
Abstract
Background
Candidemia is the most common invasive fungal disease in intensive care units (ICUs).
Objective
We aimed to investigate cases of candidemia infection developing in the ICU and factors associated with mortality due to this infection.
Materials and Methods
This is a retrospective study including patients admitted to a tertiary university hospital ICU between January 2012 and December 2020. Patients over 18 years of age who had candida growth in at least one blood culture taken from central or peripheral samples (>48 h after admission to the ICU) without concurrent growth were evaluated.
Results
The study group consisted of 136 patients with candida. Eighty-seven (63.97%) patients were male, with a median age of 69.5 (59–76.5) years. The 7-day mortality rate was 35.29%, while the 30-day mortality rate was 69.11%. As a result of multiple logistic regression analysis, after adjusting for age and malignancy, high APACHE II score and low platelet-lymphocyte ratio (PLR) - were found to be significant factors in predicting both 7-day and 30-day mortality.
Conclusion
In this study, PLR and APACHE II scores were shown to be independent predictors of mortality in patients with candidemia in the ICU.
Introduction
Candidemia is the most common invasive fungal disease in intensive care units (ICUs) and is considered to be the bloodstream pathogen with the highest mortality.1, 2 Risk factors for candidemia have been identified in several studies and can be listed as prolonged stay in ICU, use of immunosuppressive drugs, invasive interventions, and use of broad-spectrum antibiotics. In addition, as these risks demonstrate an increasing trend in medicine, the frequency of candidemia has also increased gradually during the last two decades and has become an important health problem in modern medicine.3,4
Many of the predisposing factors for candidemia are very common in critically-ill patients admitted to the ICU. 5 In addition, the low sensitivity of diagnostic tools and delayed results prevent rapid detection and treatment of this infection. 6 Therefore, early and targeted treatment in candidemia is very important in terms of mortality and prognosis. 7 Although blood cultures are accepted as the gold standard for the diagnosis of candidemia, the most important disadvantage of this method is that the results are often delayed. 8 For this reason, investigation of the role of various laboratory parameters in the diagnosis of candidemia has recently gained interest. 9 In addition, the relationship of haematological parameters such as neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) with prognosis and mortality in some diseases have yielded interesting results.10,11 However, the relationship between these indicators and mortality from candidemia has not been adequately discussed, especially in ICU patients with candidemia.
With a better understanding of the relationship between candidemia and haematological parameters, important clues can be obtained both in the prevention of its development and in the early treatment of candidemia, which has become an important problem, especially in ICUs. Thus, it is evident that the identification of possible relationships in this context will also be effective in reducing mortality and morbidity in patients suffering from candidemia. In this study, we investigated cases of candidemia in the ICU and factors associated with mortality.
Methods
This study is a retrospective cohort examining patients admitted to the ICU at Istanbul Medipol University Hospital between January 2012 and December 2020. Necessary permissions were obtained from the Clinical Research Ethics Committee of local Institutional Review Board for the study.
Inclusion criteria
Patients over 18 years of age who had candida growth in at least one blood culture obtained from central or peripheral sites (>48 h after admission to the ICU) without concurrent growth were included. A total of 136 samples fulfilling these criteria were identified during the study period. If the same patient had more than one episode of candidemia during the study period, only the first episode of candidemia infection was included.
Exclusion criteria
Patients who were under the age of 18, had suspected candidemia before being admitted to the ICU, and subjects who died within 48 h of ICU admittance or were transferred to a different hospital were not included in the study. Accordingly, a final total of 136 patients were included in the analyzes.
Measurements
Yeast production detected in blood cultures was typed with VITEK 2 Compact System (BioMerieux, France) automated identification system. After positive blood culture was detected, blood samples were obtained for laboratory analyzes. A complete blood count (CBC) was performed in the hematology laboratory of the same hospital with the Horiba ABX Pentra DF 120 automatic analyzer.
