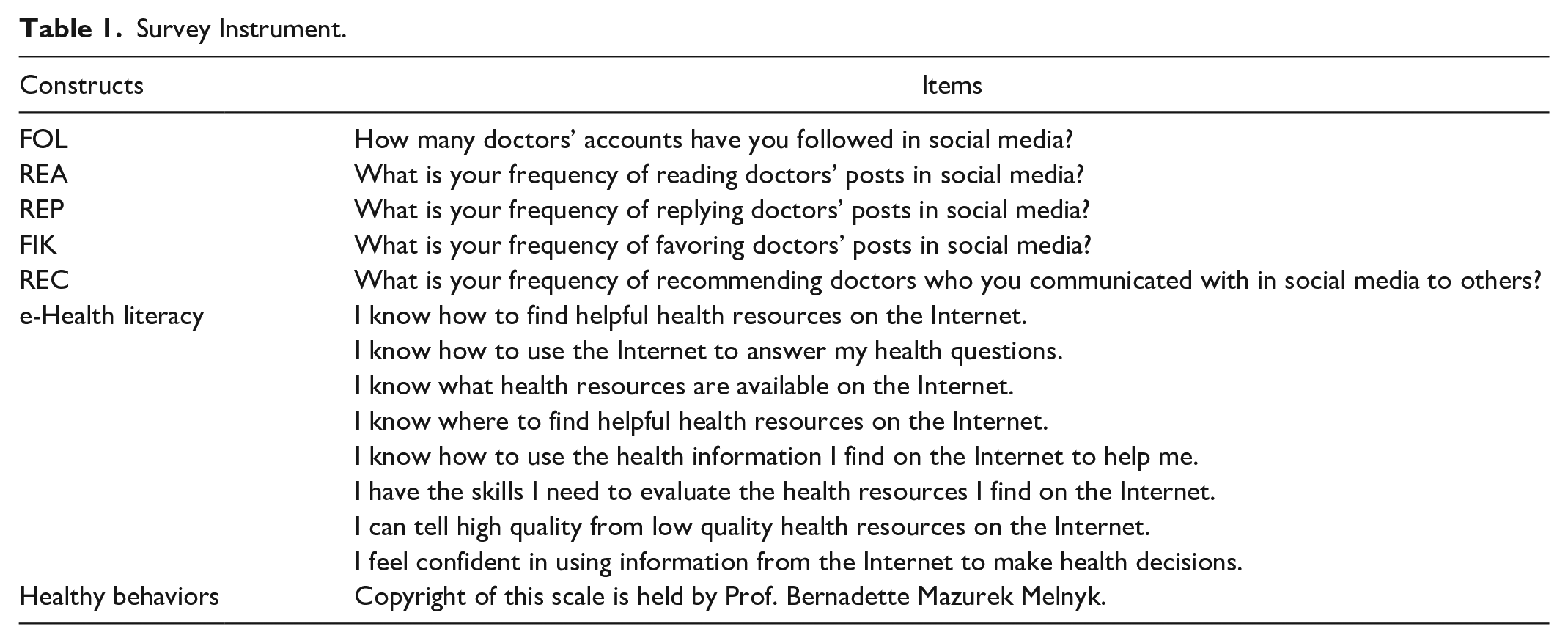
To answer our research question, an online survey was used in this study since social media are internet-based applications. 9 Toward the 5 communication activities, FOL is a user’s action that subscribes doctors’ content from their social media account; REA is a user’s action that views doctors’ content presented on social media; REP is a user’s action that replies or comments on doctors’ content on social media; FIK is a user’s action that expresses users’ favor attitude toward doctors’ content; and REC is a user’s action that suggests or forwards doctors’ content or accounts to their social media friends. Measurement instruments of the 5 communication activities, which are mentioned in introduction section, e-Health literacy and healthy behaviors, were investigated by using online questionnaires. The popular social media in China were mentioned in the questionnaire for participants’ consideration including: Weibo, Wechat, QQ Zone, Youku, etc. 26 A 5-point Likert scale was used to measure all the communication activities. All questions were measured on a 5-point Likert scale with anchors from “strongly disagree” to “strongly agree.” Therefore, the value range of variables were from 1 to 5. The questionnaire with a total of 31 questions that contained screening and demographic questions were sent to respondents. The specific details of measurement instruments are listed in Table 1. Meanwhile, we also list the content of online questionnaire in the Supplemental Appendix A.
