
Abstract
Introduction
The COVID-19 pandemic had a significant impact on healthcare delivery worldwide. Digital tools emerged as a preferred solution for maintaining healthcare services during this crisis. This study aimed to assess the magnitude of digital health literacy among healthcare professionals in Ethiopia in 2020–2023.
Methods
A systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. Articles published from 2020 to 2023 were reviewed using various electronic databases such as Medline, PubMed, and Cochrane Library, CINAHL, HINARI, Science Direct, Google Scholar, and Global Health. Meta-analysis was performed using STATA 17, and publication bias and heterogeneity were assessed.
Results
Six studies involving a total of 2739 participants were included in the analysis. The pooled level of high digital health literacy among health professionals in Ethiopia during the pandemic was found to be 56.0% (95% CI: 55, 58). Several factors were identified as significant contributors to high digital health literacy, including internet use (AOR = 2.72, 95% CI: 1.86, 3.98), perceived ease of use (AOR = 2.79, 95% CI: 1.83, 4.25), favorable attitude (AOR = 2.49, 95% CI: 1.61, 3.85), perceived usefulness (AOR = 2.29, 95% CI: 1.65, 3.18), information-communication-technology training (AOR = 6.09, 95% CI: 1.83, 24.27), and educational level (AOR = 3.60, 95% CI: 2.96, 4.37).
Conclusion and recommendation
The study findings revealed a moderate level of high digital health literacy among Ethiopian health professionals. Factors such as internet use, favorable attitude, and information-communication-technology training were associated with high-level digital health literacy. To enhance digital health literacy, it is crucial to provide timely training and improve internet access for healthcare professionals. Additionally, promoting the perception of digital tools as useful and supporting evidence-based decision-making can further improve digital health literacy. Comprehensive information-communication-technology training programs should be implemented to equip healthcare professionals with necessary skills to effectively combat outbreaks like the COVID-19 pandemic.
Introduction
The noble corona virus (COVID) is a respiratory virus that causes millions of death across the global environment. 1 The virus was first identified in one of the Chinese city, Wuhan, since December 2019. 2 Due to the nature of the (COVID-19) virus rapid spread around the world, the World Health Organization (WHO), declared it as a pandemic disease. 3 The burden of the corona virus disease has been increased and affected the health system and challenged as a result of huge amount of cases that seek health care services. The corona virus disease (COVID-19) has produced difficulties for both individual, patients, health professionals and the health care system as a whole.
Though lockdowns and quarantine mechanisms have been introduced to reduce the virus expansion from infected individual to non-infected ones, government officials, public authorities and groups of individuals showed a role in tackling it.4–7 Different conducted research results in Africa, indicate that health care systems have been vulnerable due to the pandemics’ challenge in health care staff shortages, personal protective equipment(PPE) shortages, intensive care unit (ICU), and Hospital bed capacity shortages.6,8
To curb, the corona virus diseases transmission that causes more illness in the working area, health professionals were using digital technologies to support clinical consultations, and medical treatments. Due to the pandemic exponential growth, the use of digital health interventions 9 has a paramount role and its advancement has greatly increased by the health care professionals to mitigate the over expansion of the disease.10,11
As to the first case of covid-19 confirmed in Ethiopia since 13 March 2020, a report revealed by World Health Organization and Ethiopian Ministry of Health, and the World Health Oorganization Country Office Ethiopia (WCO) is following up closely to ensure an outbreak in Ethiopia is quickly controlled and contained. The COVID-19 Emergency Operations Centre housed at Ethiopian Public Health Institute (EPHI) is working closely with the Ministry of Health and the WCO to respond to this case and implement firm control measures.
12
In addition, to foster the collaboration between Health Care providers and communities living both in Rural and Urban areas of the globe, technological advancements are in place to solve the most daunting public health challenges. Using different techniques to identify, and apply the right technology in a way that is effective and efficient is today's digital health approach.
The Ministry of Health in Ethiopia has launched digital technologies to digitize the health information system (HIS), and keep running to enable digital health data reporting, for use among health care providers.
Studies suggested that digital health literacy has been associated with better health, positive behavior, such as prevention and management of chronic disease. 13 With the same understanding, digital health literacy has paramount significance for the management of health conditions and improves the service delivery quality.14–16 The corona virus outbreak has forced different sectors, particularly the health sector to use different digital technologies to manage health-related information and increase data use for better decision-making.