Neutrophil-to-lymphocyte ratio (NLR) was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count. Platelet-to-lymphocyte ratio (PLR) was calculated by dividing the platelet count by the lymphocyte count. Lymphocyte-to-monocyte ratio (LMR) was calculated by dividing lymphocyte count by monocyte count. The prognostic nutritional index (PNI) is associated with serum albumin level and the total lymphocyte count and was calculated by the formula: PNI = 10 × serum albumin concentration (g/dL) + 0.005 × total lymphocyte count (mm3). Systemic inflammation index (SII) was calculated using the following formula: platelet × (neutrophil/lymphocyte).
All clinical scores were recorded on the day of admission to the ICU. The Modified Glasgow Prognostic Score (mGPS) provides scores based on C-reactive protein (CRP) (CRP > 10 mg/L = 1 point) and albumin (albumin < 3.5 g/dL = 1 point) levels. Cases are classified as low risk (0 points), medium risk (1 point) and high risk (2 points) according to mGPS scores.12,13 The Acute Physiology and Chronic Health Evaluation (APACHE) II is a parameter calculated based on the clinical and laboratory characteristics of the cases, and it is well established that higher scores indicate unfavorable outcomes. 14
After recording all the above data, we identified 7-day and 30-day mortality status and evaluated associated factors.
Statistical analysis
All analyzes were subject to a significance threshold of p ≤ 0.05 and were performed on SPSS v25 (SPSS Inc., Chicago, IL, USA). For the normality check, histograms and Q-Q plots were used. Data are given as mean ± standard deviation or median (interquartile range; IQR) for continuous variables according to the normality of distribution, and as frequency (percentage) for categorical variables. According to distribution normality/non-normality, the independent samples t-test or the Mann-Whitney U test, respectively, were used for comparison of continuous variables. Categorical variable