
Abstract
Background
Sepsis, caused by a dysregulated host response to infection, is a life-threatening condition linked to nearly one-fifth of deaths worldwide. As a biomarker of myocardial stress, N-terminal pro B-type natriuretic peptide (NT-proBNP) has gained attention for its potential association with clinical outcomes in sepsis patients. This study investigated its association with short- and long-term mortality in sepsis.
Methods
This retrospective observational cohort study utilized data from the Medical Information Mart for Intensive Care IV database. Sepsis patients on their first intensive care unit admission with NT-proBNP measured within 24 h were categorized into four groups based on their natural log-transformed levels. The primary endpoint was 30-day all-cause mortality (ACM), with secondary endpoints of 90-day and 1-year ACM. Cox models, Kaplan–Meier curves, restricted cubic splines (RCS), and subgroup analyses were performed to assess the relationship between log(NT-proBNP) and 30-day, 90-day, and 1-year ACM.
Results
The study cohort consisted of 1237 patients, with 54.41% male. The 30-day, 90-day, and 1-year ACM rates were 27.41%, 29.99%, and 31.69%, respectively. Multivariate Cox analysis showed that log(NT-proBNP) was independently associated with higher risks of 30-day ACM (hazard ratio[HR] 1.12 [95% confidence interval (CI) 1.03–1.22]; P = 0.01), 90-day ACM (HR 1.12 [95% CI 1.03–1.22]; P = 0.005), and 1-year ACM (HR 1.11 [95% CI 1.03–1.20]; P = 0.007). These associations remained robust in sensitivity analyses. The RCS curves demonstrated a linear increase in ACM risk as log(NT-proBNP) levels rose. Subgroup analyses confirmed these associations across different patient groups.
Conclusion
Elevated log(NT-proBNP) in critically ill sepsis patients are significantly and independently associated with higher 30-day, 90-day, and 1-year ACM, suggesting that NT-proBNP may serve as a valuable risk marker for both short- and long-term mortality in this population.
Keywords
Introduction
Sepsis, defined as life-threatening organ dysfunction caused by a dysregulated host response to infection, is a leading cause of mortality and critical illness worldwide. 1 It is estimated that 48.9 million cases of sepsis occurred worldwide in 2017, with 11.0 million deaths attributed to sepsis, accounting for around one-fifth of all global deaths. 2 In Asia, sepsis affects 22.4% of intensive care unit (ICU) patients, with hospital mortality reaching 32.6%. Mortality rates are even higher in low- and middle-income countries. These striking figures underscore the urgent need for effective early risk assessment. Timely identification of high-risk patients enables critical interventions such as antibiotic therapy, fluid resuscitation, and organ support, which are essential for improving outcomes.
N-terminal pro-B-type natriuretic peptide (NT-proBNP) is an inactive prohormone derived from the cleavage of pro-B-type natriuretic peptide (BNP), which is primarily secreted by ventricular myocardial cells in response to myocardial stretch and stress. Compared to its active counterpart BNP, NT-proBNP exhibits a longer plasma half-life and greater biochemical stability, but its levels are influenced by aging, renal dysfunction, and obesity.3,4 The role of NT-proBNP in heart failure (HF) screening, diagnosis, and prognosis evaluation has been well-established. 5 Low levels typically exclude HF, while high levels are often indicative of poor prognosis. In asymptomatic high-risk individuals, elevated NT-proBNP levels can serve as an early warning, guiding timely interventions to prevent and delay the onset of HF. 6
Recent studies have increasingly focused on the prognostic role of NT-proBNP in sepsis. While traditionally linked to sepsis-induced cardiac dysfunction, NT-proBNP is also elevated in noncardiac, critically ill patients, with higher levels seen in non-survivors, 7 possibly related to the synergistic effect of inflammatory mediators. 8 In septic shock, no significant difference was found between lactate and NT-proBNP in predicting in-hospital mortality. 9 Beyond its role as a single biomarker, NT-proBNP, when combined with other parameters, shows enhanced predictive potential for sepsis prognosis.10–12 However, most existing studies have been limited by small sample sizes and primarily focused on short-term outcomes. Our study, utilizing the Medical Information Mart for Intensive Care IV (MIMIC-IV) database, explores the relationship between NT-proBNP and sepsis mortality across multiple time points, providing a more comprehensive understanding of its role as a risk marker for both short-term and long-term.