Though COVID-19 affected the economic, social and health of the public as an emergent disease, it opens the room for finding solution to seek information related to health, such as use of internet to find up-to-date information, communicate with people who lived at distant and users mentioned that their attitude to use internet enabled devices positively increased during the COVID-19 pandemic.17,18
While contemplating digitization, users should play a role not as a passive recipient of any form of information rather they should actively involve in the communication process by interacting with the information on hand and by sharing their own health-related information. 19 Health professionals endorsed themselves with the latest digital health platforms of information and communication, with regard to playing a pivotal role in finding recent and most up-to-date health data and disseminate it to the user as a means to tackle misinformation about the distribution of the virus.20,21 The knowledge of digital health would promote the participants’ sovereignty by enhancing transparent health information for the active users, and further health professionals’ health information-seeking behavior.21–23 During the corona virus outbreak, health professionals were indebted in search of health information using information technologies to capacitate and share health-related information to the public using different social media platforms. 24
In Ethiopia, even though the digital health literacy level of health professionals was not adequately measured, there was an initiative to use digital platforms which could support the health extension workers to inform them about COVID-19 basic information, vaccine information, treatment and service information, and their home-to home visit, work setting and institutional inspections. 25 The platform was designed by Amharic Language and it was implemented by the ministry of health (MoH), named as “COVID-19 HEW Guide-Amharic”. 26
Studies witnessed that, digital health literacy was associated with computer skills, perceived ease of use, perceived usefulness, internet access, knowledge of digital health, Positive attitude and digital health training.6,7,27,28 Furthermore, digital health literate health professionals are believed to combat patient adverse effects by using information communication technologies (ICTs) and enabling their patients by providing IT support 28 on how to use, access and share streamlined health information that can aid the patients for better treatments.24,29 On the other side, poor digital health literacy among health care professionals would result in adverse patient outcomes; such as poor adherence to medical treatments, poor communication between providers and patients, and a medication errors.6,29–31
Identifying and dealing with these problems, would have a positive impact to design and secure sustainable digital health implementation and advancing the quality of health care service delivery. Additionally, knowing the level of digital Health determinants will help the health care administrators to install and design appropriate digital health tools for tackling emergent diseases like COVID-19. Moreover, the policy makers will be benefited from the result of this systematic review and meta-analysis findings, for wide installations of digital health initiatives which can advance the quality of health service delivery and promote a large-scale adoption by different sectors of the health system. If the government put an effort to capacitate and capitalize on the benefits of digital health, it will be quite demanding to expand the culture of information for better decision-making. With a direct effect, having better decision-making will result in better health outcomes. However, due to a limited number of studies, it has a burden to determine the effect of digital health literacy among health care providers in Ethiopian context. The finding of this study will be a baseline for the upcoming researchers to expand the study with intervention regarding digital health literacy. Therefore, the basic aim of this study was to assess digital health literacy and associated factors through systematic review and meta-analysis during the COVID-19 pandemic in Ethiopia.
Methods
Study design and search strategy
The Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guideline was used rigorously throughout this review. This systematic review and Meta-Analysis were registered in PROSPERO with a protocol number CRD42023461451. A systematic review and meta-analysis of published and unpublished studies were performed to assess the pooled effect of digital health literacy and associated factors in Ethiopia during the outbreak of corona virus pandemic. Electronic databases such as Medline, Pub Med, and Cochrane Library, CINAHL, HINARI, Science Direct, Google Scholar, and Global Health were used. The following key terms and Medical Sub Headings, free text search terms will be used to identify studies: such as “digital health,” “electronic health,” “Covid-19,” “Corona virus,” “factors,” “determinants,” “predictors,” “factors associated,” “associated factors,” “Ethiopia” by a combination of Boolean operators “AND” or “OR” as applicable and the search was made by two authors independently (MDK and SDK).
Inclusion and exclusion criteria
This review included all accessible studies done from January 2020, till October 2023. All published and unpublished studies were used on digital health literacy among health professionals during COVID-19 and associated factors in Ethiopia were incorporated in the review. All observational studies with English language publications that measured the digital health literacy level during COVID-19 outbreak and associated factors among health professionals were included in this review. Unpublished articles, Papers with the absence of full text, conducted out of Ethiopia, did not focus on digital health literacy and qualitative studies were excluded.
Outcome measurement
The level of digital health literacy in this systematic review and meta-analysis was measured using 9 close-ended Likert scale item questions labeled “strongly disagree = 1”, “disagree = 2”, “neutral = 3”, “agree = 4”, “strongly agree = 5”. Since the studies indicated that the responses for each item for measuring digital health literacy was not normally distributed median was used and participants who scored above the median score were classified as high digital health literate and those participants who scored below the median score value were categorized as having low digital health literacy level.14,32–36
Study selection, quality appraisal, and data extraction
All articles explored from selected databases were exported to Endnote 20 and duplicate files have been dropped. Two investigators (MDK and MHK) played a role in screening the leftover articles and abstracts for inclusion in the full-text appraisal. The difference between reviewers was managed through discussion, and disagreement was handled by the third party (NK). The Joanna Briggs’ Institute (JBI) critical appraisal checklist for the prevalence study was used to evaluate the quality of articles that fulfilled the inclusion criteria. Three reviewers (AM, SDK, and MHK) independently assessed the articles prior to inclusion in the review.
