
Abstract
Objectives
Polypharmacy, the concurrent use of multiple medications, presents significant challenges and risks in modern healthcare systems, particularly among older individuals and those with chronic diseases. This study aimed to investigate the prevalence and determinants of potential drug–drug interactions (pDDIs) among older adults at Jerusalem, Gaza Strip, and the West Bank of Palestine. This study serves as a baseline assessment before the October 2023 Palestine crisis, which led to extensive forced displacement.
Methods
This cross-sectional study examined the prescribed medications for 403 participants, conducted between May 2023 and August 2023, 2 months prior to the invasion of Gaza. This study served as a baseline evaluation of the potential pDDIs before the 7 October 2023 of Palestine crisis. Participants recruited using simple random sampling technique from medical records’ lists of patients. They were interviewed at various pharmacies and hospitals across Jerusalem, the Gaza Strip, and the West Bank of Palestine using an online questionnaire created via Google Forms. Descriptive, Univariate and multivariate analyses, and Chi-square tests were carried-out by SPSS v21.
Results
The study revealed a high prevalence of pDDIs among the Palestinian population, with a substantial proportion of participants experiencing moderate to major interactions. Participants receiving a higher number of medications were significantly more likely to experience major pDDIs. Additionally, marital status was a significant factor associated with major pDDIs, with married individuals being more likely to experience major interactions compared to non-married individuals. Regional differences were also observed, with participants residing in the northern region of the West Bank more likely to experience moderate pDDIs. Moreover, participants diagnosed with dyslipidemia and diabetes mellitus were significantly more prone to moderate pDDIs.
Conclusions
These findings emphasize the interaction of clinical and demographic factors in influencing the risk of pDDIs among participant patients in Palestine. Healthcare providers should consider these factors when prescribing medications and designing interventions to reduce the risks associated with polypharmacy.
Introduction
The 2023 Palestine crisis has significantly exacerbated the on-going humanitarian crisis in Palestine. The conflict has seen vast destruction of the housing and healthcare infrastructure. The situation is especially critical for older adults in the Gaza Strip as they faced various concomitant health conditions such as infection, COVID-19, and existing non-communicable diseases.1–3 In modern healthcare systems, managing chronic illnesses and complex medical conditions often requires administering multiple medications simultaneously, a practice known as polypharmacy. 4 Polypharmacy is becoming increasingly common, particularly among older adults and those with chronic diseases. 5 However, while the use of multiple medications can be beneficial, it also carries risks. One significant risk is drug–drug interactions (DDIs), where two or more medications interact; potentially altering their effects and causing harm. 6 These interactions can lead to side effects, reduced treatment efficacy, hospitalizations, and even death, posing challenges for both patients and healthcare systems.
Although there has been less research on DDIs in Middle Eastern countries compared to some Western nations, several studies have explored the prevalence of potential DDIs (pDDIs) and the factors contributing to them in the Arab region. For example, a study by Nussair et al. in 2020 examined the prevalence of pDDIs among hospitalized participant patients in Jordan. 7 The study found that pDDIs were common, particularly among patients with comorbidities who were taking multiple medications. This highlighted the importance of healthcare providers carefully reviewing patients’ medications to reduce the risk of harmful interactions.
Similarly, a study by Al-Asiri and Al-Arifi in 2011 investigated the prevalence of pDDIs among participants with chronic diseases in Saudi Arabia. 8 They found a significant number of pDDIs, especially among participants with heart disease and diabetes, emphasizing the importance of regularly monitoring patients’ medications to ensure safety. To the best of our knowledge, there is a lack of studies and information regarding the prevalence of pDDIs in Palestine, as well as the factors associated with this risk. Polypharmacy is particularly common among older adults, who often have multiple health conditions requiring ongoing treatment. 2
It is crucial to understand the unique challenges associated with the use of multiple medications in this population. Accordingly, this baseline study, conducted right before the October 2023 crisis, aimed to identify socio-demographic and clinical factors associated with potential pDDIs in Palestine. These findings may serve as a pre-crisis reference point for monitoring future changes in medication safety and polypharmacy patterns in Palestine. Additionally, this study investigated clinical factors that may influence the risk of pDDIs, such as the presence of comorbidities, the number of medications an individual is taking, and their history of previous pDDIs. By identifying these factors, the findings of this study can inform strategies aimed at reducing the risk of pDDIs in Palestine further.