Survey Instrument.
The development of research questions was based on the trend of social media usage of patients and public, while outcomes were mainly adapted from previous validated instruments. Interviews of social media users were conducted in the inception phase of this study. Consumers, including patients and non-patients were recruited to fill the questionnaires sent by an online survey platform. The results of this study will be made public in major public online platforms or sent by emails to disseminate it to participants.
Since the measurements of e-health literacy and healthy behaviors were developed in English originally, TW whose native language was Chinese translated them into Chinese at first. Then, ZH translated the Chinese version into English back. The inconsistency between the 2 English versions were solved by discussion between the 2 authors. 27 To ensure the quality of measurement instrument, we invited 9 experts in the area of medical informatics, and health management as well as 17 users of social media to fill the questionnaire and revised the questionnaire based on the comments and suggestions received from them. To distribute our online questionnaires and recruit respondents efficiently, the online panel service from a Chinese market research company was utilized. 28 This company established a pool of respondents who had communicated with doctors on social media and using simple random sampling method to collect our data.
Data Collection Procedures
Recruiting participants via online panel service allowed for efficient distribution of online questionnaires and recruiting participants who complete surveys for a reasonable compensation. Since we employed the Chinese market research company to collect the data, we did not have the identifying information of participants. Besides, several screening criteria were set to ensure data quality and reduce social desirability bias. The screening criteria included whether participants filled attention-trap and reverse coding questions correctly, whether participants had done the 5 identified communication activities with doctors in social media, and whether participants had fully completed the questionnaires, etc. 28
Through 3 weeks of survey in September 2018, 486 respondents were contacted, and 384 complete responses were collected. Therefore, the response rate is 79%. After cleaning the data by using screening criteria to check the answers of questionnaires, we were left with 352 valid responses.
Reliability and Validity
Given we use multi-items to measure e-Health literacy and healthy behaviors, we analyzed the reliability and validity of the 2 constructs. Cronbach’s alpha was computed to estimate the reliability of e-Health literacy and healthy behaviors. We found Cronbach’s alpha of e-Health literacy and healthy behaviors were 0.831 and 0.842, respectively, which were both above the recommended threshold 0.7. 29 Therefore, the reliability for these 2 variables’ scales was demonstrated. Toward the convergent validity of scales of e-Health literacy and healthy behaviors, we considered the relationship between these 2 variables by using Spearman’s rho correlation coefficients. We found e-Health literacy was significant correlated with healthy behaviors (Spearman’s rho = 0.468, P < .001). Therefore, the convergent validity of scales of e-Health literacy and healthy behaviors was also demonstrated. 29
Statistical Analysis
Descriptive analysis was first performed by stratifying the sample by age, gender, education, intensity and experience of using social media. Reliability and validity of e-Health literacy and healthy behaviors were then analyzed by using PASW 22.0. Regression analyses were conducted to estimate communication activities between doctors and consumers associated with e-health literacy and healthy behaviors. To assess the predictive power of communication activities between doctors and consumers, by using hierarchical regression analysis, we used 2 models for both dependent variables. Models 1 and 3 only contain demographic factors including age, gender, education, intensity and experience of using social media, while models 2 and 4 considered both the effect of demographic and 5 communication activities on 2 dependent variables. The formula regression models are presented from equation 1 to 4 as follows:
Model 1:
Mode1 2:

Model 3:

Model 4:
From model 1 to model 4,
Results
Sample Characteristics
According to Table 2, most of the respondents were in the age group of 19 to 29, women, possessing high school degree, and familiar with social media. The demographic information of our sample is reasonable consistent with the national survey of Chinese internet users. 30 Therefore, our sample could reflect the population to some degree.