Methods
Study population
This study is a retrospective observational study based on the MIMIC-IV version 3.1 database, a publicly available resource maintained by the Laboratory for Computational Physiology at the Massachusetts Institute of Technology. 13 The database contains comprehensive health records of over 65,000 ICU admissions at Beth Israel Deaconess Medical Center (BIDMC) in Boston, Massachusetts, from 2008 to 2022. All data in the MIMIC-IV database were approved for research use by the Institutional Review Board of BIDMC, which waived the requirement for informed consent due to the lack of identifiable information and direct patient involvement. The study was conducted in accordance with the Declaration of Helsinki as revised in 2024. The author (Anke Shi) obtained access to the MIMIC-IV database after completing the required training and certification (Certificate ID: 66255831). The reporting of this study conforms to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 14
This study included adult patients diagnosed with sepsis according to the Sepsis 3.0 criteria, which require suspected or confirmed infection and Sequential Organ Failure Assessment (SOFA) score ≥2 points.1,15 Exclusion criteria were as follows: (1) Only the first ICU admission was included for patients with multiple stays; (2) ICU stay of less than 24 h; (3) missing NT-proBNP data within 24 h (Figure 1).
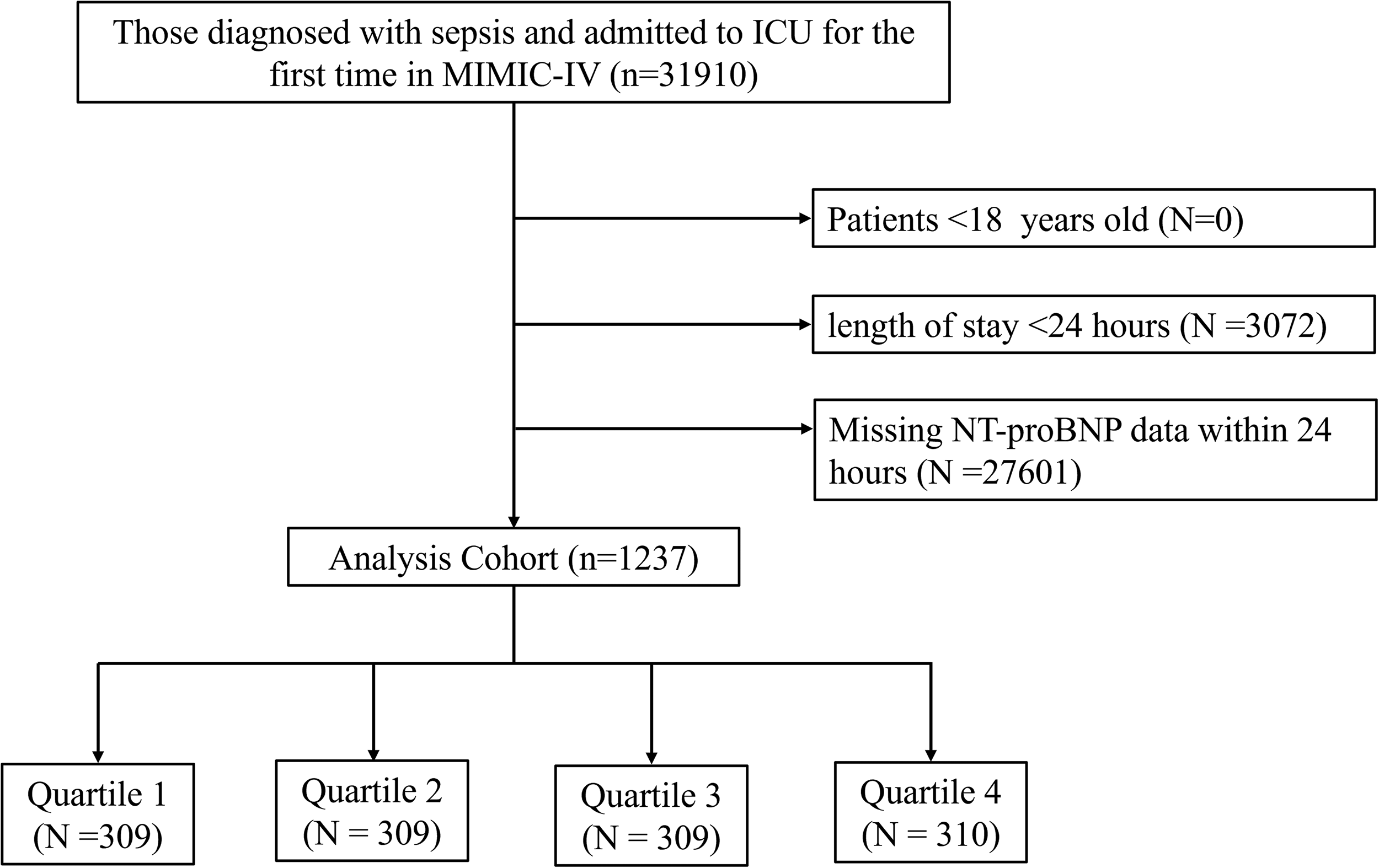
Flowchart for participants from the Medical Information Mart for Intensive Care IV(MIMIC-IV) (v 3.1).