Methods
Study design
This was a cross-sectional baseline study conducted in community pharmacies and outpatient clinics across three main regions of Palestine: the West Bank (North, Middle, South), the Gaza Strip, and Jerusalem and 1948 Lands. Data collection occurred between May and August 2023. The reporting of this study conforms to the STROBE guidelines. 9
Data collection
This study involved examining prescribed medications for participants who were interviewed at various pharmacies and hospitals located in Jerusalem, the Gaza Strip, and the West Bank of Palestine. Medication information was primarily sourced from current prescription records presented by the patients at the time of the interview, supplemented by patient self-report during a structured interview. Participants were selected using a simple random sampling method. The identities of the participants were concealed to maintain the confidentiality of the data.
During the interviews, the researchers collected data on factors related to the likelihood of pDDIs and/or polypharmacy. These factors included patients’ socio-demographic and clinical characteristics, such as educational level, number of sons/daughters (i.e. whether the patient lived alone or not), number of medications taken daily, and the presence of cardiovascular (CV) and non-CV diseases. To assess the severity of pDDIs, the researchers employed a classification system based on sources such as Drugs.com (https://www.drugs.com/drug_interactions.html) and Lexicomp Online (https://online.lexi.com).
Data variables and definitions
This classification categorized pDDIs into three distinct severity levels: 1) Minor pDDIs with minimal clinical significance, equivalent to Lexicomp category B. These represent pDDIs with a limited impact on patient health; 2) Moderate PDDIs, holding moderate clinical significance, aligning with Lexicomp category C. These denote interactions that may moderately affect a patient's health and should be carefully considered; and 3) Major pDDIs, interactions of high clinical significance that are generally recommended for avoidance or modification of the drug regimen. In these cases, the potential risks associated with the interaction may outweigh the benefits. This classification corresponds to Lexicomp categories D and X, signifying interactions with substantial implications for patient well-being.
The independent variables were included based on their associations with theoretical frameworks that explore polypharmacy and its association with pDDIs. Socio-demographic characteristics, such as educational level, can influence patients’ understanding of medication instructions and their ability to adhere to prescribed regimens. 9 Lower educational levels have been associated with higher risks of medication non-adherence or misuse, which increases the likelihood of polypharmacy and, consequently, pDDIs. Also, the number of sons/daughters or whether a patient lives alone is relevant because social support systems have been shown to play a role in medication adherence. Patients living alone may be at greater risk of polypharmacy due to the lack of family support or reminders, leading to potential medication errors and pDDIs. 10
Furthermore, the number of medications taken daily is a direct measure of polypharmacy and is one of the strongest predictors of pDDIs. Polypharmacy, especially among older adults, is often associated with multiple co-morbidities, which can lead to an increased risk of pDDIs. 11 The presence of CV and non-CV diseases is crucial in explaining the risk of pDDIs because chronic conditions often necessitate the use of multiple medications that may interact. Overall, the inclusion of these factors aligns with existing literature on polypharmacy, which demonstrates that polypharmacy is not only influenced by clinical characteristics, but also by socio-demographic characteristics.
CV and non-CV diseases have emerged as the leading causes of death among the Palestinian population, accounting for 65.7% of all recorded deaths, as documented by the Palestinian Health Information Center in 2018. Moreover, this trend is more pronounced in the West Bank, where these diseases constitute 57% of the causes of death, in contrast to 40% in the Gaza Strip. Among them, CV diseases stand out as significant contributors to illness, disability, and mortality in Palestine.12,13 This has resulted in a substantial increase in medication utilization, as well as in healthcare personnel and associated healthcare costs. Palestine is currently undergoing a significant epidemiological shift, with a vast increase in communicable diseases. At the same time, there is a silent but growing prevalence of non-communicable diseases, including CV diseases such as hypertension and diabetes mellitus, and non-CV diseases such as cancer. 14
Subsequently, understanding these independent variables can significantly help explain the risk factors leading to pDDIs, and effective interventions in medication management to avoid or minimize pDDIs. In instances where conflicting results arose between Drugs.com and Lexicomp, the classification of the drug interaction was determined based on the more severe category. Furthermore, all medications included in the study were categorized according to the WHO Anatomical Therapeutic Chemical Classification System (https://www.who.int/tools/atc-ddd-toolkit/atc-classification), which provides a standardized method for classifying drugs based on their therapeutic properties and anatomical targets.