analyzes employed chi-square tests or Fisher's exact tests. The prediction performance of the variables was assessed by using Receiver Operating Characteristic (ROC) curve analysis. Multiple logistic regression analysis (forward conditional method) was performed to determine the best predictive factors of mortality.
Results
The study group consisted of 136 patients with candida. Eighty-seven (63.97%) patients were male and their median age (IQR) was 69.5 (59–76.5) years. While 7-day mortality rate was 35.29%, 30-day mortality rate was 69.11%. Factors associated with 7-day mortality were: malignancy (p = 0.001), high APACHE II score (p = 0.032), low platelet count (p = 0.002), low eosinophil count (p = 0.016), low PLR (p = 0.001) and low SII (p = 0.038) (Table 1)
Summary of patients characteristics with regard to 7-days mortality.
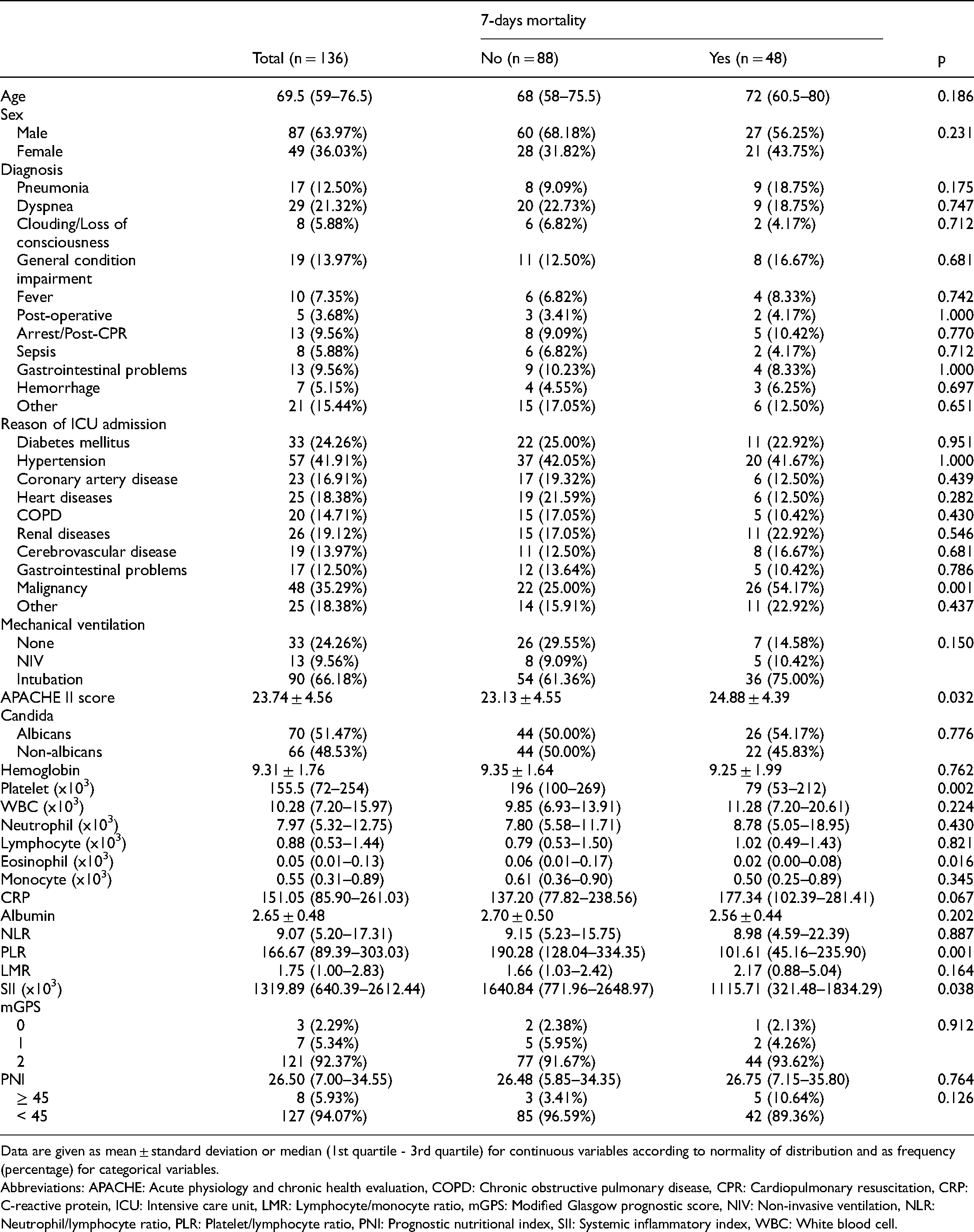
Data are given as mean ± standard deviation or median (1st quartile - 3rd quartile) for continuous variables according to normality of distribution and as frequency (percentage) for categorical variables.
Abbreviations: APACHE: Acute physiology and chronic health evaluation, COPD: Chronic obstructive pulmonary disease, CPR: Cardiopulmonary resuscitation, CRP: C-reactive protein, ICU: Intensive care unit, LMR: Lymphocyte/monocyte ratio, mGPS: Modified Glasgow prognostic score, NIV: Non-invasive ventilation, NLR: Neutrophil/lymphocyte ratio, PLR: Platelet/lymphocyte ratio, PNI: Prognostic nutritional index, SII: Systemic inflammatory index, WBC: White blood cell.
When the performances of various variables in predicting 7-day mortality were evaluated, it was found that high APACHE II score (p = 0.008), low PLR (p = 0.001) and low SII (p = 0.038) were significant. Among these variables, PLR was found to predict 7-day mortality with the highest accuracy (73.68%) (Table 2,Figure 1

ROC curve of the variables to predict 7-days mortality.
Performance of the variables to predict 7-days mortality.