Data collection
Structured query language was used to extract data from the MIMIC-IV (v 3.1) database. Only the first recorded data within 24 h of ICU admission were included. Sepsis patients were identified using the official derived table (mimiciv_derived.sepsis3) in the MIMIC-IV database, assuming a baseline SOFA score of zero. The extracted covariates encompassed six main domains: Demographic information, vital signs, laboratory parameters, disease severity scores, medical interventions, and comorbidities, with detailed descriptions provided in Table 1. Variables with more than 25% missing data were excluded, while missing values for the remaining variables were handled using multiple imputation (Supplemental Table S1).
Characteristics and outcomes of participants categorized by log(NT-proBNP).

All continuous variables are presented as median (IQR) due to non-normal distribution. HR: heart rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; RR: respiratory rate; HB: hemoglobin; PLT: platelet; WBC: white blood cell; PH: potential of hydrogen; INR: international normalized ratio; PT: prothrombin time; PTT: partial thromboplastin time; SOFA: sequential organ failure assessment; CRRT: continuous renal replacement therapy; GC: glucocorticoid; COPD: chronic obstructive pulmonary disease; HF: heart failure; CAD: coronary artery disease; AKI: acute kidney injury; CKD: chronic kidney disease; ACM: all-cause mortality; NT-proBNP: N-terminal pro B-type natriuretic peptide; PaCO2: partial pressure of carbon dioxide.
Clinical outcomes
The primary outcome of this study was 30-day all-cause mortality (ACM), while secondary outcomes included 90-day and 1-year ACM.
Statistical analysis
Continuous variables were summarized as mean ± standard deviation (SD) or median (interquartile range, IQR), depending on their distribution. Group differences were assessed using analysis of variance (ANOVA) for continuous variables or the Kruskal-Wallis test for skewed data. Categorical variables were expressed as frequencies and percentages, and group differences were evaluated using the chi-square test or Fisher's exact test, as appropriate. NT-proBNP was transformed using the natural logarithm to address its skewed distribution, and the study population was divided into quartiles (Q1–Q4) based on the transformed values.
Kaplan–Meier (K-M) survival curves were constructed to estimate survival probabilities across the log-transformed NT-proBNP quartiles. Differences in survival between groups were assessed using the log-rank test. To evaluate the association between log(NT-proBNP) and mortality outcomes, including 30-day, 90-day, and 1-year ACM, multivariable Cox proportional hazards regression models were constructed with adjustments for potential confounders. Model 1 was unadjusted. Model 2 adjusted for demographic variables. Model 3 further adjusted for respiratory rate (RR), temperature, pH, lactate, international normalized ratio (INR), anion gap, SOFA score, continuous renal replacement therapy (CRRT), diuretic, HF, acute kidney injury (AKI), chronic kidney disease (CKD), and malignant cancer. The detailed covariate selection process is described in the Supplementary Material (Table S2–S3). Variance inflation factor (VIF) was calculated to address multicollinearity among the selected confounders. Variables with a VIF greater than 5 were excluded to ensure stability and reduce redundancy. Log(NT-proBNP) was analyzed as both a continuous variable and a categorical variable, with the first quartile (Q1) used as the reference group in the categorical analysis. Results were expressed as hazard ratios (HRs) with 95% confidence intervals (CIs). Additionally, a sensitivity analysis restricted to patients with documented body mass index (BMI) was performed to verify the robustness of the results, with BMI added as a covariate in the multivariable Cox models. Restricted cubic spline (RCS) models were constructed to explore potential non-linear relationships between log(NT-proBNP) and ACM. To ensure consistency with the main analysis, the RCS models adjusted for the same covariates as Cox regression Model 3. Subgroup analyses were performed to explore whether the association between log(NT-proBNP) and ACM varied across different clinical characteristics. Statistical analyses were performed using Python version 3.11.9, R version 4.4.2, and DecisionLink 1.0, which is a platform that integrates multiple programming environments to support data processing, analysis, and machine learning through a visual interface. 16 A two-tailed P-value <0.05 was considered statistically significant.
