
Abstract
Objective
Despite of the tentative role of asbestos in chronic obstructive pulmonary disease (COPD), their lung function variation in relation to air pollution remains unexplored. This cross-sectional study aimed to explore the effects of air pollution on severe airway obstruction (SAO) in asbestos-related COPD.
Methods
COPD subjects were retrospectively recruited, and their asbestos exposure and SAO were verified using the existence of pleural plaque in chest X-ray and the predicted value of forced expiratory volume in 1 second in percentage less than 50%, respectively, followed by examining the association between PM2.5, PM10, SO2, NO2, O3, and CO and SAO stratified by asbestos exposure using regression model.
Results
SAO percentage was 67.2% (41/61) and 65.2% (15/23) in COPD subjects without and with asbestos exposure, respectively. An increased 3-day average concentration of CO and O3 correlated with SAO (odds ratio, 95% confidence interval: 0.06, 0.01-0.41 and 0.09, 0.01-0.64, respectively). Moreover, an increased 5-day average CO concentration also correlated with SAO (0.13, 0.02-0.71) prior to hospital admission of COPD subjects irrespective of asbestos exposure, and SAO failed to be associated with asbestos exposure.
Conclusions
Certain gaseous pollution at low concentration might generally exhibit a negative association with SAO in COPD subjects, indicating the negligibly negative impact of air pollution on lung function deterioration in asbestos-related COPD.
Introduction
There remains an ongoing effort to achieve ban on asbestos and the issue regarding asbestos-induced detrimental effects is still warranted to be monitored. The long latency of asbestos-related disease and the increasingly increased disease burden due to asbestos exposure required further measurements to screen asbestos-related disorders risk at the community level from a public health perspective.1,2 Individuals with asbestos exposure history and/or pleural plaques (PP) might experience lung function changes, and the forced vital capacity (FVC) and the predicted value of forced expiratory volume in 1 second in percentage (FEV1% predicted) appeared to be primary lung function parameters analyzed among asbestos exposed population,3–5 although the chronical pulmonary ventilation impairments should be interpreted case-by-case, suggesting the possible long-term impact of past asbestos exposure on respiratory dysfunction. Therefore, the health monitoring among individuals with asbestos exposure history is still necessary and might be useful to clarify long-term clinical manifestation due to past asbestos exposure.
Intriguingly, asbestos has been recently revealed to be a possible etiology of chronic obstructive pulmonary disease (COPD) and past asbestos exposure may increase the risk of COPD development even after cessation of asbestos exposure.6,7 COPD subjects with fixed airway obstruction might suffer from exacerbation, while severe airway obstruction (SAO), as determined using FEV1% predicted value, has been thought to be an indicator of poor outcomes for COPD subjects, which appears to depend on the extent of airway obstruction.8–10 Further exploration to characterize SAO between COPD subjects with and without asbestos exposure and its underlying factors might be valuable to screen the vulnerable asbestos-exposed population.
In addition to the nature of pathophysiological changes in the chest, deterioration in lung function might also be influenced by environmental pollution. COPD subjects are more vulnerable to ambient air pollution than healthier people, and lower lung function measurements were shown to be associated with air pollution.11,12 There is a hypothesis implying the putative role of air pollution in modifying asbestos-related abnormalities and increasing mortality risk of asbestos-related malignant diseases,13,14 although the possible impact of air pollution on respiratory abnormality and SAO risk among asbestos-exposed population remains largely unexplored.
The purpose of this study was to characterize lung function and laboratory examination parameters of COPD subjects stratified by asbestos exposure, followed by delineating the association between short-term air pollution exposure and SAO, which may be helpful to clarify underlying factors in association with clinical manifestation in COPD subjects with past asbestos exposure and to optimize health care management.