Ethical considerations
Before commencing the study in Palestine, ethical approval was diligently obtained from the Ethical Committee at An-Najah National University (Reference No: Med. Feb. 2023/13), ensuring that the research adhered to ethical standards and guidelines. Subsequently, it was performed in compliance with the Helsinki Declaration for research in humans. 15 Also, all participants provided their informed consent to participate in this research before being included in the study. Additionally, this study conducted in Palestine aimed to investigate the prevalence of polypharmacy and the associated factors within the sampled population. Polypharmacy was defined in this study as the concurrent consumption of five or more medications on a daily basis.1⁰ For analytical purposes, medication use was further categorized into ≤5, 6–10, and >10 medications to examine the impact of increasing medication burden. Patients using 6–10 medications and those using more than 10 medications were considered subgroups within the polypharmacy category, with the latter reflecting excessive polypharmacy.
Study population and sample size calculation
With the escalation of the Israeli–Palestinian war and conflict in October 2023, there were drastic changes in the demographics of the Palestinian population. It is estimated that the Palestinian population was 5.5 million people as of mid-2022. Among this population, approximately 297,000 individuals were older ages including both early older ages, and older ages, accounting for 4.7% of the total population. Early older ages individuals refer to those aged 55–59 years old age group. They may still in the workforce and relatively healthy. However, they may start experiencing health-related problem and age-related changes. 12 Furthermore, older ages individuals refer to those aged 60 years old and above, which aligns with retirement age in Palestine and WHO definition. In specific regional breakdowns, the West Bank had nearly 196,000 individuals in this age group, representing about 6.2% of its total population. Meanwhile, the Gaza Strip had around 100,000 individuals aged 55 and above, constituting 4.7% of its total population. These population figures were derived from the 2022 census, as made available by the Palestinian Central Bureau of Statistics (The International Day of Older Persons 01/10/2023, https://www.pcbs.gov.ps/default.aspx).
Inclusion criteria used in participants’ selection were Palestinian patient diagnosed with at least one CV or non-CV disease, with an age ≥ 55 years and received more than one mediation.
We included some participants and a small group of early old patients from age of 55 to 59 years, to specifically examine the continuum of aging and to compare outcomes in this “early old” group with those in the traditional geriatric age group.
Exclusion criteria were non-Palestinian patient, on monotherapy, and illiteracy with inability to comprehend survey questions.
The calculated sample size for this study was 384, based on 50% prevalence, and using Daniel formula for sample size calculation:

Where n is the estimated sample size, Z is the statistic for a level of confidence, p is the expected prevalence or proportion, and d is the precision. Thus, the prevalence of potential pDDIs in Palestine was considered to be 50%, as the prevalence of pDDIs varies notably between CV and non-CV patients, influenced by factors such as polypharmacy and multi-morbidity. We used p as 0.50, to maximize the required sample size, and since as no prior specific prevalence data for the Palestinian geriatric population was available, representing a worst-case scenario for sample size calculation.
So, p = 0.50, while Z = 1.96 for 95% level of confidence, and d is the margin of error (set at 5%). While considering population size of 297000 as infinite population (https://www.who.int/campaigns/world-health-day/2024), and based on a 50% prevalence of pDDIs in Palestine, this calculation yielded an estimated minimum sample size of 384 individuals.
Consequently, complete data was collected from a total of 414 individuals suffering from CV and/or non-CV diseases. However, it is worth noting that the study results were based on data from 403 participants, as 11 participants who self-identified as illiterate were excluded from the analysis. This exclusion was implemented to ensure methodological rigor in research regarding pDDIs, as those participants did not understand questions or struggled to understand the questions, potentially affecting reliability. Additionally, the subjectivity of the collected data further justified their exclusion. Moreover, the participants were recruited randomly using simple random sampling method from medical records’ list of participants with CV and non-CV diseases, who visited the study settings regularly and continuously to ensure a proper selection of participants.
