
Abstract
Background
Cognitive Impairment (CI) represents an important extra-pulmonary feature of Chronic Obstructive Pulmonary Disease (COPD), in which its prevalence remains under-recognised. The Montreal Cognitive Assessment (MoCA) is a validated screening test for detecting CI.
Objectives
The use of the MoCA in clinically stable COPD in routine practice. Secondary aim: CI prevalence in COPD.
Design
Feasibility study.
Methods
Quantitative and qualitative data were collected in 30 COPD patients, aged ≥65 years, at the Outpatient Department in Modena (Italy).
Results
The MoCA administration was on average 11 min. Patient feedback was positive. The COPD participants (mean age 75 years) viewed the test favourably and felt that understanding more about cognitive function would help improve their care. The median MoCA score was 23 with 10% of patients had moderate CI. The prevalence of CI was 84%.
Conclusion
The MoCA is not time-consuming and should be incorporated in daily routine to identify CI in COPD, in which the prevalence of mild CI remains high. Results warrant further studies in larger populations to confirm feasibility in clinical practice.
Keywords
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a common and complex disease characterised by progressive airflow limitation with persistent respiratory symptoms, especially dyspnoea, and acute worsening of symptoms, called exacerbations, that are important events in the disease management. 1 Comorbidities are frequently associated with pulmonary disease and their identification is needed to understand COPD severity.2,3 As the worlds’ population ages, more people will develop the long-term effects of exposure to COPD risk factors, mainly cigarette smoking. This illness is currently considered as an age-related disease with the highest prevalence among individuals >60 years.
Cognitive Impairment (CI) is more frequent in older age and involves problems with memory, thinking, language and writing. 4 CI has been shown as highly prevalent in patients living with COPD as an important extra-pulmonary comorbidity.5,6 Presence of CI in COPD has important consequences. First, screening of cognitive function may help people better manage their disease, for example by ensuring that they have the cognitive ability to follow the correct inhalation technique. Additionally, understanding the real impact of CI on COPD can define the true burden of the disease, for example the need for additional help in activities of daily living. 7
Many research studies have previously used the Montreal Cognitive Assessment (MoCA) 8 in people with COPD.9–11 The MoCA is a reliable screening test with high sensitivity and specificity for detecting mild CI in COPD patients. The Mini-Mental State Examination (MMSE) 12 is also commonly used tool for cognitive screening in medical practice, particularly among older adults and for clinical research in patients with COPD.13,14 However, comparing with the MMSE, the MoCA seems to have better diagnostic performance for detecting mild CI. 15 The well-established approach using the MoCA in COPD therefore facilitated a feasibility study to help further establish the use of this tool in routine practice.
The primary aim of this study was to evaluate the feasibility of using the MoCA in older patients with scheduled visit for COPD. Feasibility was assessed through enrolment in the study of clinically stable COPD patients and completion of MoCA. Considering that CI is still underestimated and under-recognised in this population,5,6 the study also examined the prevalence of CI in COPD as a secondary aim.
Materials and methods
Study design and participants
This observational study was conducted in patients with COPD referred to the Outpatient Respiratory Department of Hospital Policlinico in Modena for scheduled visit between 8th November 2019 and 21st May 2020. In June 2020 study recruitment was stopped due to COVID-19 pandemic restrictions and additional case-load of inpatients. Authority in Italy to conduct the study was granted by the Ethics Committee of Hospital Policlinico (Reference 888/2019/OSS/AOUMO).
The study was designed to evaluate the feasibility of using the MoCA to detect CI in older (≥ 65 years) patients with COPD in routine practice.
The inclusion criteria were diagnosis of COPD at least 12 months prior to the study, age ≥ 65 years, smoking history ≥10 pack-years. Patients at screening visit performed spirometry to confirm diagnosis (post-bronchodilator persistent airflow limitation) according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations.1,16,17 Patients with restrictive pattern on spirometry (total lung capacity ≤ 80%) were not included.