Three authors appraised the quality of each independently (AM, SDK, and MHK). The tool mainly included the following information as a criterion. (1) whether the study used an appropriate sampling frame; (2) study participants sampled in an appropriate; (3) indication of an adequate sample size, (4) a detail description of the study subjects and setting, (5) whether the data analysis conducted with sufficient coverage, (6) were the study used valid methods for condition identification, (7) whether the condition measured in a standard, reliable way for all participants or not; (8) whether the study briefing appropriate statistical analysis and (9) indication of an adequate response rate. “Yes,” “Not reported” and “Not appropriate” ratings were given for each item. In the end, the total quality score was assigned based on the number of “Yes” responses as per the study. Articles with a rating of 5 or above out of 9 were included in the final review. 37
Microsoft Excel 2013 sheet was used for data extraction. The information on the author’s name, year of publication, year of study, study design, study area, response rate, sample size, study quality score, proportion, and associated factors contained in the data extraction tool.
Statistical methods and analysis
The analysis was carried out using STATA 17 software. Forest plots diagram used to present the pooled prevalence of digital health literacy among health professionals in Ethiopia. The presence of heterogeneity was assessed by using the I2 statistics, and declared using a p-value of less than 0.05. Subgroup analyses were performed by different study characteristics such as region, study year (before 2020 or 2020 and above). The Egger regression asymmetry test was also used to check publication bias and confirmed with a p-value of less than 0.05. Moreover, Duval and Tweedie's “trim and fill” method was used to estimate the number of missing studies from the meta-analysis.
Results
Study selection
From a total of 256 articles identified from the database search (Medline, Pub Med, and Cochrane Library, CINAHL, HINARI, Science Direct, Google Scholar, and Global Health), we found 103 articles duplicated at the beginning. One hundred fifty-three (153), articles were further screened for eligibility and 85 articles were found excluded due to title and abstract. In addition, 68 articles were reviewed for full-text article and 62 were found excluded due to the absence of full text, conducted outside of the study area (Ethiopia), qualitatively done and did not focus on digital health literacy. Therefore, only six studies were included for the systematic review and meta-analysis (Figure 1).

PRISMA flow diagram of digital health literacy and associated factors among health professionals during the outbreak of COVID-19 pandemic in Ethiopia.
Characteristics of the selected studies
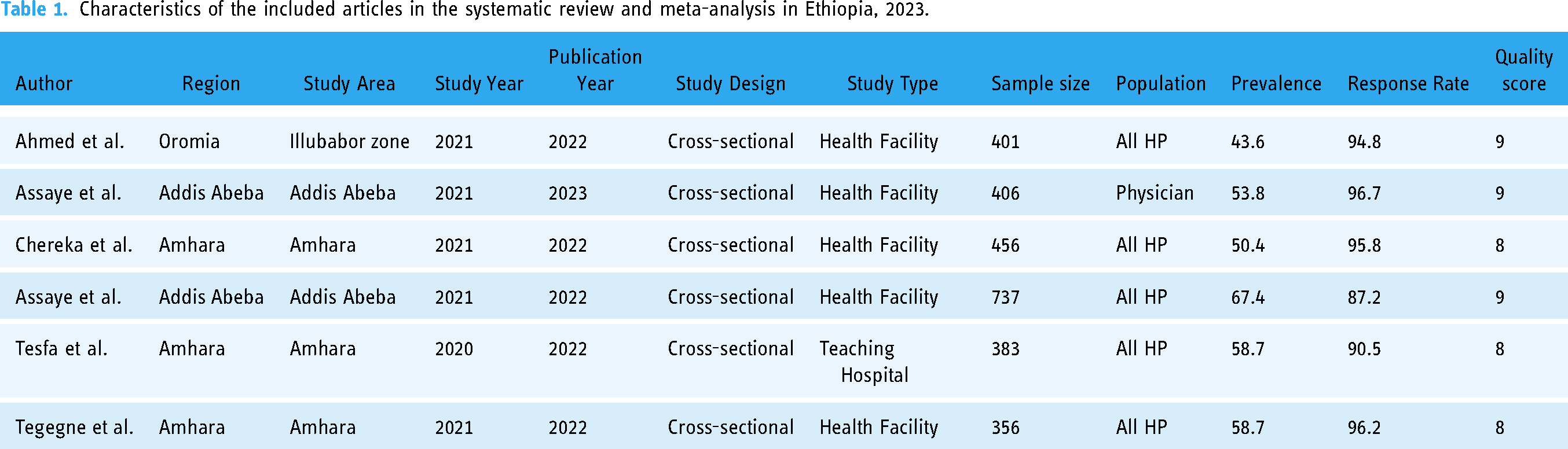
To estimate the pooled prevalence of good digital health literacy among health professionals during the outbreak of covid-19 pandemic in Ethiopia a total of six primary studies with 2739 study participants were included. In this meta-analysis three studies from Amhara region33,35,36 with a total sample size ranging from 356 to 456 were used and two studies conducted from Addis Ababa32,38 and one study done from Oromiya 14 were included. As indicated in the table below all studies were conducted using a cross-sectional type of study design and most of the study14,32,33,35,38 populations were health professionals and one study 32 contained physicians only (Table 1).
