
Abstract
Background
This study aims to assess healthy lifestyle behaviors among undergraduate students and determine the association between electronic health literacy with lifestyle behavior among undergraduate Jordanian university students.
Methods
A descriptive cross-sectional design was used. The study recruited 404 participants utilizing undergraduate students from public and private universities. The e-Health literacy scale was used to assess the level of health information literacy among university students.
Results
Data were collected from 404 participants who reported very good health status, the majority of the participants were female 57.2% with an average age of 19.3 years. The results showed that participants had good health behavior in terms of exercise, taking breakfast, smoking status, and sleeping status. The results have shown an inadequate level of e-Health literacy 16.61 (SD = 4.10) out of 40. The vast majority of students, in terms of their attitudes toward the Internet, thought that Internet health information was very useful/useful (95.8%). Also, they thought that online health information was very important /important (97.3%). The results showed that students who were attending public universities had higher e-Health literacy scores rather than those who were attending private universities, t (402) = 1.81, p = .014. The mean e-Health literacy score for nonmedical students was higher than those for medical students (p = .022).
Conclusion
The study's findings provide important insights into the health behaviors and electronic health literacy of undergraduate students in Jordanian universities, and offer valuable guidance for future health education programs and policies aimed at promoting healthy lifestyles in this population.
Background
Healthy lifestyle behaviors are considered important means to reduce the burden of diseases as well as bring the person's general health to the highest level of well-being and self-efficacy.1–3 University life is a critical period among students since they take on new responsibilities and decision-making roles when they arise away from their homes and families. 4 Many studies proved that healthy lifestyle behaviors had a significant impact on undergraduate student's life, and they are prone to share risky behaviors resulting in a significant impairment in health status.5,6 So, individuals should take responsibility to protect themselves from diseases by following healthy lifestyle behaviors.
Health literacy (e-Health literacy) is known as the ability of an individual to read, write, and understand the information related to health and to choose the appropriate decisions. 7 e-Health literacy is defined as “reading, understanding, and applying the information that individuals receive about their health.” 8 e-Health literacy is noted as the ability to appraise health information using different electronic sources and apply the knowledge acquired to address or solve a health problem. 9
Utilizing e-Health literacy among university students is an essential factor to maintain healthy behavior and quality of life. 10 Studies show that health literacy skills increase the health knowledge of university students, and the development of positive health behaviors. A cross-sectional study was conducted among 152 nursing students, the results showed that (65.1%) of students mentioned e-Health literacy usefulness in helping to make health decisions. 11 In another study, the results showed that more than a quarter of students improved their “Actively managing my health,” “Social support for health,” after using e-Health literacy. 12
e-Health literacy is considered one of the six components such as analytical skills (media, traditional and numeracy, and information literacies) and context-specific skills (science, computer, and health literacies). 13 Generally, many social and behavioral variables are associated with health literacy levels among university students such as age, gender, educational level, income, and medical background.14,15 It was found that male students, with higher educational levels, higher incomes, and high academic achievements were strongly associated with high levels of health literacy.10,16 However, health responsibility, physical activity, spiritual development, nutritional habits, and stress management were the main constituents of healthy lifestyle behaviors that were shaped during the university life period. Hence, this study is conducted to assess the healthy lifestyle behaviors among undergraduate students and determine the association between e-Health literacy and lifestyle behavior among undergraduate Jordanian university students.
Materials and methods
Study design
A descriptive cross-sectional study was conducted involving undergraduate students from different faculties.
Sample and setting
The study was conducted in different governmental and private universities which included different faculties including medical and nonmedical schools in northern Jordan. G* Power software was used to calculate the sample size. Based on an estimated effect size of (d) = 0.7, ά = 0.05, power = 0.95, the required sample size was estimated at 370 to run a paired sample t-test. In literature reviews, as a general rule, a sample size of 300–400 is considered sufficient for this type of study.17,18 The inclusion criteria included (1) undergraduate university students from the first to the sixth year of study and (2) agree to participate in the study.
Data were collected by sending the questionnaire link to different WhatsApp groups between January and February 2023. Also, the link was distributed among different student clubs and forums via Facebook groups. Each willing participant fills out the link and sends it. There were 404 surveys completed in total. However, incomplete responses were excluded from the final study.