Statistical analysis
The Statistical Package for the Social Sciences (SPSS v.25) was used to perform statistical analysis, and an initial descriptive analysis was conducted for the main variables. A p-value < 0.05 was considered statistically significant. Descriptive and comparative statistics were carried-out for all variables, which were expressed as frequency and percentage for categorical variables, including socio-demographic and clinical characteristics such as the number of medications taken daily and types of pDDIs. The primary outcome variable was the presence or absence of major pDDIs. Therefore, binary logistic regression (i.e. univariate analysis) followed by multiple logistic regression analyses (i.e. multivariate analysis) of factors associated with major pDDIs were conducted, especially that the outcome variable (I.e. Major pDDIs) is containing two categories (I.e. Presence/Absence).
Several factors were considered as independent variables in these analyses, including patients’ socio-demographic characteristics such as: 1) gender; 2) age categories; 3) place of residency; 4) educational level; 5) marital status; and 6) number of sons/daughters, as well as clinical characteristics including: 1) CV diseases; 2) non-CV diseases; and 3) the number of medications taken daily. These independent variables were examined to assess their potential association with the likelihood of encountering a major pDDIs. The univariate analysis examined each variable individually, while the forward stepwise multivariate analysis explored their combined effects to determine significant predictors of major pDDIs occurrence. Subsequently, a chi-square test was used to assess differences in the percentages of pDDIs, including the three types (i.e. minor, moderate, and major), across different patients’ socio-demographic and clinical characteristics (e.g. number of medications).
Overall, we did two primary analytical streams:
Primary Regression Analysis: To identify predictors of Major pDDIs (a binary outcome: Presence/Absence) using univariate and multivariate logistic regression.