Demographic and Variable Statistics.

FOL = follow doctors’ social network accounts; REA = read doctors’ posts; REP = respond to doctors’ posts; FIK = favor doctors’ posts; REC = recommend doctors to others; SD = standard deviation.
Communication Activities, E-Health Literacy, and Healthy Behaviors
According to the analysis results, toward e-Health literacy, age (<25, r = −0.178, P < .05) was found to be associated with e-Health literacy significantly, while FOL (r = 0.127, P < .001), REP (r = 0.141, P < .001), and REC (r = 0.133, P < .001) were also associated with e-Health literacy significantly. Thus, following doctors’ accounts, responding to doctors’ posts, and recommending doctors to others could facilitate the improvement of e-Health literacy. With regard to healthy behaviors, age (<25, r = −0.144, P < .05) was also found to be associated with healthy behaviors, FOL (r = 0.091, P < .001), REP (r = 0.072, P < .01), FIK (r = 0.129, P < .001), and REC (r = 0.220, P < .001) were found to be associated with healthy behaviors. Therefore, following doctors’ accounts, responding to doctors’ posts, favoring doctors’ posts, and recommending doctors to others could improve e-Health literacy. The regression analysis results are presented in Table 3.
Regression Analysis of e-Health Literacy and Healthy Behaviors.
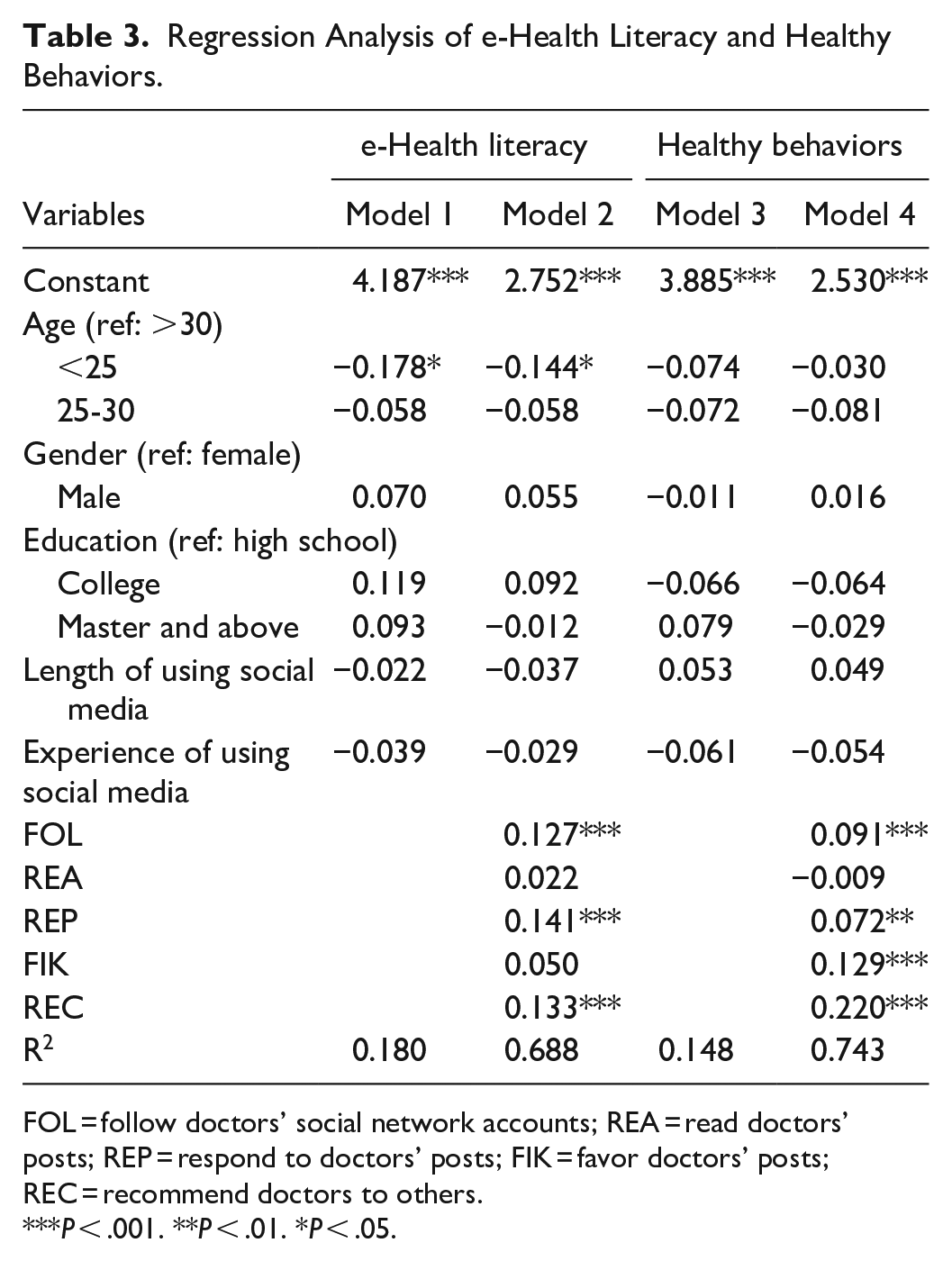
FOL = follow doctors’ social network accounts; REA = read doctors’ posts; REP = respond to doctors’ posts; FIK = favor doctors’ posts; REC = recommend doctors to others.
P < .001. **P < .01. *P < .05.
Discussions
In this study, FOL, REP and REC were found to be significantly correlated with e-health literacy. Through FOL, doctors’ social network accounts could be the source of health information, which could increase the health knowledge which consumers need. The increased health knowledge facilitated the improvement of e-health literacy. For REP, consumers should understand the content created by doctors on social media before they respond. The process of understanding could increase consumers’ health knowledge which contributes to their e-health literacy. Toward REC, consumers need to know the doctors well and learn much health-related knowledge on social media. Therefore, the process of learning would enhance consumers’ e-health literacy.