Characteristics of the included articles in the systematic review and meta-analysis in Ethiopia, 2023.
Magnitude of digital health literacy in Ethiopia during the corona virus pandemic
The pooled magnitude of high digital health literacy among health professionals during the outbreak of the novel corona virus in Ethiopia was 56% (95% CI: 55,58). This indicates that 56% of the health professionals included in the analysis demonstrated high levels of digital health literacy during the coronavirus outbreak. The result of this systematic analysis showed that there was a significant amount of heterogeneity among the included digital health-related primary studies (overall IV, I2 = 94.2, p = 0.000) (Figure 2).

Forest plot of the pooled prevalence of DHL among health professionals during the outbreak of coronavirus pandemic in Ethiopia, 2023.
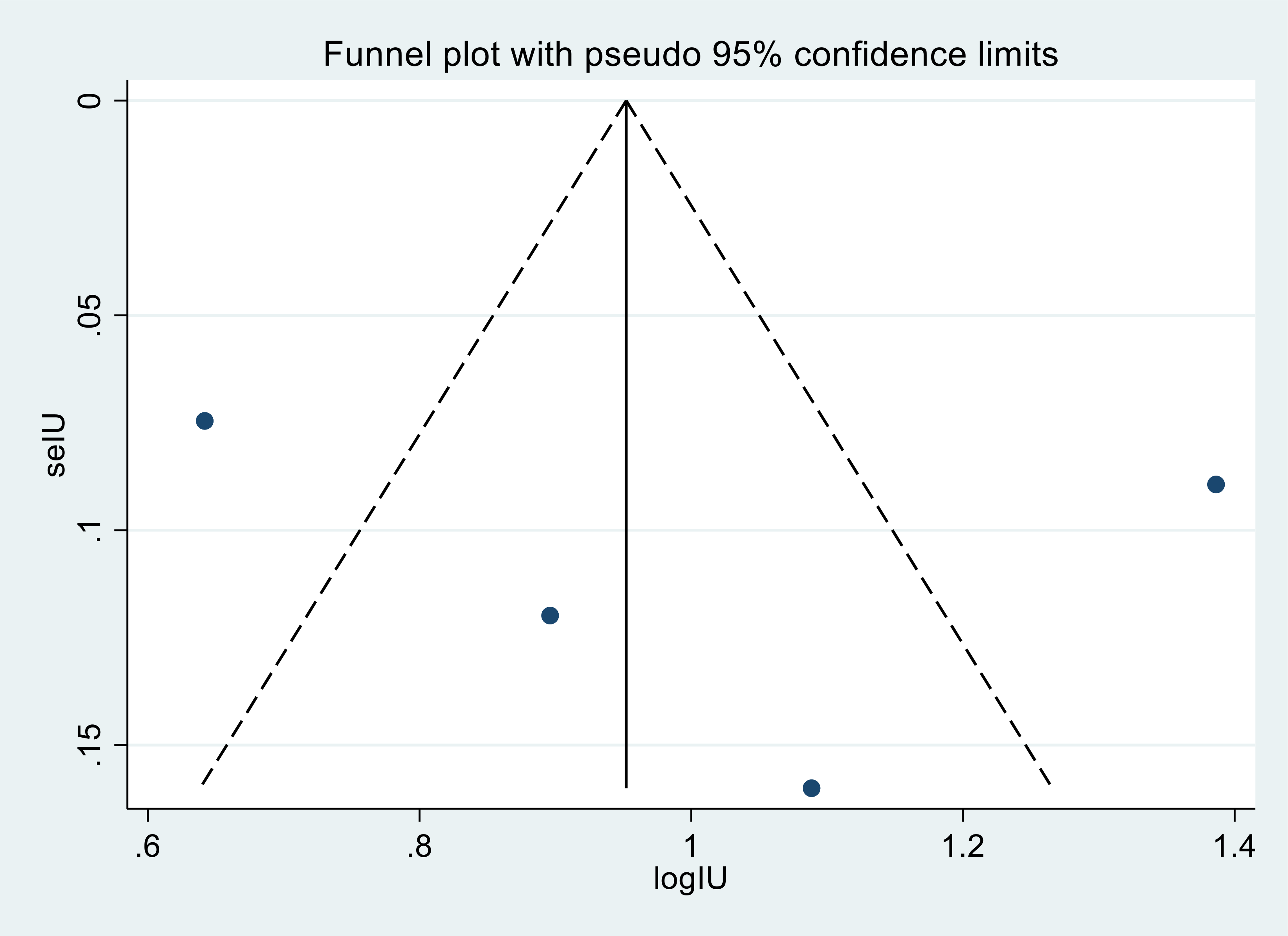
However, to check the publication bias among the included studies in this meta-analysis, a funnel plot was used to inspect the symmetrical distribution of the effect estimate and egger test statistics was done (Figure 3). The result of the funnel plot suggests asymmetric distribution of the effect estimates among the six included studies/articles indicates the presence of publication bias.