Secondary Descriptive Analysis: To describe the distribution of all three pDDI severity types (Minor, Moderate, Major) across participant characteristics using Chi-square tests.
Results
Socio-demographic and clinical characteristics of participants
In the study, a total of 403 participants were enrolled. The socio-demographic characteristics of these participants are summarized in Table 1. Notably, more than half of the participants were male, constituting 56.1% of the total sample. Additionally, a significant proportion, 56.8%, had completed their education at the school level. Furthermore, when considering the age distribution, the largest segment of participants (40.7%) fell within the 60–69 years age group. The majority of participants, 79.2%, indicated that they resided in the North of the West Bank of Palestine, and a substantial portion, 74.2%, were married. Lastly, having 4 to 6 children appeared to be the most common, with 43.9% of participants reporting this range, although it was less than half of the total sample.
Socio-demographic characteristics of participants (N = 403).
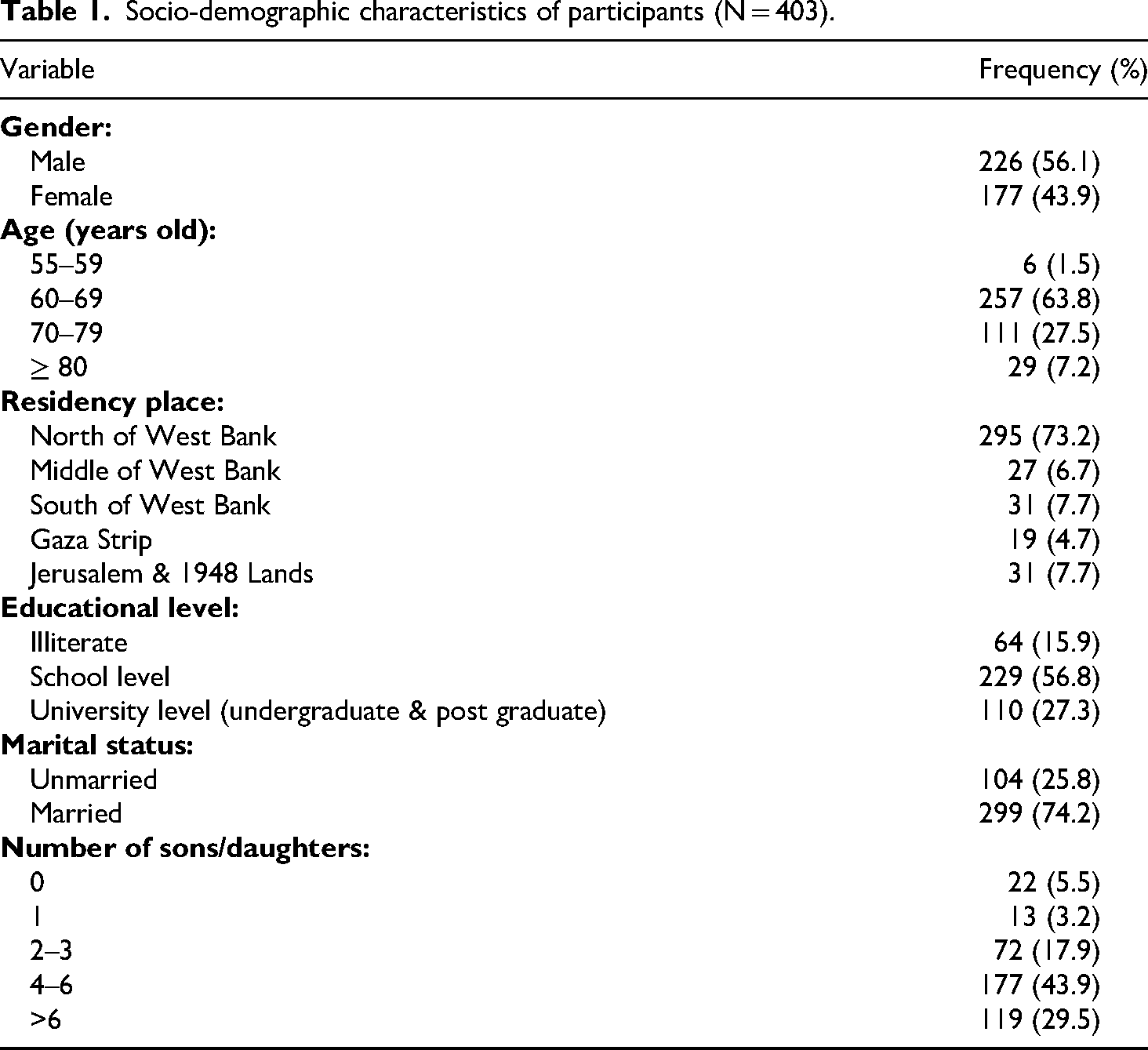
Table 2 provides an overview of the clinical characteristics of the participants in the study. Notably, less than half of the participants, specifically 43.2%, had hypertension and other CV diseases. Additionally, a significant majority, amounting to 59.8%, had been previously diagnosed with diabetes mellitus. Regarding medication usage, more than half of the participants, totaling 66.0%, were prescribed five or fewer medications on a daily basis. The study's findings revealed that a substantial majority of participants, represented by N = 300 (76.7%), experienced pDDIs. Among those participants who reported pDDIs, the majority of these interactions were categorized as moderate (68.0%), followed by major pDDIs (24.0%), and minor pDDIs (8.0%).
Clinical characteristics of participants (N = 403).