Meanwhile, this study also reveals that FOL, REP, FIK, and REC were significantly correlated with healthy behaviors. For FOL, the number of following doctors’ accounts could be the signal of consumers’ health awareness and beliefs. Their awareness and beliefs could contribute to healthy behaviors. Regarding REP, responding to doctors’ social media posts may reflect consumers’ engagement in understanding the health content in the posts. The involvement may lead to consumers’ better understanding of the health knowledge in the posts well. Considering FIK, this action may reflect consumers’ positive attitude toward the posts and may follow the suggestions in the posts. Thus, it may affect consumers’ healthy behaviors by changing their intention of conducting the behaviors. 31 At last, toward REC, recommending doctors to others is a specific form of word of mouth which could be the results of satisfaction of doctors’ posts content or trusting doctors they have communicated with. 32 The satisfaction and trust may promote consumers’ healthy behaviors.
However, this study also failed to observe a significant association between REA and either e-Health literacy or healthy behaviors. The possible reason for the insignificant association between REA and the 2 dependent variables is that reading doctors’ posts is a passive use of social media that reflects low involvement in communicating with doctors on social media. 10 Therefore, just reading doctors’ posts may not influence consumers’ e-Health literacy or healthy behaviors. Meanwhile, FIK is shown not to associate e-Health literacy. The possible reason is that favoring posts does not help consumers develop their ability to understand health information directly. 33 Consumers may favor doctors’ posts without reading the content if they identify the doctors.