Instruments
A self-administrated questionnaire contains three parts including (1) demographical data of age, sex, year of study, faculty type, living situation, general health, and Internet use; (2) lifestyle behaviors asking about exercise, breakfast, smoking, hours of sleep, and smoking status, and (3) e-Health literacy that includes eight questions measures a variety of e-Health literacy skills. 19
In accordance with previous studies each health behavior was divided into one of two categories (good health behavior; poor health behavior).20,21 For the lifestyle behaviors, answers to exercises were (1–2 days/week, ≥ 3 days/week, 1–2 days /month, and never). 19 The highest frequency of categories (1–2 days/week, ≥ 3 days/week) was considered good health behavior while the highest frequency of categories (1–2 days /month, and never) was considered poor health behavior.
Answers about breakfast were categorized as (every day, 5–6 days/week, 1–4 days/week, and never). 20 The highest frequency of categories (every day, 5–6 days/week) was considered good health behavior while the highest frequency of categories (1–4 days/week and never) was considered poor health behavior.
Answers about smoking have assessed the answers of nonsmokers, previous smokers, and current smokers. 21 The highest frequency of the category of nonsmokers considered good health behavior.
Answers about sleeping hours were organized as (≥ 9 hours, 7–8 hours, and < 6 hours). 20 The highest frequency of categories (≥ 9 hours, 7–8 hours) was considered good health behavior while the highest frequency of categories (< 6 hours) was considered poor health behavior.
The body mass index (BMI) was defined as < 18 underweight, 18.1–25 normal, and > 25 overweight. 20
The e-Health literacy is composed of four questions about Internet capability and four questions about using health information.16,21 A 5-point scoring system was used to generate answer options “1 = strongly agree so to 5 = strongly disagree (5)” for each item. The sum score is used to rate e-Health literacy as inadequate, 8–20: problematic, 21–26: or sufficient, 27–40). 22 The e-Health literacy skills have showed adequate reliability and validity in both the English and Arabic versions of the scale with high reliability, Cronbach’s α=0.93.16,22 Also, it was used among medical students which shows reliable and valid measures of eHEALS. 23 In another test of the reliability and validity of eHEALS in Poland using the telephone-based and online among two representative samples, Cronbach's α were 90.0 and 88.0. 24 Besides, the questionnaire was tested for validity and reliability in previous studies and was found valid and reliable.2,25 The reliability coefficient (Cronbach's α) for this study was 0.83, this indicates that the instrument has acceptable internal consistency. The higher score indicates higher health literacy skills and vice-versa.
Ethical considerations
The study protocols were reviewed and approved by the ethics committees at Al al-Bayt University (1 January 2023). A student who was willing to complete the survey implied informed consent. Privacy and confidentiality of subjects were maintained. Participants had the freedom to skip questions or stop answering at any time.
Data analysis
Data were analyzed using the Statistical Package for the Social Sciences, Version 20 for Windows. Frequencies and descriptions of all variables were examined to assess the accuracy of data entry and missing values. Descriptive statistics of frequency, mean, standard deviation, and percentages were used to express participants’ demographical data, lifestyle behaviors, and the level of e-Health Literacy skills. While inferential statistics such as t-test was used to assess the differences between groups and the total scores of e-Health literacy skills. The correlation was also utilized to assess the association between participants’ characteristics, lifestyle behavior, and total e-Health literacy skills.
Results
Participant's demographic
A total of 404 undergraduate students participated in this study. The average age of the students was 19.34 (SD = 1.25) years, and more than half of them (n = 231, 57.2%) were women. The majority of participants (n = 135, 33.4%) were in their first year of study, with 50.2% of them studying medical specialties and 49.8% nonmedical specialties. An average of 93.8% of participants utilized the Internet every day. The vast majority of students, in terms of their attitudes toward the Internet, thought that Internet health information was very useful/useful (95.8%). Also, they thought that online health information was very important /important (97.3%) (Table 1).
Demographic characteristics and interest usage (N = 404).

Concerning the lifestyle behaviors that were followed among undergraduate university students, the results revealed that more than half of participants n = 226 (55.9%), had good health behavior in terms of exercise. Regarding taking breakfast n = 231 (57.2%) had good health behavior that they take their breakfast every day or 5–6 days/week. Regarding the smoking status, two-third of participants n = 289 (71.5%), reported that they were nonsmoker. Although more than half of the participants were classified as normal weight (56.7%), however, about 33.9% were considered overweight. The majority of participants n = 326 (80.7%), had good health behavior in terms of sleeping status. Self-reported health status for the majority of participants was very good (53%) or good (37.6%) (Table 2).
Lifestyle behaviors of the participants (N = 404).