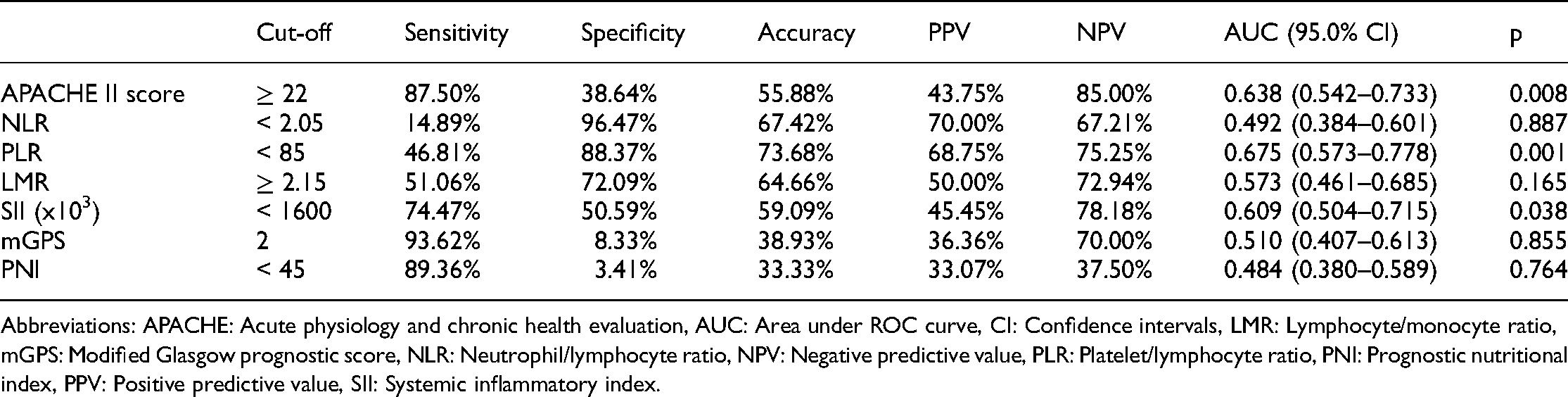
Abbreviations: APACHE: Acute physiology and chronic health evaluation, AUC: Area under ROC curve, CI: Confidence intervals, LMR: Lymphocyte/monocyte ratio, mGPS: Modified Glasgow prognostic score, NLR: Neutrophil/lymphocyte ratio, NPV: Negative predictive value, PLR: Platelet/lymphocyte ratio, PNI: Prognostic nutritional index, PPV: Positive predictive value, SII: Systemic inflammatory index.
We performed multiple logistic regression to determine significant predictive factors of 7-day mortality. We found the presence of malignancy, high APACHE II score and low PLR were significant factors. Patients with a high APACHE II score (≥22) had a 7.127-fold higher risk of death than those with a lower score (OR: 7.127, 95% CI: 2.188–23.217; p = 0.001). Patients with low PLR (<85) had a 9.328-fold higher risk of death than those with higher PLR (OR: 9.328, 95% CI: 3.303–26.344, p < 0.001). Other variables included in the model, age (p = 0.681), sex (p = 0.727), mechanical ventilation (p = 0.978), type of candida (p = 0.602), NLR (p = 0.222), LMR (p = 0.565), SII (p = 0.583), mGPS (p = 0.741) and PNI score (p = 0.718) were found to be non-significant (Table 3).
Significant predictive factors of the 7-days mortality, multiple logistic regression analysis.

Dependent Variable: 7-days mortality; Nagelkerke R2 = 0.413; Correct prediction = 78.20%
Abbreviations: APACHE: Acute physiology and chronic health evaluation, CI: Confidence intervals, PLR: Platelet/lymphocyte ratio.
When the factors associated with 30-day mortality were analyzed, significant relationships were found between 30-day mortality and malignancy (p = 0.014), mechanical ventilation (p = 0.038), high APACHE II score (p < 0.001), high CRP (p = 0.049), and low albumin (p = 0.025) There was no significant difference between Candida species (albicans vs non-albicans) in terms of 7-day and 30-day mortality rates (p = 0.776, p = 0.247, respectively) (Table 4).
Summary of patients characteristics with regard to 30-days mortality.

Data are given as mean ± standard deviation or median (1st quartile - 3rd quartile) for continuous variables according to normality of distribution and as frequency (percentage) for categorical variables.