Methods
Study population
Local COPD inpatients with demographic and medical records due to the deterioration of respiratory symptom in the Department of Pulmonary and Critical Care Medicine at Cixi People’s Hospital between January 2019 and December 2020 were retrospectively retrieved, followed by excluding the inpatients without lung function and tumor-associated antigen measurements at their corresponding date of hospital admission and recruiting the remained inpatients. The recruited COPD inpatients were historically diagnosed and classified into asbestos-exposed inpatients as cases and non-exposed inpatients as controls, according to the information of the asbestos exposure and their corresponding chest X-ray images. The self-reported medication usage was arbitrarily defined to be yes and no if the medication prescription including corticosteroids, long-acting muscarine anticholinergic, or long-acting beta-agonists was reported. Meanwhile, liquefied petroleum gas, biofuel combustion and coal fuel as household fuel types for cooking using questionnaire was collected. This retrospective observational cross-sectional study followed the requirements of the strengthening the reporting of observational studies in epidemiology (STROBE) guideline 15 and was approved by Ethics Committee of Medical Research of Hangzhou Hospital for the Prevention and Treatment of Occupational Disease (Approval NO. HZFLS2025Y002, 4-12-2025), and the informed consent was waived due to the nature of already available data without disclosure of individual information. All patients’ details were de-identified and all procedures during this investigation were in accordance with the Helsinki Declaration of 1975 as revised in 2024.
Discrimination of asbestos-exposed subjects
The question about asbestos exposure or not was arbitrarily used to recall the possibility of asbestos exposure. The typical asbestos exposure scenarios for the investigated COPD inpatients might include occupational and para-occupational asbestos exposure in household textile workshops and large-scale textile manufactory during the production of asbestos-related products between the 1950s and 2010s, as indicated in our previous report. 16 Accordingly, occupational or para-occupational asbestos exposure was defined as the presence of asbestos exposure in this study. Further confirmation of pleural plaque presence using a chest X-ray image was used to identify an asbestos-exposed COPD case, otherwise a non-exposed COPD case was defined.
Lung function and pulmonary artery pressure assessment
FEV1 and FVC measurements using a JAEGER MasterScreen Pneumo spirometer were collected, followed by assessing the flow-volume loop and whether the changes in the highest and lowest absolute value of FVC and FEV1 were less than 0.20 L. Thereafter, the best results were reported as absolute values and as a percentage of the predicted values. The severity of airflow obstruction was assessed using the Global Initiative for Chronic Obstructive Lung Disease (GOLD) system, based on FEV1. It was recorded as GOLD stage ranging from 1 to 4, 17 followed by arbitrarily dividing airflow obstruction into mild/moderate and severe, based on 50% for FEV1% predicted cut-off point as previously employed. 18 Therefore, SAO was determined if FEV1% predicted value was less than 50%. Meanwhile, pulmonary artery pressure was measured using Philips iE33 ultrasound system to indicate possible pulmonary vascular disorders related to COPD. 19
Laboratory measurements collection
The data of routine blood examination using SYSMEX XN-1000 automatic haematology analyzer, cytokeratin 19 fragment (CYFRA 21-1) and squamous cell carcinoma antigen (SCC) using Abbott ARCHITECT I2000 chemiluminescent analyzer system, partial pressure of carbon dioxide (PaCO2) and partial pressure of oxygen (PaO2) with Werfen GEM3500 blood gas analyzer, and C-reaction protein (CRP) with Hitachi 7600 biochemistry analyzer were retrieved from a medical system in the local tertiary hospital, respectively.
Air pollutants data collection
The daily concentration of PM2.5, PM10, SO2, NO2, O3 and carbon monoxide (CO) in Cixi between January 2019 and December 2020 was publicly available and the corresponding data at Cixi monitoring site was retrieved from the air quality real-time reporting platform in Ningbo Municipal Bureau of Ecology and Environment (https://air.znbeemc.cn/StationAQ/Index). To verify the suitability of ambient monitoring data for the residential region of the investigated subjects, the zip code corresponding to the residential address of the investigated COPD inpatients in Cixi was collected and then employed to approximately calculate the linear distance between the living site and ambient environmental monitoring site in Cixi with official map using measuring tools (https://zhejiang.tianditu.gov.cn/map), as previously employed with modification using data from a monitoring station in the investigated participants’ residential area. 14
Statistical analysis
Demographic and clinical variables were expressed as mean with standard deviation and number with frequency, respectively. Air pollutants were shown as median with maximum and minimum value. Comparisons between two variables were determined using T-tests, Mann-Whitney U tests and Chi-square tests where applicable. To evaluate the short-term accumulative effects of air pollutants, the 1-day lag and 3-day, 5-day and 7-day average concentrations of air pollutants were calculated using the corresponding daily values, namely 1 day, 3 days, 5 days and 7 days prior to the date of hospital admission. Thereafter, the possible correlation between individual air pollutant and FEV1% predicted value and FEV1/FVC in percentage stratified by asbestos exposure was assessed in multivariate linear regression model with adjustment of gender, age, smoking, medication usage, and duration of COPD, and the coefficients was reported as standardization β along with 95% confidence intervals (CI) for unstandardized coefficient (B). Further logistic regression was employed to estimate the SAO risk due to increased air pollutants concentration (e.g., > median level of the corresponding air pollutant at observation time-point) stratified by asbestos exposure with adjustment of gender, age, smoking, medication usage, and duration of COPD, and the results were presented as odds ratio (OR) with 95% CI. All analyses were performed using IBM® SPSS® Statistics (version 26.0) and GraphPad Prism (Version 8.2.1) and a p-value <0.05 was considered as statistically significant.