Funnel plot that depict publication bias in the 6 included studies of DHL among health professionals during the outbreak of coronavirus pandemic in Ethiopia, 2023.
Even though egger's test (p = 0.089) implies there is no evidence of small study effect, we forced to reject it as the funnel plot visually suggests the existence of publication bias. Given the facts that four of the included articles are outsized of the triangle.
Due to the presence of significant heterogeneity among the six included studies in this systematic review and meta-analysis, subgroup analysis was done to identify the potential sources of heterogeneity. Therefore, the subgroup analysis was done based on region, and study year. As a result, the studies which were conducted in Addis Ababa were one of the candidates for sources of heterogeneity (I2= 97.5%, p < 0.001), showing a high prevalence of high digital literacy 61% (95% CI:58,64) (Figure 4).

Forest plot of subgroup analysis based on region in the included studies/articles in Ethiopia, 2023.
The other source of heterogeneity was the period when studies were have been done. Since the inception of corona virus was too early in Ethiopia after the world’s breaking news was distributed from different communication technologies, different researches had been conducted. The study period was too challenging to identify the sources of the disease information.
The sources of heterogeneity as indicated below (Figure 5), studies conducted in 2021 were one of the potential sources. The heterogeneity (I2 = 95.3%, p < 0.001), shows a pooled prevalence of digital literacy at 56% (95% CI: 54,58). The reason for this could be due to the scientific findings that were most commonly apparent onwards after the known indications of the virus. Hence, publication rate of digital health literacy related articles increased after the virus appeared in Ethiopia. Health professionals had no choice but to use digital technologies for the management of patient care in their working environment.
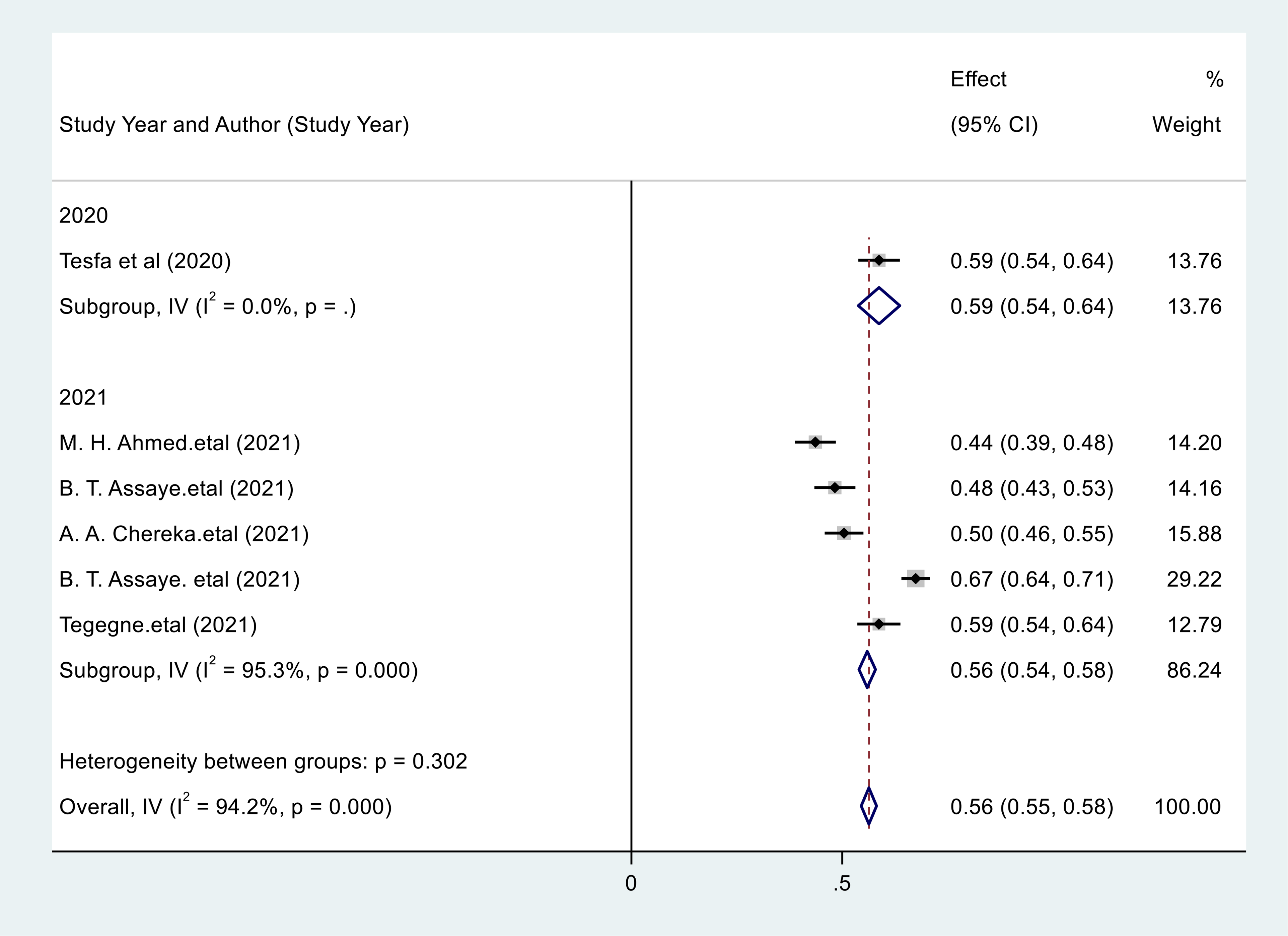
The forest plot indicating the pooled effect of study year and DHL of health professionals during the outbreak of coronavirus in Ethiopia, 2023.
Factors associated with digital health literacy among health professionals during the outbreak of COVID-19 pandemic
The random effect meta-analysis model was done to indicate the presence of severe heterogeneity (I2 = 89.9, p < 0.001) among the associated factors towards digital health literacy. In this systematic review, three included studies with factor perceive-usefulness were positively associated with high digital health literacy. The pooled odds of high digital health literacy among health care professionals who perceived the usefulness of being literate in digital health for health care services during the corona virus pandemic were 2.29 times higher than those who did not perceive as useful.