Abbreviations: APACHE: Acute physiology and chronic health evaluation, COPD: Chronic obstructive pulmonary disease, CPR: Cardiopulmonary resuscitation, CRP: C-reactive protein, ICU: Intensive care unit, LMR: Lymphocyte/monocyte ratio, mGPS: Modified Glasgow prognostic score, NIV: Non-invasive ventilation, NLR: Neutrophil/lymphocyte ratio, PLR: Platelet/lymphocyte ratio, PNI: Prognostic nutritional index, SII: Systemic inflammatory index, WBC: White blood cell; NIMV: Noninvasive mechanical ventilation.
The performance of the variables in predicting 30-day mortality was evaluated. Among the variables, only the APACHE II score was found to significantly predict 30-day mortality with an accuracy of 77.94%. No significant value was found in terms of other variables (Table 5,Figure 2).

ROC curve of the variables to predict 30-days mortality.
Performance of the variables to predict 30-days mortality.

Abbreviations: APACHE: Acute physiology and chronic health evaluation, AUC: Area under ROC curve, CI: Confidence intervals, LMR: Lymphocyte/monocyte ratio, mGPS: Modified Glasgow prognostic score, NLR: Neutrophil/lymphocyte ratio, NPV: Negative predictive value, PLR: Platelet/lymphocyte ratio, PNI: Prognostic nutritional index, PPV: Positive predictive value, SII: Systemic inflammatory index.
We performed multiple logistic regression to determine significant predictive factors of 30-day mortality. We found age, malignancy presence, high APACHE II score and low PLR as significant factors. Patients with a high APACHE II score (≥22) had 31.699-fold higher risk of death than those with a lower score (OR: 31.699, 95% CI: 8.394–119.709; p < 0.001). Patients with low PLR (<105) had 10.467-fold higher risk of death than those with higher PLR (OR: 10.467, 95% CI: 2.540–43.123; p = 0.001). Other variables included in the model, sex (p = 0.767), mechanical ventilation (p = 0.631), type of candida (p = 0.156), NLR (p = 0.569), LMR (p = 0.697), SII (p = 0.393), mGPS (p = 0.103) and PNI score (p = 0.237) were found to be non-significant (Table 6).
Significant predictive factors of the 30-days mortality, multiple logistic regression analysis.

Dependent Variable: 30-days mortality; Nagelkerke R2 = 0.527; Correct prediction = 79.70%
Abbreviations: APACHE: Acute physiology and chronic health evaluation, CI: Confidence intervals, PLR: Platelet/lymphocyte ratio.
Discussion
According to the results of our study, 7-day mortality rate was 35.2% and the 30-day mortality rate was 69.1% in ICU patients that developed candidemia. We also found a high APACHE II score and low PLR to be significant independent risk factors for both 7-day and 30-day mortality in ICU patients with candida infection –with adjustment for age and malignancy by inclusion in the models.
Prior studies show that 33–55% of all candidemia infections occur in the ICU and 5–71% of these cases are reported to result in mortality.15,16 In a multicentre study evaluating candida infections in 23 ICUs in Europe, crude 30-day mortality was reported to be 42%. 17 Other studies estimating attributable mortality rates show values between 40–50%.18–20 In our study, the 30-day mortality rate was found to be 69.1%, which was considerably higher compared to the literature. However, our results may have been affected because our study was conducted in a tertiary ICU, and there was no evaluation of whether the deaths were due to candidiasis or worsening of the underlying disease; thus, attributable mortality rates could not be calculated.
In different studies, many factors associated with mortality and prognosis in candidemia have been identified. These factors include the use of mechanical ventilation, hypoproteinaemia, high APACHE II score, delay in catheter removal, and inadequate antifungal therapy.21–24 In addition, a recent study reported that the cumulative number of related risk factors is the most useful variable in predicting hospital death due to candidemia among intensive care patients. 25 In our study, factors associated with both 7-day and 30-day mortality were evaluated. Accordingly, 7-day mortality was found to be associated with (univariate analysis): malignancy, high APACHE II score, platelet level, eosinophil level, low PLR level and SII level. The factors that were significantly associated with 30-day mortality (again, univariate results) were malignancy, mechanical ventilation, high APACHE II score, high CRP, and low albumin. However, with further analysis after adjusting for age and malignancy via regression models, high APACHE II scores and low PLR levels were found to be independent risk factors for both 7-day mortality and 30-day mortality.