The exclusion criteria were acute exacerbation of COPD in the previous four weeks, concomitant asthma or Interstitial Lung Disease (ILD), lung cancer or other malignancies, neuromuscular or neurodegenerative diseases, chronic psychiatric disorder on treatment, immunodeficiency disorders including HIV, history of alcohol or drug abuse in the last year, patient not able to perform lung function test or to give informed consent.
For the occurrence of COVID-19 pandemic in March 2020, previous SARS-CoV-2 infection or admission for COVID-19 was added as a further exclusion criterion.
Definitions
Smoking habit was calculated as pack/years and participants classified into former smokers and current smokers. Duration of COPD, number of COPD acute exacerbations and/or hospitalisations due to exacerbation or different reason in the previous year, patient medication list, and number of comorbidities calculated as age-adjusted Charlson Comorbidity Index (CCI) were collected (Supplemental File). 18 The diagnosis of a comorbidity was confirmed by patient's medication list or medical record. The burden of COPD symptoms was assessed using the COPD Assessment Test (CAT) (Supplemental File). 19
Lung function testing and COPD classification
At screening visit, spirometry was performed1,16,17 and patients were classified based on the severity of airflow limitation (Grades 1 to 4) and the symptom burden and risk of exacerbation (Groups A to D) according to 2021 GOLD recommendations. 1
Cognitive impairment
CI was assessed using the MoCA test (Italian version; Supplemental File) and administered by the researcher. Training was conducted to ensure proper administration of the test. The MoCA is a tool used to assess deficits in different cognitive domains: visuospatial ability, executive function, language, memory, attention, naming, orientation, delayed recall, and abstraction. It is scored out of a total of 30 points and a cut-off of <26 may indicate CI. The MoCA grade score is: 26–30 as normal cognition, 18–25 as mild CI, 10–17 as moderate CI, <10 as severe CI. 8 Family history of dementia as a risk factor was collected at enrolment.
Education level
Education level was classified into five categories: primary school, middle school, secondary school, and bachelor/master degree. Participants receiving no formal education were excluded. For analysis, education was treated as a dichotomous variable indicating either higher education (>12 years; bachelor/master degree) or lower education (≤12 years; primary to secondary school).
Data examination and qualitative data
All data obtained from the study procedures of each patient were anonymised and entered into an electronic database only used for the scientific purposes of the research. All observations were conveyed in table form. Continuous variables were summarised as means and standard deviations (SDs); categorical variables were summarised as frequencies and percentages. We did not statistically analyse data due to the small group of patients and resulting lack of appropriate power. The purpose of this study was also to collect patients’ personal perspectives. The participants’ qualitative feedback was transcribed. Transcripts were reviewed by a senior researcher (AV) to identify key themes that corresponded to the study goals.
Results
Participants
Thirty-one patients were asked for completing the MoCA. One patient was excluded as illiterate. A total of 30 patients, aged 75 years (range 65–84), were included; 53% were male (n = 16). All patients underwent comprehensive clinical and functional assessment, and MoCA test. Baseline characteristics and collected data are shown in Table 1. The population was White/Caucasian (100%). Seventy-seven percent of patients had a primary-middle school qualification. Current smokers were 23% (mean pack/years 36). GOLD Grade 2 was in 47% of patients, GOLD 3 and 4 in 37%. The patients were 57% in GOLD group B. Overall, the patients were non-frequent exacerbators: the number of COPD acute exacerbations per year ranged between 0 and 1. The mean CAT score was 13.5. None of the included patients was receiving long-term oxygen therapy. COPD duration was on average seven years. The mean CCI was 4.5 (age-adjusted). The main comorbidities associated with COPD were: hypertension (70%), hyperlipidaemia (43%), ischaemic heart disease (20%), Type-2 diabetes (17%), and osteoporosis (17%). None of the participants had concomitant depression or anxiety on treatment.