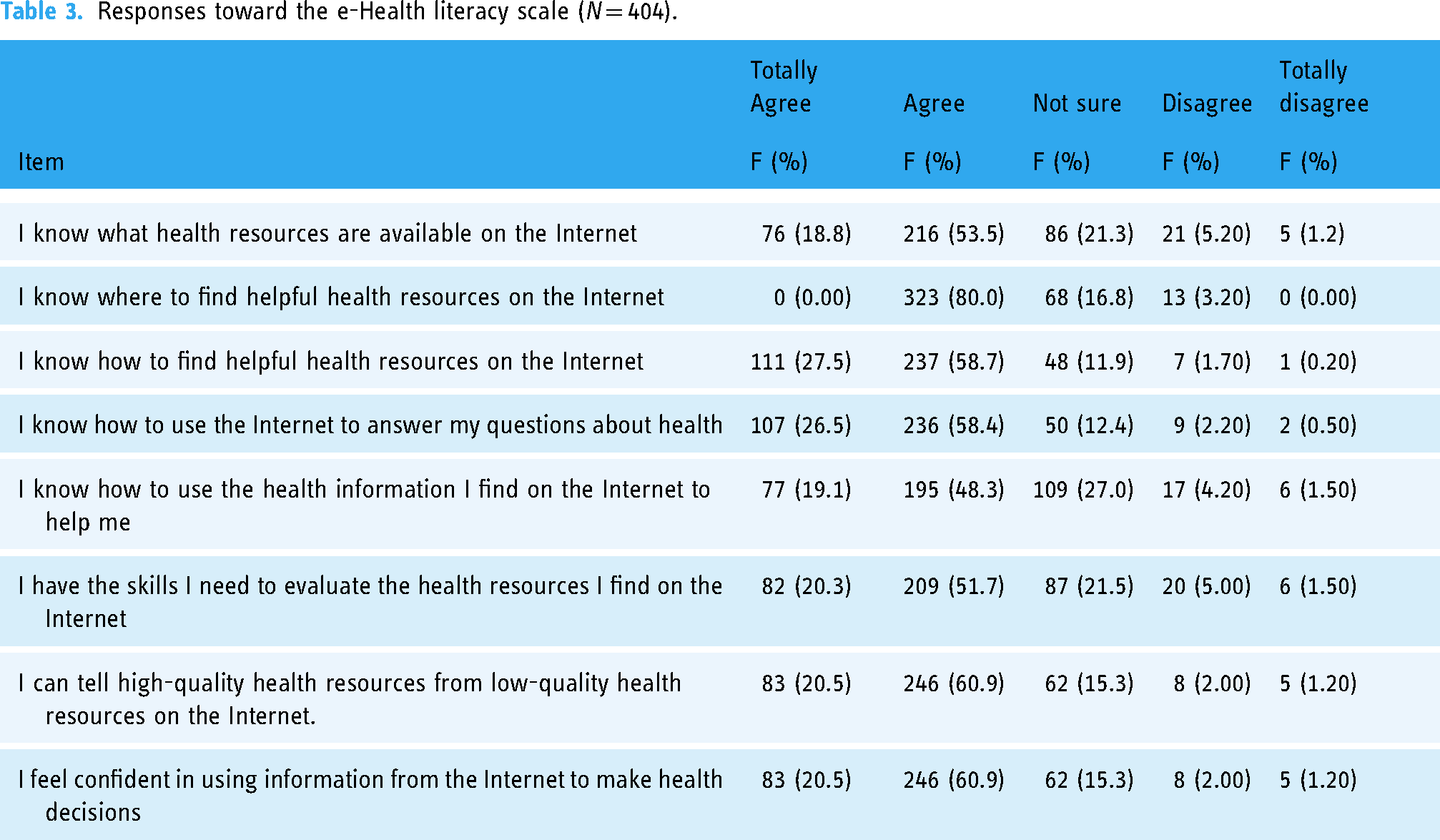
The e-Health literacy level among university students, the results have shown that the mean score of e-Health literacy was 16.61 (SD = 4.10) out of 40, ranging from 9 to 37. The e-Health literacy subscale's results showed that each item's mean scores ranged from 1.89 to 2.23. The participants mostly agree with their knowledge about the health resources which were available on the Internet (n = 216, 53.5%). Most of the students verified the agreement of their knowledge of where and how to locate helpful health resources on the Internet (n = 323, 80%) and (n = 237, 58.7), respectively. Around half of the students (n = 195, 48.5%) and (n = 209, 51.7%), respectively, reported that they agreed with their knowledge and skills to evaluate the health resources that they found (Table 3).