The APACHE II score, which is widely used in the ICU and is one of the important tools in showing prognosis, has been shown to accurately measure the severity of the disease and is also strongly associated with mortality in critically-ill patients. 26 In addition, it has been frequently emphasized that a high APACHE II score may be a predictor of mortality in patients with candida infection,16,27,28 similar to our findings. In a recent study, it was reported that an APACHE II score above 20 was an independent risk factor for mortality in patients with candidiasis. 29 In our study, patients with a high APACHE II score (≥22) had a 7.1-fold higher risk of death in terms of 7-day mortality and a 31.6-fold higher risk of death in terms of 30-day mortality, in line with the literature. In addition, it was found that the APACHE II score significantly predicted 30-day mortality with an accuracy of 77.94%.
Studies have reported that PLR, which is a haematological index reflecting inflammation and thrombosis, may provide prognostic efficacy in various cancers and heart-lung diseases.30–33 In addition, in a study, it was reported that PLR value was associated with increased mortality in sepsis patients. 34 In a recent study, Zhai et al. reported that PLR is an independent predictor of mortality in patients hospitalized in the ICU. 35 Contrary to these reports, in a study evaluating bloodstream infections, including candida, it was suggested that PLR level was not associated with clinical outcomes. 36 In our study, however, it was found that low PLR level was independently associated with increased 7-day mortality (9.3 fold) and 30-day mortality (10.4 fold). In addition, PLR levels was found to predict 7-day mortality with the highest accuracy (73.68%). We thought that this result was mainly due to the decrease in platelet level. Consistent with our findings, recent studies have reported that newly developing thrombocytopenia is associated with mortality in candidemia cases.37,38 In the literature, it can be said that the relationship between PLR and mortality in candidemia cases has been examined in very few studies, and the fact that our results indicate greater accuracy compared to APACHE II score is crucial and warrants further research on this topic. New studies are needed to better understand the relationship between haematological parameters and candida infections, and how these factors are associated with mortality and prognosis.
This study had some limitations. First, the study design had inherent disadvantages due to its retrospective nature. Second, we did not distinguish whether death was due to candidemia or the underlying disease, as it is difficult to determine the exact cause of death in critically ill patients. In relation, previous studies have reported that culture sampling experience may affect the outcomes. 39 Although all cultures were obtained in a standardized fashion, possible differences in operator experience may have caused limited but unavoidable variations in culture positivity for both candida and other agents. The fact that the study was single-centred can be noted as another limitation. In addition, although there have been many studies examining candidemia and the factors affecting mortality, one of the strengths of our study is that it is one of the few studies examining the relationships between CBC-derived haematological parameters and mortality.
Conclusions
In this study, it was observed that low PLR level and high APACHE II score increased both 7-day and 30-day mortality in patients who developed candidemia in the ICU. These two parameters were independent predictors of mortality, in addition to malignancy (7-day and 30-day) and age (30-day). In clinical practice, it may be useful to consider APACHE II and PLR levels in cases with candidemia in the ICU, and it appears that PLR may in fact be more accurate for prognostic assessment in the shorter term. Since patients with candidemia have greater mortality in clinical practice, empirical antifungal therapy may be considered for patients with high APACHE II score, low PLR or thrombocytopenia at ICU admission in order to reduce mortality. The relationship between CBC-derived haematological parameters and candidemia can be examined in more detail with future prospective, multicentre studies that include more cases.
Footnotes
Authors' contributions
All authors analyzed, interpreted the patient data, and were major contributors in writing the manuscript. All authors read and approved the final manuscript.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request
Consent for publication
Informed consent was not obtained from the patients because the study was a retrospective study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study has been conducted by the principles of the Helsinki Declaration and approved by the local Institutional Review Board.