This study has several contributions to the understanding of physician-consumer communication. On the one hand, we contribute to doctor-consumer communication literature by studying communication between doctors and consumers in the social media context. As far as we know, this is the first study considering the effectiveness of specific doctor-consumer communication activities on social media. Consistent with previous literature, our study shows that communication between doctors and consumers in social media context also could promote consumers’ health outcomes like eHealth literacy and healthy behaviors. Meanwhile, we identified 5 types of activities to reflect communication between doctors and consumers, and evaluated their effects separately. At last, we revealed the impacts of different communication activities on consumers’ e-Health literacy and healthy behaviors through a cross-sectional survey method. On the other hand, the 5 recognized activities could be the novel channels for health policy makers and doctors to promote consumers’ e-Health literacy and healthy behaviors, especially for FOL, REP, FIK and REC. For example, health policy makers could encourage consumers to subscribe more doctors’ accounts in social media and responding to more doctors’ posts. Meanwhile, the favoring and recommending behaviors could be the signals of consumers’ high involvement in communicating with doctors, thus increasing their e-Health literacy and healthy behaviors.
This study has some limitations. First, since the values of correlation coefficients between independent and dependent variables were not high, we also could consider other social media communication activities and relevant variables beside communication activities. Second, we only considered 2 health outcomes including e-Health literacy and healthy behaviors. More health outcomes, especially chronic diseases outcomes may be discussed. Third, the mechanisms of communication activities between doctors and consumers were not studied in this paper. It would be useful to examine the mechanisms for developing effective interventions. Fourth, the generalizability may be constrained since we only surveyed a group of Chinese consumers. To better generalize the study results, future research may involve consumers from other countries. Fifth, we only studied the frequencies of communication activities between doctors and consumers on social media, not the specific content of communication. The communication content could be important drivers for both doctors and consumers’ behaviors. 34 At last, since our study targets were mainly the social media users who communicated with doctors on social media, they may only cover a few people with multi-morbidity.
Conclusion
With their wide use, social media could be a new channel to improve health outcomes. Our study demonstrates that the consumers’ communication with doctors on social media could be effective to promote consumers’ health outcomes. To be specific, following doctors’ posts, responding to doctors’ posts, favoring doctors’ posts and recommending doctors to others are found to be associated with consumers’ health outcomes including e-Health literacy and healthy behaviors. The analysis results suggest that leveraging information technology to promote health outcomes may be an important tool for health policy makers and health providers.
Supplemental Material
sj-pdf-1-inq-10.1177_0046958020971188 – Supplemental material for Impact of Communicating With Doctors Via Social Media on Consumers’ E-Health Literacy and Healthy Behaviors in China
Supplemental material, sj-pdf-1-inq-10.1177_0046958020971188 for Impact of Communicating With Doctors Via Social Media on Consumers’ E-Health Literacy and Healthy Behaviors in China by Tailai Wu, Zhifei He and Donglan Zhang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We sincerely thank the anonymous reviewers for their helpful and illuminating suggestions, but we take the full responsibility for this article. We would also like to thank all participants at the study sites for their cooperation.
Authors’ Contributions
ZFH and TLW contributed to the conception and design of the study. TLW, DLZ, ZFH performed data analysis. DLZ contributed to the final review. All authors critically revised the final version of the manuscript and gave approval for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (71801100), the Fundamental Research Funds for the Central Universities (No. 2018KFYYXJJ063 and 2019kfyXJJS172), Chongqing Social Science Planning Project (No. 2019QNGL33) and 2019 Southwest University of Political Science and Law Project (No. 2019XZQN-30). We highly appreciate the support of School of Medicine and Health Management, Tongji Medical College, Huazhong University of Science and Technology; Southwest University of Political Science & Law, and University of Georgia.
Ethical Approval
All the procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The institutional review board of Tongji Medical College, Huazhong University of Science and Technology has approved our study procedures (No. 2017S319).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.