The result of this systematic review also revealed that four studies were found to estimate the pooled odds of internet use. The pooled odds of digital health literacy among those health professionals who used the internet were 2.72 (95% CI: 1.86,3.98) among those health professionals who were not internet users. With the same philosophy of interpretation, two studies discovered that training related to ICT had significant association with high level of digital health literacy. The pooled odds of high digital health literacy among those health professionals who got ICT training were 6.09 times (95% CI: 1.53,24.27) higher compared to those health professionals who did not get training.
Similarly, three studies were identified that indicate perceived ease of use is positively associated with health professionals’ high digital health literacy. The odds of high digital health literacy among health care professionals who thought perceived using digital health tools as being easy in digital health for healthcare services during the corona virus pandemic were 2.79 (95% CI: 1.81,4.23) times higher than their counter parts.
Furthermore, in this systematic review, two studies showed health professionals educational level has a significant association with high digital health literacy. The pooled odds of high digital health literacy among health professionals with an educational level of master's degree and above were 3.60 times (95% CI: 2.96,4.37) higher than those health professionals whose educational level where degree and diploma.
In addition, two studies specified health professionals who have a favorable attitude towards high digital health literacy. The pooled odds of high digital health literacy among health professionals with favorable attitude were 2.49 times (95% CI: 1.61,3.85) higher than those health professionals with unfavorable attitude (Figure 6).

Forest plot that indicates the pooled effect of factors associated with digital health literacy among health professionals during the outbreak of COVID-19 pandemic, Ethiopia, 2023.
A random effect meta-analysis pooling of aggregate data among the perceived ease of use as an associated factor was observed a severe heterogeneity among three included articles. I2 = 89.3%, and p = 0.000). (Figure 7).

Forest plot indicating the effect of perceived ease of use on digital health literacy a systematic review and meta-analysis among health professionals during the outbreak of corona virus pandemic in Ethiopia, 2023.
Funnel plot visual inspection of the effect of estimates was distributed asymmetrically (Figure 8).

Funnel plot of pooled odd ratio of perceived ease of use towards digital health literacy among health professionals during the outbreak of corona virus pandemic in Ethiopia, 2023.
Egger's test also revealed that there is no evidence for the presence of publication bias (p = 0.166) (Table 2).
Egger's test indicating for small study effect regarding the perceived ease of use of health professionals during the outbreak of corona virus pandemic in Ethiopia, 2023.

Test of H0: no small-study effects p = 0.166.
In this systematic review and meta-analysis, the association between internet use of health professionals and high digital health literacy was estimated using four included articles (Figure 9). The pooled odds of high digital health literacy among those health professionals who used internet were 2.72 (95% CI: 1.86,3.98) among those health professionals who were not internet users.