Responses toward the e-Health literacy scale (N = 404).
An independent t-test was used to assess the mean difference between the total score of e-Health and the demographics of sex, university type, and specialty. Generally, the items of type of university, specialty, and study years were significantly associated with e-Health literacy based on participant characteristics. In addition, the results showed that students who were attending public universities had higher e-Health literacy scores rather than those who were attending private universities, t (402) = 1.81, p = .014. The mean e-Health literacy score for nonmedical students was higher than those for medical students (p = .022). There were, however, no significant differences between the sex of the students, t (402) = −0.034, p = .973, and the living status among university students, t (402) = 0.462, p = .709 (Table 4).
One-way ANOVA between groups was conducted to explore the impact of years of study and living status on the e-Health literacy total scores. The result revealed that e-Health literacy scores differed significantly across the groups, F (5) = 2.73, p = .019. The Turkey HSD test post hoc comparison revealed a significant difference between the fifth-year students’ mean score (M = 23.3, SD = 7.23) and the other study years. While for living status the result demonstrated that there were no statistically significant differences among the participants, F (4, 404) = 0.462, p = .709 (Table 5).
one-way ANOVA test was utilized to find the mean differences between the participants’ lifestyle behaviors and their total e-Health literacy score. For doing the exercises, it statistically differed across the groups, F (5) = 8.512, p < .000, among the students who do exercise 1–2 days/month (M = 17.41, SD = 4.43). Having the breakfast meal and smoking status, and sleeping hours were not statistically significant factors with the total score of e-Health literacy score, F (2) = 1.182, p = .361, F (2404) = 0.946, p = .389, F (2404) = 1.86, p = .157, respectively (Table 6).
Difference between groups related to e-Health.

Association of e-Health literacy scores with demographical characteristics (N = 404).

Association of e-Health literacy scores with lifestyle behaviors (N = 404).

Multiple regression analysis using a stepwise method showed that the predictor variables were able to explain 7.5% of the variance in e-Health literacy scores among students, with an R-squared value of 0.075. The F-value was 7.753, with an associated p-value of .066, indicating that the overall model was statistically significant, but the effect size was small. Among the predictor variables, never exercising had the largest positive effect on e-Health literacy scores, with a regression coefficient of 1.730 (SE B = 0.406, β = 0.216, p = .001). Exercising 1–2 days per month and consuming breakfast 1–4 days per week also had positive effects, with regression coefficients of 1.712 (SE B = 0.751, β = 0.115, p = .023) and 0.945 (SE B = 0.419, β = 0.111, p = .025), respectively. Being in a nonmedical specialty was also positively associated with e-Health literacy scores, with a regression coefficient of 0.787 (SE B = 0.383, β = 0.102, p = .041) (Table 7).
Multiple regression of predictors of score of e-Health literacy skills among students.
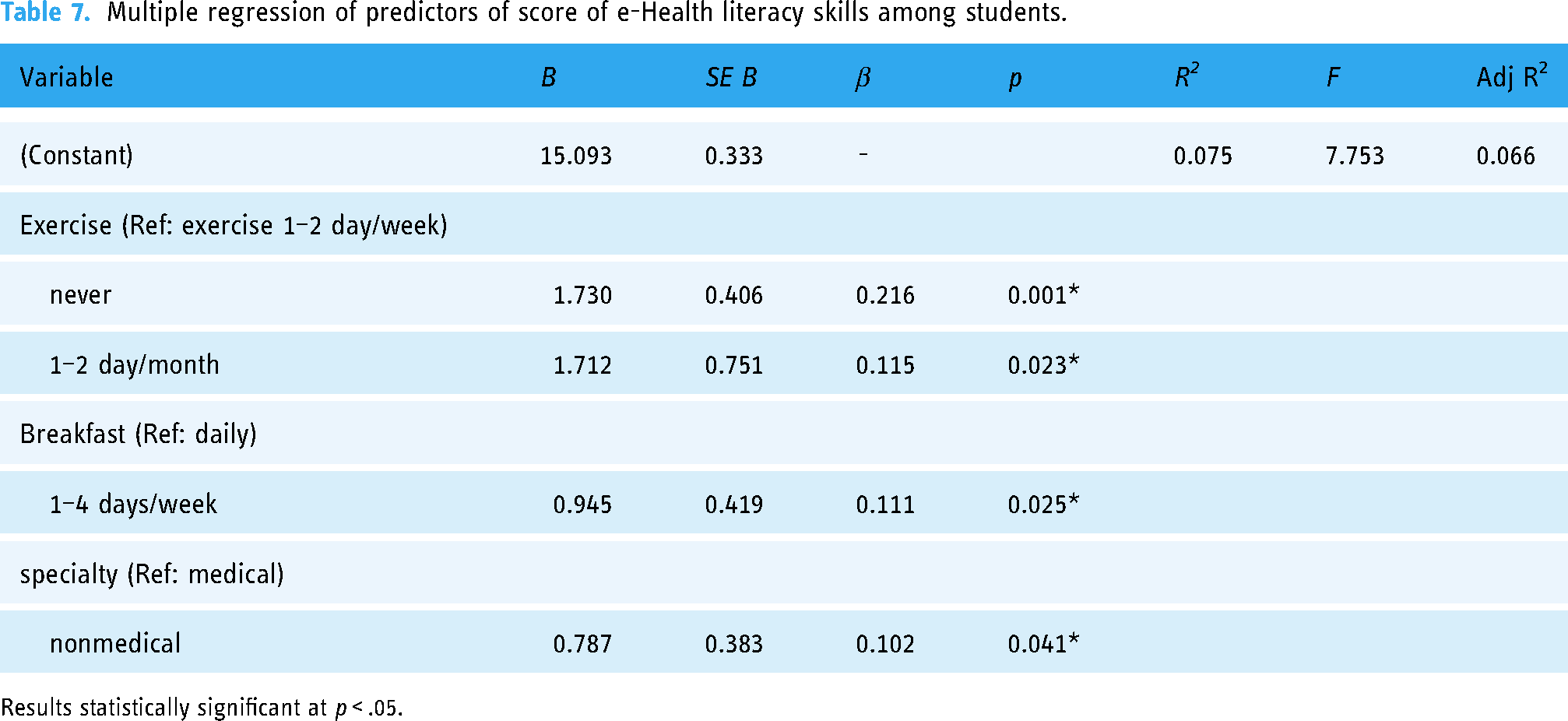
Results statistically significant at p < .05.