Results
Baseline characteristics:
A total of 1237 sepsis patients in the ICU were included in the analysis from the MIMIC-IV database, with a median age of 71 years(IQR: 61–81), and 54.41% (n = 673) of them were male. The 30-day, 90-day, and 1-year ACM were 27.41%, 29.99%, and 31.69%, respectively. Based on the log(NT-proBNP) levels within 24 h of ICU admission, subjects were divided into four quartiles: Q1 (log: 2.20–7.16; raw: 9–1291 pg/mL), Q2 (log: 7.17–8.31; raw: 1294–4074 pg/mL), Q3 (log: 8.31–9.34; raw: 4078–11,436 pg/mL), and Q4 (log: 9.35–11.15; raw: 11,491–69,280 pg/mL). The median log(NT-proBNP) for these quartiles were 6.30 (IQR: 5.51–6.82), 7.76 (IQR: 7.45–8.03), 8.86 (IQR: 8.57–9.12), and 10.04 (IQR: 9.68–10.40), respectively.
Patients with higher log(NT-proBNP) levels were more prone to developing comorbidities. Compared to Q1, patients in Q4 had a significantly higher prevalence of HF (29.45% vs 69.35%), AKI (44.01% vs 70.32%), and CKD (10.03% vs 39.68%), alongside higher rates of hypertension, coronary artery disease (CAD), stroke, and diabetes. These patients also demonstrated higher levels of white blood cells (WBC), lactate (1.70 vs 2.00 mmol/L), INR, prothrombin time (PT), partial thromboplastin time (PTT), creatinine (1.00 vs 1.90 mg/dL), urea nitrogen, potassium, anion gap, and SOFA (4.00 vs 6.00), along with lower levels of hemoglobin, partial pressure of carbon dioxide (PaCO2), mean arterial pressure (MAP), and temperature. With increasing log(NT-proBNP) levels, patients were more commonly treated with CRRT (6.47% vs 14.19%) and diuretics (18.77% vs 36.77%), and exhibited a poorer prognosis with significantly higher 30-day (20.06% vs 34.48%), 90-day (22.01% vs 38.39%), and 1-year (22.98% vs 39.68%) ACM rates. The detailed results are presented in Table 1.
Clinical outcomes
The K-M survival analysis was performed to evaluate the ACM rates across various quartiles of log(NT-proBNP) levels. As shown in Figure 2, survival probabilities diminish progressively with increasing log(NT-proBNP) quartile. Patients in Quartile 1 exhibited the highest survival probability, whereas those in Quartile 4 had the lowest at all time points (30-day, 90-day, and 1-year), with a statistically significant difference (log-rank P < 0.001). The correlation between log(NT-proBNP) levels and ACM at 30-day, 90-day, and 1-year was further examined using Cox proportional hazard regression analysis. When log(NT-proBNP) was considered as a continuous variable, it was identified as an independent predictor of 30-day ACM in both the initial adjusted model (HR: 1.13; 95% CI: 1.05–1.22; P = 0.002) and the comprehensive adjusted model (HR: 1.12; 95% CI: 1.03–1.22; P = 0.01). Similar associations were observed for 90-day and 1-year ACM (Table 2).

Kaplan–Meier curves and cumulative incidence of 30-day (A), 90-day (B) and 1-year (C) ACM stratified by log(NT-proBNP) quartiles. NT-proBNP: N-terminal pro B-type natriuretic peptide; ACM: all-cause mortality.