Funnel plot of the pooled odds ratio for internet use towards digital health literacy among health professionals during the outbreak of corona virus pandemic in Ethiopia, 2023.
Despite the Egger's test suggests that there is no evidence of publication bias among the four included articles, the effect of internet use on digital health literacy (p = 0.688).
Discussion
As a global concern, corona virus has shown unanticipated usage of health care technologies for the health sectors worldwide. Having attachments with digital technologies were have been the first choice to perform health care services that health care professionals delegated to function their routine tasks. Following a digital pattern and withdrawal of the existing work functions at health care institutions was the new paradigm during the outbreak of the corona virus pandemic globally and in Ethiopia specifically. With the new paradigm shift Ethiopian heath care institutions were among the first in adopting telecommunication-based (digital-oriented) health services to the population who needed the particular services. As an indication of this new shift, outpatient services that were supposed to be done in the health institutions were nearly closed and the routine health care services were also changed to the new array of tackling the transmission and distribution of the disease. To continue the essential functions of the health care system, digital health has been considered as stopgap tool for huge amount of cases. 39
As to the knowledge of the author, this study was the first in Ethiopia to estimate the pooled level of digital health literacy among health professionals during the outbreak of the corona virus disease. Therefore, the author calculated the pooled level of high digital health literacy among health professionals in Ethiopia was found to be 56% (95% CI: 55,58). The result is consistent with primary studies conducted in Amhara 35 and Germany. 9 However, the result of this study is higher than primary studies conducted in Malaysia, 40 Amhara 33 and Addis Ababa 32 48%, 50.4% and 53.81% respectively. The possible justification for this discrepancy might be due to the methodological design used for the primary studies to collect the survey data was internet based in the case of Malaysia that could minimize the responses of the participants intended to be answered. The other possible justification could be the inadequate sample size used to collect the data that can minimize the possibility of answering the digital health literacy questions.
The result of this systematic review and meta-analysis was lower than the results shown by a primary study conducted in Addis Ababa. 38 The possible reason for this difference might be due to the fact that health professionals whose demand to access digital health-related information in the cited place were higher as there was an immediate quarantine during the pandemic.
Additionally, the sub-group analysis results revealed that studies conducted in Addis Ababa showed higher digital health literacy level of 61% (95% CI: 58,64) as compared to the other regions, Amhara (56%), Oromia (44%) and the pooled result (56%) discovered in this systematic review and meta-analysis. The discrepancy could be due to the availability of good internet access (hence connectivity of internet penetration is better in Addis Ababa), technological-related trainings and access to these digital technologies. The other possible reason for this gap might be the socioeconomic disparities. Infrastructures available in Addis Ababa were supposed to create better employment opportunities, and access to health care services which can affect digital health literacy.
The pooled odds of high digital health literacy among health care professionals who perceived the usefulness of being literate in digital health for health care services during the corona virus pandemic were increased by 2.29 times as compared to those who did not perceive it as useful. This finding is consistent with studies conducted in South West Ethiopia, 14 Amhara Region, 36 Egypt, 28 and Jordan. 41 The possible justification could be health professionals perceive themselves as they have the ability to navigate, and utilize digital health technologies to access online health information sources, platforms and uncover the unknown to be known.
In this systematic review, the author discovered the pooled prevalence of internet use among health professionals during the pandemic era. The pooled odds of digital health literacy among those health professionals who used internet were 2.72 (95% CI:1.86,3.98) among those health professionals who were not internet users. This result is in line with a primary study conducted in Addis Ababa, 32 the University of Gondar Hospital 34 and with another country Poland. 18 The possible reason is due to the fact that internet has been considered as the super information high way by which health professionals could be able to communicate with their colleagues, patients and record the information generated from different sources. The other possible justification might be during the lockdown there was no other option than using internet for searching health-related information that can address patients’ need. Additionally, the use of internet has made it possible for patients to consult with their doctors at a distant which reduces the risk of exposure to the virus and assists with managing non-emergency medical issues.
The pooled odds of high digital health literacy among those health professionals who got ICT training were 6.09 times (95% CI: 1.53,24.27) higher compared to those health professionals who did not get training. This finding is consistent with a study done at teaching and referral hospitals in North West Ethiopia.35,36 The possible reason for this might be due to the fact that information communication technology trainings are important for healthcare professionals since it enables them to effectively use digital technology tools to enhance and improve healthcare services.
Furthermore, in this systematic review educational level has a significant association with high digital health literacy. The pooled odds of high digital health literacy among health professionals with educational level of master's degree and above were 3.60 times (95% CI: 2.96,4.37) higher than those health professionals whose educational level where degree and diploma. This result is consistent with primary studies conducted in Ethiopia,14,35 Egypt. 28 The best justification might be due to the empirical fact attaining higher education is a tool for health professionals’ proficiency and adaptive skills together with digital technology tools. With the same understanding, a study conducted in Taiwan 42 supports this idea by revealing assumptions; health professionals with higher educational degree were more likely to use digital technologies to access, evaluate, and made evidence-based decisions with up-to-date information use.