Discussion
The purpose of this study was to assess the behaviors related to a healthy lifestyle among undergraduate students and determine the correlation between electronic health literacy and lifestyle behaviors among Jordanian university students. The findings of this investigation reveal that the vast majority of students use the Internet daily and view online health information as practical and valuable. These results were consistent with previous research that has highlighted the Internet's significance as a primary source of health information, particularly for younger generations. 26 The high usage rate of the Internet among students can be attributed to the fact that it offers easy and convenient access to a plethora of health-related information. This is especially important for individuals who may not have easy access to traditional healthcare services or who may be searching for additional information to supplement their healthcare provider's advice. 27 The discovery that most students find online health information to be useful and important is also noteworthy. This suggests that students place a considerable amount of trust in online health information and believe that it can provide them with valuable insights into their health and well-being. However, it is important to recognize that not all online health information is equal, and users should be encouraged to assess the information they find online critically. 28
The finding that only half of the students were taking breakfast daily is also notable. Breakfast is often referred to as the most important meal of the day, and skipping breakfast has been associated with negative health outcomes, including weight gain and poor metabolic health. 29 On a positive note, the majority of students were nonsmokers, which is consistent with the declining trend of smoking prevalence among young adults. 30 In addition, more than half of the students had a normal BMI and reported getting enough sleep, which are important indicators of good health.
The results of this study suggest that the lifestyle behaviors of the majority of students are good health behavior in terms of exercise and sleep. The finding that less than half of students were not engaging in regular exercise is concerning given the well-established benefits of physical activity for both physical and mental health. 31 This is consistent with previous research that has shown that sedentary behavior is common among young adults and that it is associated with a range of negative health outcomes.32–34
Regarding electronic health literacy, the study found that the mean score was at an inadequate level. This is in line with previous research that has identified low levels of health literacy as a common problem, especially in relation to electronic health information.35,36 Interestingly, the study revealed that electronic health literacy was higher among students in public universities compared to those in private universities. The reason for this disparity may be attributed to a variety of factors such as variations in access to resources and support for health education and promotion initiatives. Additionally, students in public universities may have greater opportunities to engage with electronic health information, which could contribute to their higher levels of electronic health literacy.