Results
A total of 84 COPD subjects were recruited in this study, which included 61 subjects without asbestos exposure history, namely 14 subjects with occupational asbestos exposure and 9 subjects with para-occupational asbestos exposure (Figure 1). Meanwhile, the approximate linear distance between the air pollutant data monitoring site and the residential address for the investigated COPD subjects ranged from 2.12 kilometers to 26.80 kilometers. The number of COPD subjects living within 15, 20, and 30 kilometers were 77, 6 and 1, respectively. Moreover, liquefied petroleum gas, rather than biofuel combustion or coal, was the household cooking fuel among all these investigated COPD subjects. Their demographic, laboratory examination and lung function analysis are summarized in Table 1. There were no significant differences in age, gender, smoking rate, duration of COPD, medication usage, routine blood parameters, CYFRA 21-1, and SCC between COPD subjects with and without asbestos exposure history. Despite of the comparable blood gas measurements, GOLD stage, FEV1, FVC, and FEV1% predicted, FEV1/FVC was higher in COPD subjects with asbestos exposure than COPD subjects without asbestos exposure (p=0.040). The percentage of SAO was 67.2% and 65.2% for COPD subjects without and with asbestos exposure history, respectively (p=0.863). The flowchart of selection of asbestos exposed and non-asbestos exposed chronic obstructive pulmonary disease cases. Characteristics of chronic obstructive pulmonary disease subjects by asbestos exposure.

Overall, all the 1-day, 3-day, 5-day and 7-day average concentrations of PM10, PM2.5, SO2, NO2, CO, and O3 were comparable between COPD subjects with and without asbestos exposure history, respectively (Figure 2). Briefly, the average concentration was 43.00∼56.28 μg/m3 for PM10, 27.00∼34.14 μg/m3 for PM2.5, 99.00∼109.86 μg/cm3 for O3, 0.63∼0.70 mg/m3 for CO, from 22∼25.28 μg/m3 for NO2, and 8.33∼9 μg/m3 for SO2 for COPD subjects with asbestos exposure, respectively. Its value was 49.00∼56 μg/m3 for PM10, 30∼33.42 μg/m3 for PM2.5, 98.00∼108.57 μg/cm3 for O3, 0.6∼0.63 mg/m3 for CO, 21∼25.67 μg/m3 for NO2, and 8∼9.2 μg/m3 for SO2 among COPD subjects without asbestos exposure, respectively. The air pollutants concentrations prior to the date of hospital admission of chronic obstructive pulmonary disease cases.
Coefficients between lung function parameters and air pollutant in chronic obstructive pulmonary disease subjects with and without asbestos exposur

The data were determined in multivariate linear regression model with adjustment of gender, age, smoking, medication usage, and duration of COPD. CI, confidence interval.
Adjusted odds ratio of severe airway obstruction among COPD cases stratified by asbestos exposure in response to relative higher levels of air pollutant (reference: lower levels).