Cox proportional HRs for ACM at 30-day, 90-day, and 1-year.

Model 1: unadjusted; Model 2: adjusted for age and gender; Model 3: adjusted for age, gender, respiratory rate, temperature, lactate, pH, INR, anion gap, SOFA, CRRT, diuretic, HF, AKI, CKD, and malignant cancer. ACM: all-cause mortality; HR: hazard ratio; CI: confidence interval; NT-ProBNP: N-terminal pro B-type natriuretic peptide; HF: heart failure; INR: international normalized ratio; CRRT: continuous renal replacement therapy; CKD: chronic kidney disease; SOFA: sequential organ failure assessment; AKI: acute kidney injury; CKD: chronic kidney disease; PH: potential of hydrogen; INR: international normalized ratio.
When categorizing the log(NT-proBNP) levels as an ordinal variable, with Q1 as the reference, the risk of ACM progressively increased with higher log(NT-proBNP) quartiles across all time points (all P for trend < 0.05). Specifically, for 30-day ACM, only patients in the highest quartile (Q4) exhibited a significantly elevated risk compared to those in Q1 in the fully adjusted model (HR: 1.54;95% CI: 1.08–2.19; P = 0.016), while the intermediate quartiles (Q2 and Q3) showed no statistical significance. Notably, for the longer-term outcomes (90-day and 1-year ACM), the significant association extended to include Q3. Sensitivity analysis restricted to patients with documented BMI (n = 690) yielded results consistent with the primary analysis. After adjusting for BMI and other potential confounders (consistent with Model 3), log(NT-proBNP) levels remained significantly associated with ACM at all time points. Specifically, except for the Q2 group in the 30-day analysis (P = 0.059), all other groups in Model 3 across 30-day, 90-day, and 1-year time points showed significant associations with increased mortality risk, and the trend remained significant (all P for trend < 0.05, Supplemental Table S4). Consistent with these findings, RCS analysis confirmed a linear association between log(NT-proBNP) and ACM at all time points (all P for nonlinearity >0.05, Figure 3).

Restricted cubic spline curve for 30-day (A), 90-day (B) and 1-year (C) ACM. CI: confidence Interval; ACM: all-cause mortality.
Subgroup analysis
The strength of the association between log(NT-proBNP) and ACM was further assessed through subgroup analyses, which included age, gender, the presence of HF, AKI, and CKD (Figure. 4). Overall, no significant interaction was detected between log(NT-proBNP) and any subgroup variable (all P for interaction > 0.05). For 30-day ACM, more pronounced associations were noted in patients of all ages (≤65 years: HR:1.29; 95% CI:1.11–1.49; P = 0.001; >65 years: HR: 1.14; 95% CI:1.03–1.25; P = 0.009), males (HR: 1.18; 95% CI: 1.06–1.31; P = 0.002), and individuals with HF (HR: 1.18; 95% CI: 1.06–1.31; P = 0.002), with AKI (HR: 1.25; 95% CI: 1.13–1.38; P < 0.001), and without CKD (HR: 1.18; 95% CI: 1.08–1.29; P < 0.001).