Demographics and variables by MoCA cut-off score.
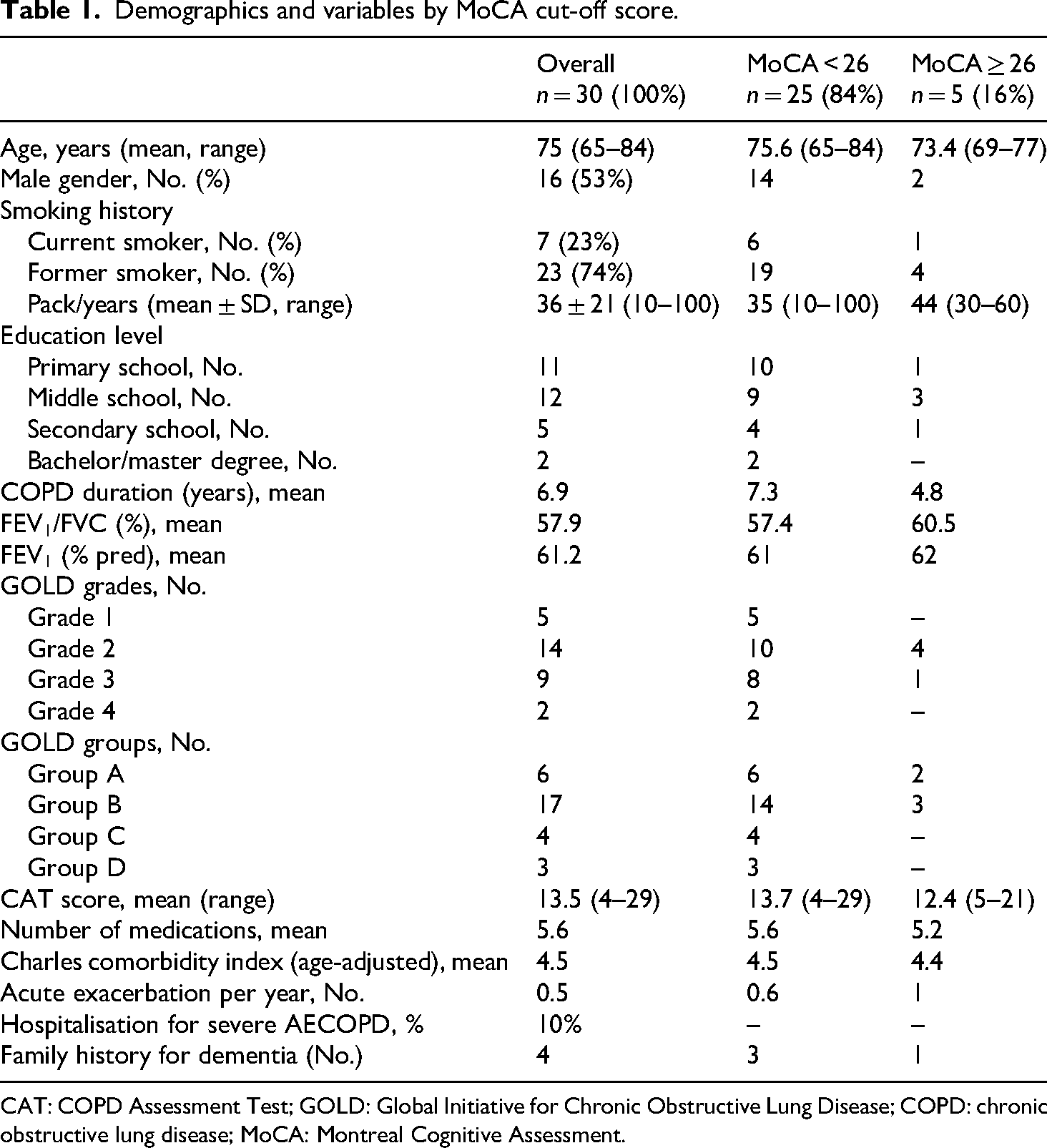
CAT: COPD Assessment Test; GOLD: Global Initiative for Chronic Obstructive Lung Disease; COPD: chronic obstructive lung disease; MoCA: Montreal Cognitive Assessment.