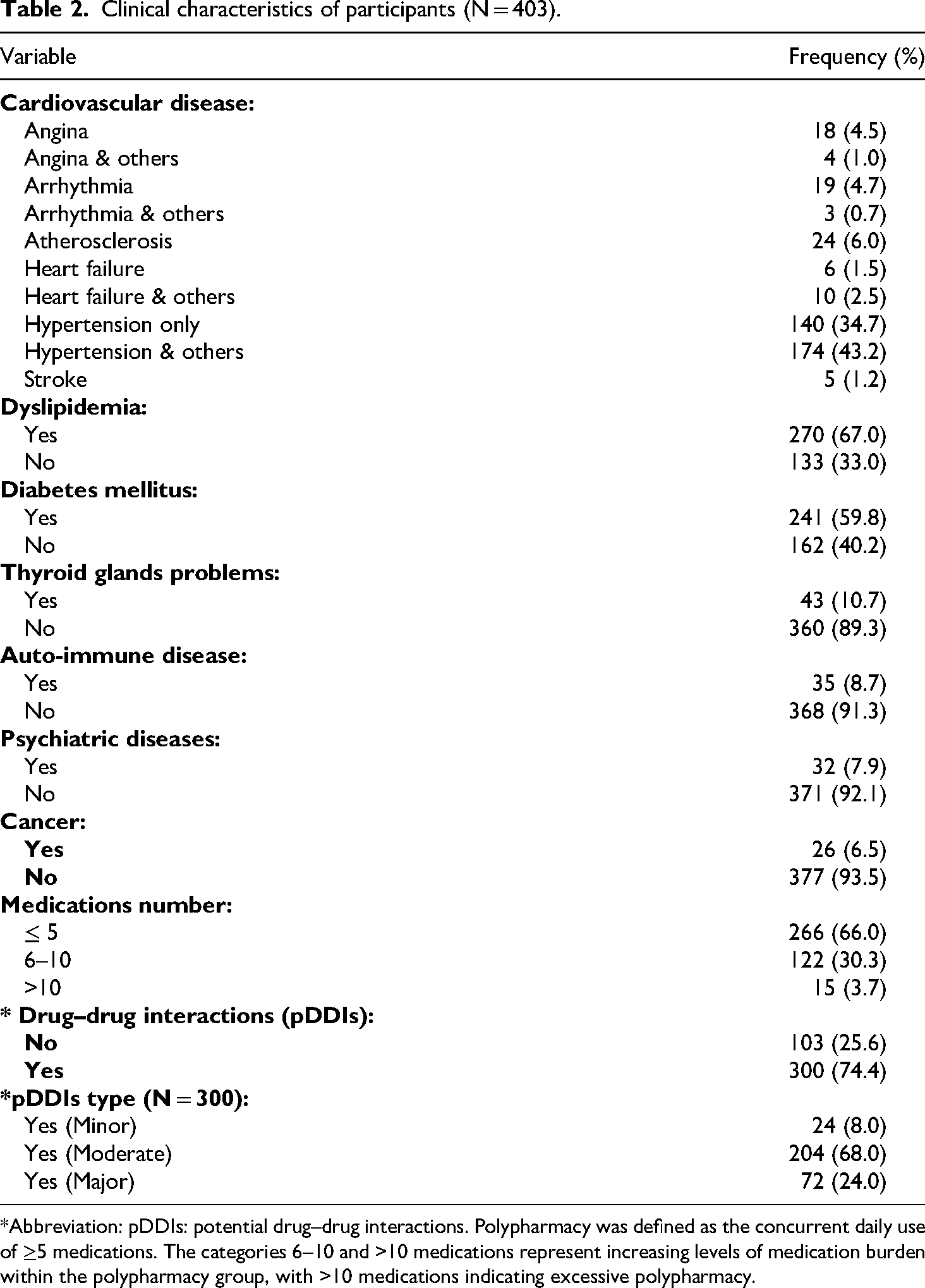
*Abbreviation: pDDIs: potential drug–drug interactions. Polypharmacy was defined as the concurrent daily use of ≥5 medications. The categories 6–10 and >10 medications represent increasing levels of medication burden within the polypharmacy group, with >10 medications indicating excessive polypharmacy.
Factors associated with major drug–drug interactions
In the context of major pDDIs, the univariate analysis conducted to examine associated factors (as shown in Table 3: Univariate Analysis) revealed significant associations between major pDDIs with educational level, marital status, and the number of medications taken by participants. The results indicated that participants with a school-level education were significantly more likely to experience major pDDIs (p < 0.05; OR = 1.224; 95% CI: 0.670–2.239). However, participants with a university-level education had a significantly lower likelihood of experiencing major pDDIs (p < 0.05; OR = 0.657; 95% CI: 0.342–1.259).
Univariate and multivariate analysis of factors associated with major drug–drug interactions (N = 403).

Polypharmacy was defined as the concurrent daily use of ≥5 medications. The categories 6–10 and >10 medications represent increasing levels of medication burden within the polypharmacy group, with >10 medications indicating excessive polypharmacy.