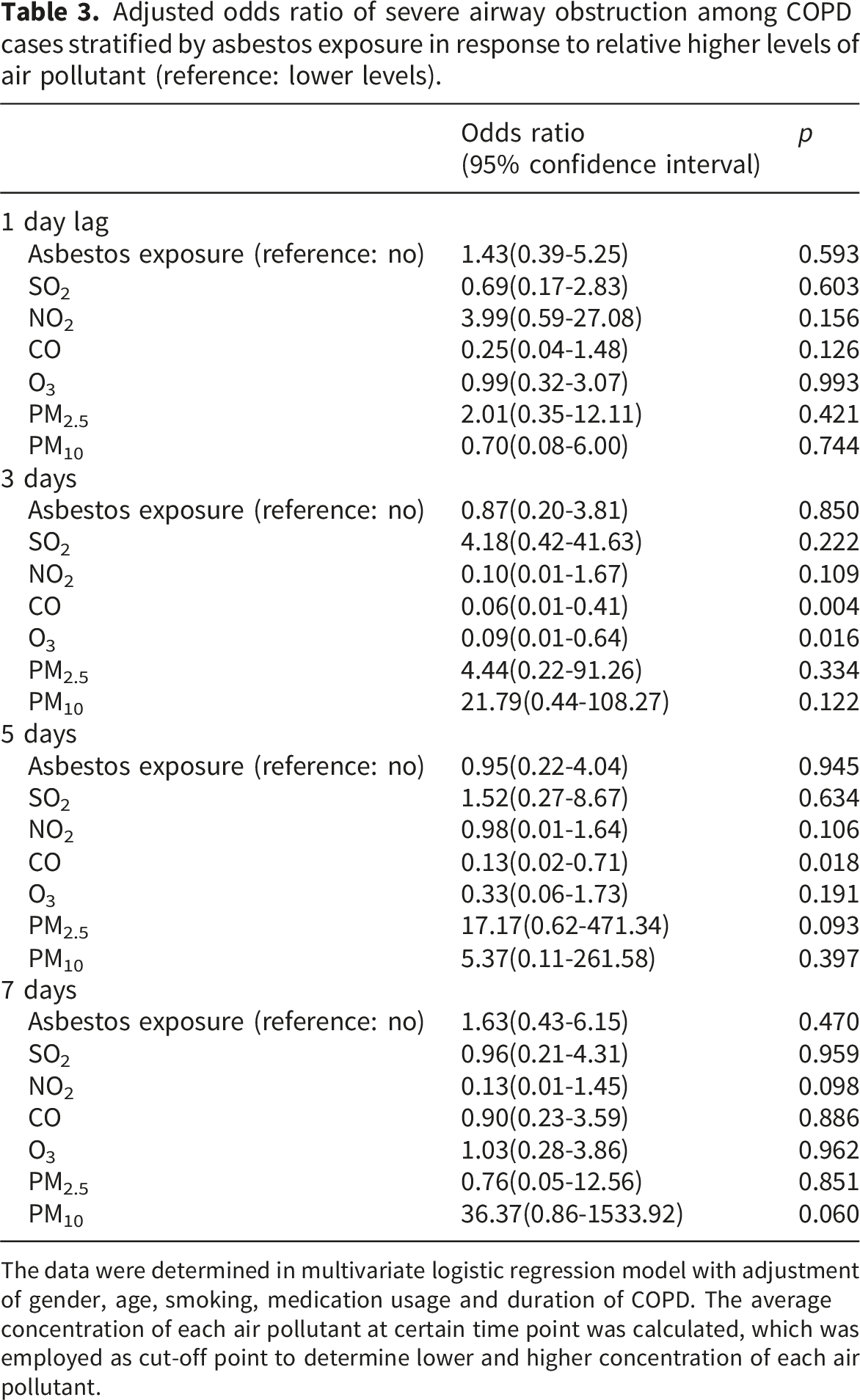
The data were determined in multivariate logistic regression model with adjustment of gender, age, smoking, medication usage and duration of COPD. The average concentration of each air pollutant at certain time point was calculated, which was employed as cut-off point to determine lower and higher concentration of each air pollutant.