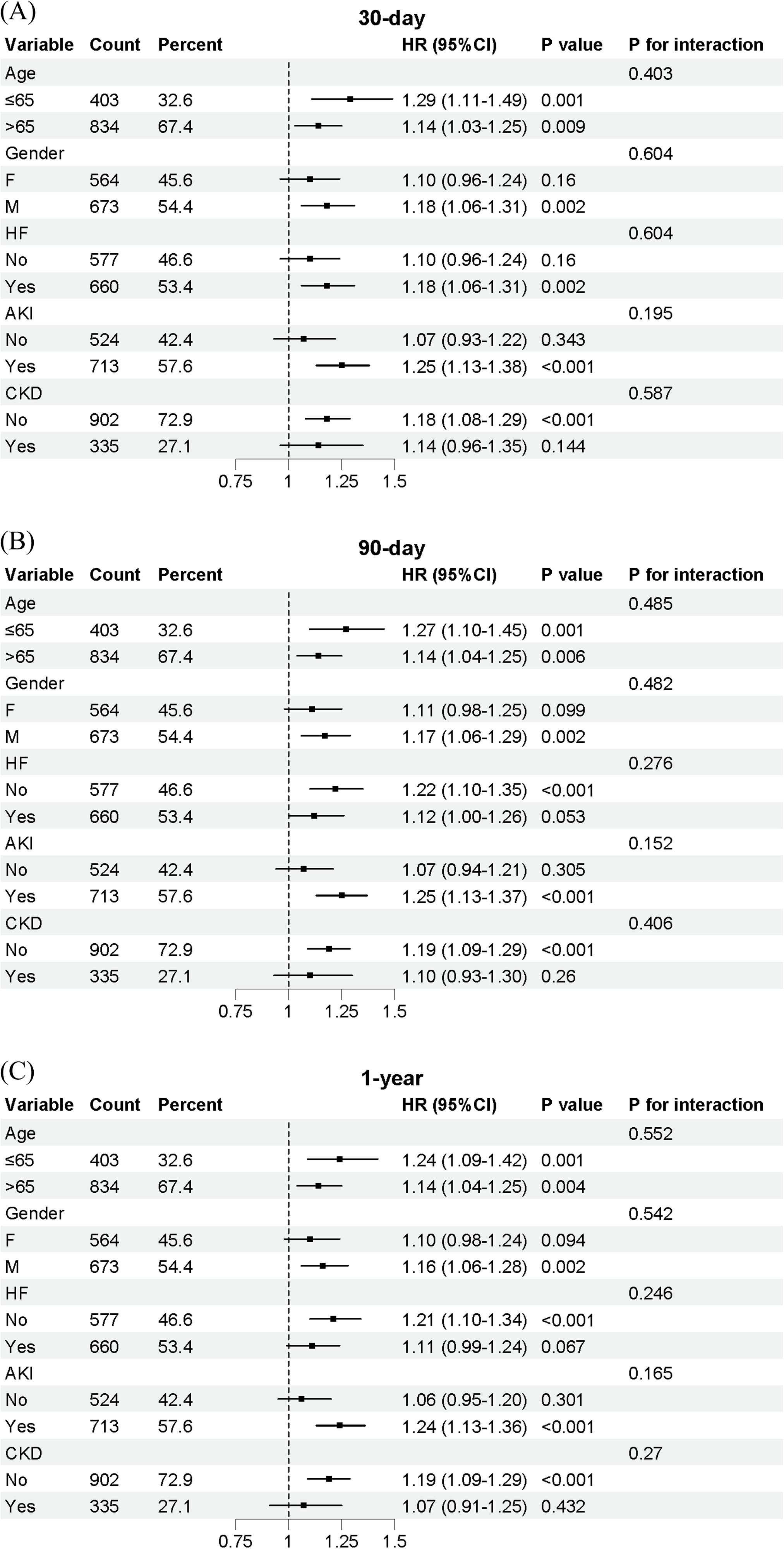
Forest plots of HRs for 30-day (A), 90-day (B) and 1-year (C) ACM in different subgroups. F: female; M: male; HF: heart failure; AKI: acute kidney injury; CKD: chronic kidney disease; HR: hazard ratio; CI: confidence interval; ACM: all-cause mortality.
For 90-day and 1-year ACM, the association became significant in patients without HF(90-day HR: 1.22; 95% CI: 1.10–1.35; P < 0.001), while other subgroups exhibited a similar pattern.
Discussion
In this study, we investigated the relationship between log(NT-proBNP) levels and both short-term and long-term ACM in critically ill sepsis patients using data from the MIMIC-IV database. Our findings demonstrate that log(NT-proBNP) is an independent associated with 30-day, 90-day, and 1-year ACM in sepsis patients, with a linear relationship observed between increasing log(NT-proBNP) levels and progressively higher mortality risk at each time point. Incorporating various confounders, higher log(NT-proBNP) levels were consistently associated with worse prognosis, and this relationship remained robust even after stratification by subgroups, further supporting log(NT-proBNP) as a reliable risk biomarker in sepsis.