Moreover, in this systematic review and meta-analysis health professionals who had favorable attitude towards higher digital health literacy associated positively. The pooled odds of high digital health literacy among health professionals with favorable attitude were 2.49 times (95% CI: 1.61,3.85) higher than those health professionals with unfavorable attitude. The result of this systematic review and meta-analysis is in line with a study conducted in Anhui Province in China, 29 where the study participants showed a positive attitude towards digital health literacy, Malaysia, 31 Amhara, 35 Dessie in North East Ethiopia, 22 and Oromia. 14 The possible reason for this consistency might be due to the likelihood of health professionals’ acceptance and use of digital technologies for healthcare management is considered as digital competency. 43 Another possible idea which support this conclusion might be, Health professionals with Positive/Favorable attitude can help them be more committed and indicates they have the ability to understand the relevance and use of digital health technologies that pave to the way to create motivation in further use. In addition, having positive attitude can bring a digital culture that can help health professionals for better decision-making in patient care.14,22
Finally, health professionals perceived ease of use towards high digital health literacy has a positive association. The odds of high digital health literacy among health care professionals who thought perceived using digital health tools as being easy in digital health for healthcare services during the corona virus pandemic were 2.79 (95 CI: 1.81,4.23) times higher than their counterparts. This finding is supported by studies conducted in Slovenia, 29 North west and North east Ethiopia.14,34,36 The possible justification might be due to the fact that perceived ease of use is an important factor in digital health literacy which outlines that individuals’ digital health tools acceptance depends on their perception of its ease of use. 29 If health professionals perceive digital health tools as easy to use, they are more likely to embrace and integrate them into their workflows. This was a fashion during the pandemics when health professionals obliged to find digital tools to gain benefits that can enhance efficiency, improve communication, and access to broader range of resources about the virus. 44 Meanwhile, having this positive experience would reinforce their motivation and confidence to broadly develop their literacy about digital health.
Limitations
This systematic and meta-analysis tried to determine the pooled prevalence of digital health literacy among Ethiopian health professionals during the corona virus pandemic. Though the author tried to include articles published in English, their finding suggested the effects associated with the presence of publication bias. This bias would affect the generalizability of the finding as it might have introduced the missing of unpublished or exclusion of studies published other than English language. However, the author would like to endorse the upcoming researchers to find out and show the pooled effect of digital health literacy including the articles excluded with respect to methodological approaches (hence, we excluded studies published using the qualitative method).
This systematic review and Meta-Analysis do not include published papers other than Ethiopia, hence due to that we included only six published papers. Due to the variability of the samples included in the primary studies of the included articles, the author expected that the pooled prevalence would have been affected.
Conclusions and recommendations
With regard to the results identified in this systematic review and meta-analysis, the digital health literacy level of health professionals during the covid-19 pandemic was moderate. The author identified six significantly associated factors such as; internet use, perceived ease of use, favorable attitude, perceived usefulness, ICT training, and education. All had an effect on the digital health literacy level of health professionals. Our study suggests that using up-to-date and currently available information is mandatory during the occurrence of outbreak diseases like corona virus. Similarly, improving health professionals’ attitude would have the possibility of improving their perception to use digital health tools that can enhance patient care in the country. Providing technological trainings related to healthcare service deliveries would increase the health professionals’ decision-making process using the available evidences. To augment digital technology use, enhancing the perception of health professionals’ on how they can use these digital devices for healthcare services deliveries shall be strengthened. It is recommended that embracing health professionals on digital health literacy would enhance effective communications with patients, empower individual patients to make informed decisions about their health, improve health outcomes, and also provide contributions to advance health care in increasingly digital world. To advance digital health literacy, health professionals should get training that can advance their skills and realize the culture of digitalization.
Footnotes
Acknowledgements
We the authors of this systematic review and meta-analysis would like to forward our deepest gratitude to the researchers who conducted these primary studies used in this study. The author of this study (MDK) also wanted to extend his acknowledgement to his wife (Ehite) and Kid (Mama set, Yemariam M) for their great patient and kind supports from the inception to the final stage of the study.
Availability of data and material
All the data sets used and generated for the current study are available from the corresponding author upon a reasonable request.
Contributorship
MDK conceptualized the study, analyzed the data, and wrote the results, and drafted the manuscript. MHK and AM edited the manuscript. NK and SDK revised the manuscript. All the authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Since this study does not include human participants, ethical approval was not necessary.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MDK.
Patient and public involvement
No patient or public were involved in this research.