*Abbreviation: C.I: Confidence Interval.
**Bold p-values are statistically significant.
=Univariate Analysis.
==Multivariate Analysis.
Specifically, the analysis indicated that married participants were significantly more likely to experience major pDDIs (p < 0.05; OR = 1.376; 95% CI: 0.668–1.734) (Table 3: Univariate Analysis). Furthermore, when considering the number of daily medications, participants who received 6 to 10 medications daily (p < 0.001; OR = 3.178, 95% C.I: 1.085–5.371) and those who received more than 10 medications daily (p < 0.001; OR = 9.051, 95% C.I: 6.012–14.228) were significantly more likely to encounter major pDDIs (Table 3: Univariate Analysis).
Also, Table 3 showed multivariate analysis of factors associated with major drug–drug interaction. Subsequently, it demonstrates a significant association between marital status and number of medications taken on a daily basis with the occurrence of major pDDIs. Consequently, this analysis showed that being married and increased number of medications on a daily basis was significantly associated with increased odds of experiencing major pDDIs. Subsequently, married participants were found to be significantly more likely to have major pDDIs (p < 0.05; O.R = 1.166; 95% C.I: 0.682–1.995). Furthermore, participants who received 6 to 10 medications daily (p < 0.001; OR = 3.557; 95% C.I: 2.053–6.165) and those who received more than 10 medications daily (p < 0.05; OR = 9.141; 95% C.I: 1.176–71.042) were found to be significantly more likely to experience major pDDIs (Table 3: Multivariate Analysis).
Distribution of drug–drug interactions according to socio-demographic and clinical characteristics
Results shown in Table 4 highlight the distribution of pDDIs types among 403 study participants according to their socio-demographic characteristics. Subsequently, there were no statistically significant differences (p > 0.05) in prevalence of different pDDIs types among males and females. Furthermore, participants with different age groups had varying proportions of pDDIs types, including the highest prevalence of moderate pDDIs among participants whom their 60–69 years old, followed by those ages 70 −79 years old, even though differences were statistically non-significant (p = 0.438). In addition, Educational level, marital status, and number of sons/daughters did not significantly influence the prevalence and severity of different pDDIs types. Accordingly, residency place was the only socio-demographic characteristic with a significant difference (p < 0.05). Thus, levels of pDDIs types were significantly different among participants from different residency places (Table 4).
Drug–drug interactions types according to socio-demographic characteristics of study participants (N = 403).

*Abbreviation: pDDIs: potential drug–drug interactions.
**Bold p-values are statistically significant.
Differences in participants’ clinical characteristics showed statistically significant (p < 0.05) associations with differences in prevalence of different pDDIs types (Table 5). Subsequently, CV diseases types (p = 0.006), dyslipidemia (p = 0.004), diabetes mellitus (p = 0.000), auto-immune diseases (p = 0.001), cancer (p = 0.028), and the number of medications taken on a daily basis (p = 0.000) were significantly associated with the prevalence of different PDDIs types. This is showing that dyslipidemia, diabetes mellitus, auto-immune diseases, cancer, and a higher number of medications taken on a daily basis exhibited a significantly higher prevalence of moderate and major pDDIs (Table 5).
Drug–drug interactions types according to clinical characteristics of study participants (N = 403).

*Abbreviation: pDDIs: potential drug–drug interactions.
**Bold p-values are statistically significant.
Discussion
The geriatric Palestinian population faces healthcare challenges shaped by decades of geopolitical instability and fragmented healthcare services. Healthcare provision varies significantly across regions: the West Bank's services are administered by the Palestinian Ministry of Health and NGOs. In Gaza Strip, the healthcare system has been severely debilitated by a prolonged blockade and repeated conflicts. These structural disparities likely influence prescribing patterns, medication access, and adherence, forming a critical context for interpreting regional variations in polypharmacy and pDDI risk observed in this study. This baseline assessment, conducted immediately before the acute crisis of October 2023, captures these pre-existing conditions.