Feasibility
Thirty patients consented to participate in the study and completed the test. The MoCA administration took on average 11 min (range 10.3–12.1). Patient compliance was high (100% adherence). Only one patient was not able to complete the test as illiterate. Prior to testing, six patients were concerned about their performance and expressed feeling of anxiety. Of note, the participants said that they were not likely able to do the test and felt that assessing cognitive function would demonstrate that they had memory loss.
‘The memory is a big problem to me because I forget many things that I have to do the same day and I often need for help … so I think I cannot go well in the test’. Male participant, 69 years, middle school, ex-smoker, 30 pack/years, COPD duration 12 years, number of medications 7.
‘This test, to me, is impossible to do! I am feeling nervous … and I fear I will fail!’ Male participant, 77 years, middle school, ex-smoker, 60 pack/years, COPD duration 11 years, number of medications 8.
‘For me the embarrassment is a huge one … my wife says always that I am also able no more to write!’ Male participant, 75 years, secondary school, current smoker, 40 pack/years, COPD duration 8 years, number of medications 11.
‘I am really interested in … but I just think that I will not able to give valid answers to the questions because I am very old’. Female participant, 82 years, middle school, current smoker, 15 pack/years, COPD duration 11 years, number of medications 6.
‘Memory is something that I struggle with on a day-to-day basis, and I will probably not pass the test’. Male participant, 74 years, secondary school, ex-smoker, 40 pack/years, COPD duration 15 years, number of medications 3.
‘The thing that really makes me concerned is the question about attention … I guess since I am 70 … I often lose concentration’. Female participant, 70 years, middle school, ex-smoker, 30 pack/years, COPD duration 1 year, number of medications 6.
Prevalence of CI
The prevalence of CI in COPD was 84% (25/30 patients). The median MoCA score was 23.5 (range 11–27). Out of 30 patients, 22 had mild CI (73%), whereas three had moderate CI (10%). Family history of dementia was found in 13% of participants (4/30). Only three patients, of which family members were affected by dementia, had mild CI. The patients with normal cognitive function had COPD duration on average of 4.8 years compared to patients with CI who were living with COPD for seven years after diagnosis. The same burden of comorbidities as value of CCI was observed both in the participants with CI and with normal cognitive function (Table 1 and Supplemental File).
Discussion
The findings of this feasibility study suggest that the use of MoCA should be incorporated more frequently in outpatients setting to help identify mild CI in patients with COPD. We found that the prevalence of mild CI was 73%, and 10% of patients had moderate CI. The median MoCA score was 23. The qualitative responses also demonstrated that the patients valued the addition of the test. Our findings are in line with literature reporting high prevalence in COPD population, in which mild CI is associated with advancing years of age.20,21 Our results are comparable with previous research studies including stable COPD patients with moderate-to-very severe grade. The MoCA values range was 11–27 in the cohort, 18–27 after excluding patients with score < 18 (that totally account for 10%). One study showed similar findings (range 18–25), including only patients with mild CI in the analysis. 20 Different range of values (20–30) was observed in another study, yet confirming high risk of mild CI in moderate-to-severe COPD. 10 Whilst these authors reported lower rates of mild CI compared to our study, the proportion of COPD patients with mild CI was relevant, irrespective of age.
Initially, the study was designed to investigate the potentially risk factors associated with CI in COPD. Due to the pandemic that interrupted patient recruitment, we changed the focus of the study on the feasibility of using the MoCA in scheduled visits for ongoing COPD management. However, limited data had been collected when the study was terminated and in order to maximise research integrity and publish available data, feasibility results were presented instead.