While the association between NT-proBNP and mortality is well-established in HF,17–19 this relationship extends to non-cardiac critical illnesses, including stroke, AKI, and severe respiratory infections.20–24 Similarly, sepsis, as a severe infectious disease, is also likely to exhibit a significant association between NT-proBNP levels and mortality. Indeed, since Witthaut first reported significantly elevated BNP levels in septic shock, 25 this relationship has been widely explored. Brueckmann et al. demonstrated that in ICU patients with sepsis, elevated levels (>1400 pmol/L) were associated with a nearly 4-fold increase in mortality risk. 26 More recently, studies in sepsis patients showed that NT-proBNP had comparable predictive accuracy to lactate for in-hospital mortality. 9 However, most studies focus on short-term prognosis, though a few have explored long-term prognosis. A single-center study including 259 septic patients without HF found that BNP was a strong predictor of in-hospital mortality, 90-day, and 60-month mortality in sepsis patients. 27 Custodero et al. 28 found that higher levels of NT-proBNP at 24 h after sepsis onset were associated with lower short physical performance battery test score at 12 months and lower hand grip strength at 6-month and 12-month follow-up, despite this conclusion being frequently questioned due to the insufficient consideration of renal issues. Addressing these gaps, our study confirms a consistent linear association between baseline log(NT-proBNP) and mortality extending up to one year. After adjusting for confounders including heart and kidney function, each unit increase in log(NT-proBNP) was associated with a 12%, 12%, and 11% increase in ACM risk at 30 days, 90 days, and 1 year, respectively. At the same time, patients in the highest log(NT-proBNP) level (Q4) had a mortality risk 1.54, 1.62, and 1.61 times higher than those in the lowest level (Q1) at the three time points, which is consistent with previous studies.
The precise mechanisms linking NT-proBNP to sepsis mortality remain incompletely understood. Myocardial stress seems to be the most evident mechanism contributing to its elevation. Although sepsis-induced myocardial dysfunction (SIMD) lacks a standardized definition, it often manifests as biventricular systolic and diastolic dysfunction, along with a poor response to fluid resuscitation and catecholamines. This results in ventricular dilation and wall stress, stimulating NT-proBNP release. 29 Studies indicate that left ventricular dysfunction occurs in 30%–60% of sepsis patients.30–32 Charpentier et al. 33 were the first to demonstrate that BNP plasma levels are increased in patients with sepsis-related myocardial dysfunction, and that high BNP levels appear to carry a poor prognostic value in septic patients. Roch et al. found that the left ventricular stroke work index correlates with NT-proBNP levels in patients with septic shock. 34 A recent meta-analysis showed that BNP and NT-proBNP levels were higher in the SIMD group. NT-proBNP > 3000 pg/ml was an independent risk factor for SIMD, with moderate diagnostic accuracy (AUC = 0.81). 35 However, a prospective observational study found that BNP levels were elevated in septic patients without evidence of systolic dysfunction, and were positively correlated with CRP levels. 36 This suggests that myocardial stress may not fully explain the elevation of NT-proBNP in septic patients, and that inflammation itself may also play an important role. Lipopolysaccharide (LPS) enhances BNP mRNA expression via a CD14-mediated increase in p38 MAP kinase and GATA sequence in the BNP promoter. 37 Fish-Trotter et al. 38 demonstrated through three experiments that, in atherosclerosis patients, each 1-unit increase in the natural log of IL-6 was linked to a 16% rise in NT-proBNP. LPS elevated NT-proBNP in healthy individuals, and acute inflammation in hospitalized patients was associated with a 36% increase in natriuretic peptides (NPs). Another mechanism that cannot be overlooked is kidney function. The kidneys are the main organs responsible for NT-proBNP excretion, and its levels increase exponentially as glomerular filtration rate declines. 39 A recent study of 187,888 adult ICU patients found that sepsis-associated AKI (SA-AKI) occurred in nearly half of sepsis patients and one in six ICU admissions. SA-AKI was linked to significantly higher mortality compared to sepsis or AKI alone. 40 Varpula et al. 8 suggested that acute cardiac load at admission contributes to the elevated NT-proBNP levels, but later renal failure is the primary confounding factor. Additionally, the secretion of NP is regulated by sex hormones, with estrogen promoting and testosterone inhibiting their release.41,42 In septic patients, estrogen levels are significantly elevated, particularly in non-survivors, and the median plasma concentration of NT-proBNP in females is 93.48% higher than in males. However, no significant difference in 30-day mortality was found between genders.43,44 In our study, based on the consideration of the above mechanisms, we focused on analyzing key factors such as age, gender, heart function (e.g. HF), and kidney function (e.g. AKI and CKD) in our subgroup analysis. The analysis showed stable trends across these factors, and no significant interactions were detected between log(NT-proBNP) and any subgroup variable (all P for interaction > 0.05). This suggests that the association between NT-proBNP and ACM at all three time points remains robust across different clinical phenotypes, regardless of the presence of comorbidities.