The result indicating that students in nonmedical colleges have higher electronic health literacy than students in medical colleges is surprising. One possibility is that nonmedical students have a stronger drive to find and use electronic health information, given that they may have less exposure to health-related content in their academic studies. Alternatively, medical students may rely more on traditional health information sources such as textbooks and lectures, rather than electronic sources. The study found that students in the fifth year had higher electronic health literacy compared to those in the fourth and sixth years, which is consistent with previous research showing that health literacy improves with age and education level.37–39 This improvement could be attributed to increased exposure to health information and familiarity with electronic health resources. 40
The finding that students who never exercise have higher electronic health literacy than those who exercise ≤ 3 times per week is intriguing and may reflect the allocation of time and attention toward different areas of health. A study reported that e-Health literacy was not linked to health behaviors such as physical activity and dietary supplement intake in young adults. 39 One possible explanation for this finding is that those who never performed exercise may have more time and energy to devote to learning about health topics, including electronic health literacy. Additionally, individuals who engage in regular physical activity may have less time to devote to other health-related activities, including electronic health literacy, due to the time demands of exercise.41,42
The study has limitations that should be considered when interpreting its results. Firstly, the study relied on self-reported data, which may not accurately reflect the participants’ actual behavior and can be influenced by measurement errors and biases. Secondly, the study did not control for other variables that could affect the relationship between electronic health literacy and lifestyle behavior, such as socioeconomic status or cultural norms. Thirdly, the study used a cross-sectional design, which limits the ability to establish a cause-and-effect relationship. A longitudinal design would provide more robust evidence. Lastly, the study measured only a few aspects of lifestyle behavior, which may not capture the complexity and diversity of the participants’ overall lifestyle, leading to incomplete conclusions.
Conclusions
The study aimed to evaluate healthy lifestyle behaviors among undergraduate students and investigate the association between electronic health literacy and lifestyle behavior in Jordanian universities. The study found that the majority of students in the participants used the Internet daily and had a positive attitude toward online health information. The results showed that participants had good health behavior in terms of exercise, taking breakfast, smoking status, and sleeping status.
The study discovered that the average score for electronic health literacy was inadequate, with students in governmental universities having higher levels of electronic health literacy than those in private universities. In addition, students in nonmedical colleges scored higher than those in medical colleges. It was also noted that students in their fifth year of study had better electronic health literacy than those in the fourth and sixth years. However, it was surprising to find that students who did not exercise had better electronic health literacy than those who exercised three or fewer times per week. These results offer valuable information on the lifestyle behavior and electronic health literacy of undergraduate students in Jordanian universities, which could help design health education programs. Nevertheless, the study's findings should be taken with caution due to its limitations.
Implications and recommendations for practice or policy
The study's results have several implications and recommendations for practice or policy. Firstly, it suggests that promoting healthy lifestyle behaviors among undergraduate students in Jordanian universities is necessary. Interventions could be implemented to encourage regular physical activity since a significant proportion of students reported never or only occasionally engaging in physical exercise. Additionally, promoting healthy sleep habits and increasing the proportion of students who have breakfast daily could be useful. Secondly, the study highlights the importance of electronic health literacy in promoting healthy behaviors. Incorporating e-Health interventions into health education programs, such as providing access to reliable online health information, developing mobile health applications, and using social media platforms for health promotion, may be helpful. Thirdly, the study reveals differences in electronic health literacy levels between students in different types of universities and colleges. Targeted interventions and resources could be developed to address the gap in electronic health literacy between students in private universities and those in governmental universities, as well as between medical and nonmedical college students, tailored to the specific needs and preferences of different groups of students. Overall, the study's findings provide important insights into the health behaviors and electronic health literacy of undergraduate students in Jordanian universities and offer valuable guidance for future health education programs and policies aimed at promoting healthy lifestyles in this population.
Footnotes
Acknowledgments
The authors extend their appreciation to Princess Nourah bint Abdulrahman University Researchers Supporting Project number PNURSP2023R279, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Guarantor
The research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number PNURSP2023R279, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Contributorship
conceptualization: Shudayfat T; methodology: Shudayfat T and Bani Hani S; investigation and project administration: Bani Hani S and Shdaifat E; validation and supervision: Bani Hani, Shdaifat E, and Shudayfat T; data curation and funding: Al-Mugheed K; resource: Sally MF Abdelaliem and Al-Mugheed K; formal analysis: Alsenany SA and Al-Mugheed K, and Sally MF.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R279), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.