Regardless of the small sample, this study provided some key feasibility findings.
Secondly, the study excluded COPD patients with relevant psychiatric comorbidities, including depression and anxiety on treatment. The COPD population included good representation of both men and women, a range of years since diagnosis, disease diagnosis based on GOLD recommendations, and non-frequent exacerbators. Based only on observation, duration of COPD seems to play a role in CI.
Third, the optimal compliance and interest by the patients and the high prevalence of mild CI have valuable implications in clinical practice and provide additional elements for COPD care management. The COPD patients self-report loss of memory and the MoCA is suitable for any individual who is experiencing memory difficulties. Chest physicians should take into account this aspect and include the test also for preventing dementia.
Whilst CI assessment deserves consideration, evaluation of cognitive function in daily practice can be hindered by significant barriers such as limited time, lack of screening related knowledge, patient discomfort or hesitation. 23 Using our protocol, we intended to play a role in making conversation about cognitive function as a part of routine care in COPD outpatients, of which evidence remains limited except than in clinical research. The staff working in the outpatient setting for the patient recruitment shared the purpose for cognitive screening and supported the process. Therefore, having physicians trained in cognitive screening test administration and availability of staff as facilitators made possible the patient involvement. In addition, the low time-consuming for taking the MoCA test confirmed the feasibility for use. Limitations of note were solely that the study was preliminary, the patient recruitment was stopped due to COVID-19 pandemic and the resulting study was underpowered due to the small sample.
Conclusion
The MoCA is a reliable indicator of cognitive function that represents a valuable tool for clinical practice in COPD, as it is a low-cost, not time-consuming and valued by patients. Therefore, a brief cognitive screening test proposal for individuals with COPD can determine the current level of autonomy of the patient and capture patient-level complexity. In fact, taking into account cognitive status in COPD patients is critical not only for detecting CI but also for improving disease management. 24 Evidence showed that patient compliance and/or adherence to therapy with correct inhaler use technique are central to successfully managing COPD25,26 and need to be routinely verified. Furthermore, patients in which MoCA leads to CI detection can be referred to Geriatric or Neurology Department for consultation. In conclusion, we recommend the use regularly of MoCA in patients with COPD in stable condition.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251347114 - Supplemental material for The use of the MoCA in cognitive impairment for older patients with Chronic Obstructive Pulmonary disease: A preliminary study
Supplemental material, sj-docx-1-sci-10.1177_00368504251347114 for The use of the MoCA in cognitive impairment for older patients with Chronic Obstructive Pulmonary disease: A preliminary study by Alessia Verduri, Martin O’Neill, Federica Ghinassi, Federico Guidotti, Maria Serena Simeone, Valentina Ruggieri, Enrico Clini and Jonathan Hewitt in Science Progress
Footnotes
Acknowledgments
Ethics approval and consent to participate
The study protocol, copy of questionnaires, consent form and patient information sheet were submitted to the local Ethics Committee (University Hospital Policlinico, Modena, Italy). The study obtained the ethical approval on 22nd October 2019 (Reference 888/2019/OSS/AOUMO). The study was performed in accordance with Good Clinical Practice (GCP/ICH E6) and conformed to the Declaration of Helsinki.
Author contributions
Alessia Verduri: conceptualisation, data curation, formal analysis, methodology, supervision, writing – original draft and writing – review and editing; Martin O’Neill: methodology, and writing – review and editing; Federica Ghinassi: writing – review and editing; Federico Guidotti: writing – review and editing; Maria Serena Simeone: writing – review and editing; Valentina Ruggieri: project administration and writing – review and editing; Enrico Clini: methodology, supervision, validation, and writing – review and editing; and Jonathan Hewitt: conceptualisation, methodology, supervision, validation, and writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset used and analysed during the study is available from the corresponding author on reasonable request and with ethical permission.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.