Discussion
This is the first study revealing the comparable clinical manifestation between COPD inpatients with and without asbestos exposure history, although COPD subjects with asbestos exposure appear to present marginal but significant increment in FEV1/FVC. Short-term air pollution episode had no significant impact on FEV1/FVC for COPD subjects regardless of past asbestos exposure, but certain gaseous pollution had influence on FEV1% predicted values for COPD subjects without asbestos exposure. Intriguingly, short-term CO and/or O3 concentration elevation appeared to be associated with lower SAO risk for COPD subjects independent of asbestos exposure.
An increased rate of pulmonary impairment was documented, especially for asbestos exposed individuals with PP, 20 and these subjects likely experienced COPD as reported here. Previous studies showed that the COPD incidence is 16% among insulators, and 37.7% of asbestos exposed subjects had FEV1/FVC less than 70%, suggesting a relationship between asbestos exposure and COPD.21,22 Longer asbestos exposures might increase COPD risk as previously reported, 7 although a past asbestos exposure might not accelerate COPD development or increase the SAO risk as compared with subjects without asbestos exposure as shown here, which implied the plausible role of asbestos in driving COPD development rather than progression. Nonetheless, COPD phenotype in subjects currently exposed to asbestos remains to be investigated, and COPD monitoring seems to be an alternative measurement to interpret the asbestos-related mortality and morbidity.
Past asbestos exposure apparently had no significant impact on blood gas analysis or lung function measurements except for FEV1/FVC among COPD cases, which is consistent with the comparable GOLD stage and percentage of SAO between COPD subjects with and without asbestos exposure as reported here. The marginally increased FEV1/FVC for COPD subjects with asbestos exposure, which is partially consistent with a prior study showing a tendency toward higher FEV1/FVC in asbestos-exposed individuals comparted to apparently healthy controls. 4 This observation might be tentatively explained by the hyperventilation in asbestos exposed individuals with PP. Nonetheless, lung function parameters among individuals with PP might be modified by unidentified abnormalities or other factors. Individuals with asbestos exposure and/or PP likely suffer from lung cancer, which appeared to be associated with airflow limitation.23,24 The comparable lung cancer-related serum biomarkers (e.g., CYFRA 21-1 and SCC) between COPD subjects with and without asbestos exposure, as reported here, precluded the possible modifying effects of malignant abnormality factors on lung function changes. Further prospective assessment of respiratory parameters is still necessary to delineate the underlying indicators associated with lung function in asbestos-exposed COPD subjects.
FEV1/FVC appeared to be stable among asbestos-exposed individuals, regardless of PP and/or lung fibrosis, during a 4-year follow-up. 25 This is in line with the current finding showing that short-term air pollution failed to affect FEV1/FVC in our multivariate linear regression analysis adjusted for COPD duration, gender, medication usage, and smoking, among COPD subjects aged >70 years old, regardless of asbestos exposure. This might partially support the concept that deposited fiber, airborne dust and smoking, rather than negligible fiber in breathing air, might modify lung function tests such as FEV1/FVC.26,27 Nevertheless, the impact of air pollution on FEV1/FVC in asbestos exposed COPD subjects remains to be analyzed especially for non-smokers with past asbestos exposure quantification data or with definitive inhaled fiber exposure quantification information.