However, we must acknowledge several limitations in our study. First, due to the retrospective observational design of this study, we can only demonstrate an association rather than establish causality between NT-proBNP levels and mortality. Although we performed multivariable adjustment to control for potential confounders, unmeasured or unknown confounders may still exist. Second, selection bias is unavoidable because NT-proBNP measurements were likely ordered based on clinical suspicion of cardiac dysfunction or concomitant HF, rather than as a routine screening for all septic patients. Third, a substantial proportion of patients in the MIMIC-IV database lacked BMI data, which is a known physiological determinant of NT-proBNP levels. Although our sensitivity analysis restricted to patients with documented BMI confirmed that the prognostic value of NT-proBNP remained robust after adjustment for BMI, the potential for selection bias due to missing data cannot be entirely ruled out. Fourth, although NT-proBNP is relatively stable without significant intra-day or inter-day variation, relying solely on a single baseline measurement fails to capture its dynamic trajectory throughout the progression of sepsis. Critical pathophysiological events—such as SIMD, inflammatory cytokine storms, and AKI—may significantly alter NT-proBNP levels over time. Last, the study relies on the single-center MIMIC-IV database without external validation, and its generalizability may be influenced by geographic heterogeneity in sepsis management practices and ethnic differences in NT-proBNP metabolism.
Conclusion
In conclusion, our study found that elevated baseline NT-proBNP levels at ICU admission are closely associated with higher ACM at 30 days, 90 days, and 1 year in critically ill sepsis patients. This suggests that NT-proBNP may serve as a valuable tool to aid in identifying high-risk individuals and guiding risk stratification. However, future prospective and multicenter studies with dynamic monitoring of NT-proBNP are needed to confirm these findings.
Supplemental Material
sj-docx-1-sci-10.1177_00368504261425535 - Supplemental material for Association between N-terminal pro B-type natriuretic peptide and short- and long-term all-cause mortality in critically ill patients with sepsis: A retrospective study based on the Medical Information Mart for Intensive Care IV database
Supplemental material, sj-docx-1-sci-10.1177_00368504261425535 for Association between N-terminal pro B-type natriuretic peptide and short- and long-term all-cause mortality in critically ill patients with sepsis: A retrospective study based on the Medical Information Mart for Intensive Care IV database by Anke Shi, Haotian Lu, Jing Zhao, Mingshuai Ai, Jieqiong Yu, Tianpeng Hu and Shengtao Yan in Science Progress
Supplemental Material
sj-pdf-2-sci-10.1177_00368504261425535 - Supplemental material for Association between N-terminal pro B-type natriuretic peptide and short- and long-term all-cause mortality in critically ill patients with sepsis: A retrospective study based on the Medical Information Mart for Intensive Care IV database
Supplemental material, sj-pdf-2-sci-10.1177_00368504261425535 for Association between N-terminal pro B-type natriuretic peptide and short- and long-term all-cause mortality in critically ill patients with sepsis: A retrospective study based on the Medical Information Mart for Intensive Care IV database by Anke Shi, Haotian Lu, Jing Zhao, Mingshuai Ai, Jieqiong Yu, Tianpeng Hu and Shengtao Yan in Science Progress
Footnotes
Author contributions
Anke Shi and Haotian Lu designed the study. Jing Zhao, Mingshuai Ai, and Jieqiong Yu extracted, collected, and analyzed the data. Tianpeng Hu and Jieqiong Yu prepared tables and figures. Anke Shi reviewed the results, interpreted the data, and wrote the manuscript. Shengtao Yan proofread and revised the manuscript. All authors have contributed equally to the manuscript and approved the submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (grant number 2021ZD0200200).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Generative AI and AI-assisted technologies in the writing process
During the preparation of this work, the authors used ChatGPT (OpenAI) to improve the clarity, grammar, and readability of the manuscript. After using this tool, the authors carefully reviewed and edited the content as needed, and take full responsibility for the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.