The impact of air pollution on FEV1% predicted values appears inconclusive. The negative association between O3 and FEV1% predicted values was demonstrated in smokers with respiratory morbidity. 28 Comparably, short-term O3 exposure tended to correlate with lower FEV1% predicted values for COPD cases without asbestos exposure, but not for asbestos-exposed COPD cases irrespective of smoking. This is not fully consistent with a previous study reporting no effect of short-term or long-term O3 exposure on FEV1% predicted values for COPD cases. 29 Pulmonary emphysema evaluation complemented with air pollution measurements may be helpful to address these apparently inconsistent observations, because the link between O3 and emphysema severity indicates COPD exacerbations.30,31 A positive relationship between SO2 and FEV1% predicted values was observed for COPD cases without asbestos exposure, which might be tentatively explained by the concept of marginal and varying adverse effects of SO2 in COPD cases. 32
CO and/or O3 exposure apparently reduced SAO risk for COPD subjects irrespective of past asbestos exposure and PP, as found here, which partially agreed with the point indicating the reduced COPD hospitalization risk in association with short-term and low levels of CO exposure, which may provide some acute protection against COPD exacerbation.33,34 The negative association was also documented in long-term observational period under condition of CO concentrations ranging from 0.59 to 0.64 mg/m3 in China. 35 Nonetheless, either a null or a positive association between ambient CO and respiratory symptoms was reported for COPD individuals depending on the specific type of symptom, 36 which likely complicated the effects of ambient CO on COPD morbidity. Alternatively, it should also be mentioned that the possibility of reversible airway obstruction among COPD subjects with or without asbestos exposure. 37 Additionally, elders might be unresponsive to O3, and lung dysfunction could be exacerbated by extreme O3 pollution, although the association between O3 exposure and airflow obstruction is weak.38,39 It should be mentioned that the CO and O3 concentration in Cixi during the investigated period is lower than 4 mg/m3 and 160 μg/m3 as indicated in Chinese Ambient Air Quality Standards Grade II (GB3095-2012) (revised in 2018), respectively and is also comparable to 0.7 mg/m3 for CO concentration and 94.2 μg/m3 for O3 concentration in Ningbo, which is approximately 50 kilometers southeast of Cixi. 40 Accordingly, the sensitivity of COPD subjects to O3 at low pollution levels remains to be analyzed to verify the apparent protective role of low O3 exposure in reducing SAO.
There are some limitations to be addressed. This study sought to elucidate the air pollution on COPD severity and found a marginal, putative clue indicating potential factors associated with SAO fluctuation, classified by asbestos exposure history (e.g., yes or no). However, the current finding might suffer from uncertainty to some extent and is unable to provide cause-effect interpretation because of the nature of the cross-sectional study design and the failure of power analyses raised by the scarce evidence of COPD incidence, although the impact of certain gaseous pollutants on SAO risk for COPD subjects independent of asbestos exposure was implied. This finding deserves to be examined in a large-scale COPD population including participants with semi-quantification of past and/or current asbestos exposure in a sophisticated study (e.g., determination of power and sample size) using the updated COPD incidence data around 8.75% obtained from a cohort of asbestos-exposed population.7,41 Despite of the duration of COPD and medication usage included as covariates in our analyses, the unavailability of baseline COPD severity and/or lung function measurements might require further panel study design to define the change in lung function parameters (e.g., FVC and FEV1) and SAO frequency in association with the fluctuation of airborne pollutants concentration using consecutive monitoring data with adjustment of socioeconomic factors (e.g., marriage and income status) and comprehensive trace of house-hold airborne contamination. Moreover, the current evidence was applicable under the circumstance of an air pollution episode falling within the national criteria. Still, the worst pollution situation above the national standard should be interpreted with further exploration.
Conclusions
Low concentration of O3 and CO during short-term exposure may be negatively associated with SAO risk in COPD subjects irrespective of past asbestos exposure and/or PP. Asbestos-exposed COPD subjects may be unlikely susceptible to lung function deterioration in response to short-term air pollution episode. A further cohort study is warranted to verify the current finding and alleviate anxiety among COPD individuals without parenchyma and interstitial pulmonary abnormalities during air pollution episode.
Footnotes
Ethical considerations
This study was approved by Ethics Committee of Medical Research of Hangzhou Hospital for the Prevention and Treatment of Occupational Disease (Approval NO. HZFLS2025Y002, 4-12-2025).
Consent to participate
The informed consent was waived due to the nature of already available data without disclosure of individual information, which was waived by Ethics Committee of Medical Research of Hangzhou Hospital for the Prevention and Treatment of Occupational Disease.
Author contributions
Data curation, Formal analysis, Methodology, Writing-review & editing: CYC; Data curation, Methodology, Writing-review & editing: XNL; Conceptualization, Formal analysis, Methodology, Writing-original draft, Writing-review & editing, Supervision: MY. All authors have read and agreed to the current version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by Zhejiang Science and Technology Plan for Disease Prevention and Control (Project No. 2026JKY187) and the Presidential Foundation of Hangzhou Hospital for the Prevention and Treatment of Occupational Disease (2025HZFKY1). The sponsor had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Declaration of conflicting interests
All authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data generated or analyzed during this study are included in this published article, while all the original data could be provided under reasonable request in accordance with the local regulations/laws of medical information utilization.