Polypharmacy, the concurrent use of multiple medications, is a common practice in modern healthcare systems, especially among older individuals and those with chronic diseases. While polypharmacy aims to comprehensively address various health concerns, it also poses significant risks, primarily through pDDIs. Our study investigated the prevalence and determinants of pDDIs among patient participants in Palestine.
The findings of our study emphasize the pervasive nature of polypharmacy and pDDIs among the Palestinian population. Our results revealed a high prevalence of pDDIs, with a substantial proportion of participants experiencing moderate and major interactions. These findings align with global concerns regarding the challenges posed by polypharmacy and confirm the importance of addressing this issue within local healthcare contexts.
Our study revealed a high prevalence of pDDIs among geriatric participants, with 76.7% of participants experiencing such interactions. This finding is consistent with prior research conducted by Zerah et al. (2021), which reported a similar prevalence rate of 75% among older adults. 16
One of the key determinants of major pDDIs identified in our study was the number of medications taken daily. Participants receiving a higher number of medications were significantly more likely to experience major pDDIs. This expected finding aligns with previous studies.17–20 It can be concluded that the risk of pDDIs is high among participants on a higher number of medications. The stratification of medication count into 6–10 and >10 medications was used to assess the effect of increasing medication burden and does not represent alternative definitions of polypharmacy.
Furthermore, our study identified marital status as a significant factor associated with major pDDIs, with married and separated/divorced individuals being more likely to experience major interactions compared to widowed individuals. While the reasons for this association are not yet fully understood, it highlights the need for healthcare providers to consider socio-demographic factors when assessing the risk of pDDIs and tailoring medication management strategies accordingly.
Our study identified marital status and the number of daily medications as significant factors associated with major pDDIs among geriatric participants. Specifically, married participants were more likely to experience major pDDIs, while those taking 6 to 10 or more than 10 medications daily were more likely to encounter major pDDIs. This contrasts with findings from Liu et al. (2021), where marital status significantly affected the potential for DDIs. 21
Our study also found significant associations between various clinical characteristics and the occurrence of pDDIs. For instance, participants with dyslipidemia and diabetes mellitus were more likely to experience moderate pDDIs, similar to findings by Liu et al. (2020). 22 Additionally, the association between CV diseases and major pDDIs aligns with research by Akbar et al. (2020), which highlighted the increased risk of pDDIs in patients with CV comorbidities. 23
Furthermore, participants with certain non-CV diseases, such as dyslipidemia and diabetes mellitus, were significantly more likely to experience moderate pDDIs. This might indicate that specific disease states may predispose individuals to a higher risk of pDDIs, possibly due to the complexity of their treatment regimens or shared pharmacokinetic pathways among medications commonly used to manage these conditions. 24
Moreover, the regional differences observed in the prevalence of pDDIs indicate the importance of considering local healthcare contexts when designing interventions to reduce the risks associated with polypharmacy. Participants residing in the northern region of the West Bank were more likely to experience moderate pDDIs, suggesting potential regional variations in prescribing practices or access to healthcare resources. This might be due to different medical guidelines used in the northern region for prescribing medications associated with a high risk of pDDIs or due to other reasons that require further investigation.
The study's limitations encompass several key areas. Firstly, reliance on self-reported data for medication usage and medical history introduces potential recall bias and inaccuracies. Secondly, selection bias may arise from recruiting participants from healthcare facilities, potentially skewing medication regimens and health profiles. Additionally, the study's focus on socio-demographic and clinical factors overlooks potential determinants such as genetic predispositions and dietary habits.
Conclusions
Overall, our study identified the prevalence and determinants of pDDIs among participant patients in Palestine. By identifying factors associated with major pDDIs, our findings can inform targeted interventions aimed at optimizing medication safety and reducing the burden of polypharmacy-related complications in this region. Future research is recommended to explore the underlying mechanisms driving the observed associations.
Footnotes
Acknowledgment
Authors would like to thank all participants for taking part voluntarily.
IRB approval
Ethical approval was diligently obtained from the Institutional Review Board (IRB), an ethical committee of An-Najah National University, Nablus, Palestine, at 13 February 2023. (Reference No: Med. Feb. 2023/13). Subsequently, the researcher provided each participant with a brief oral explanation about the study, its purposes and importance, as well as participants’ right, along with the consent form attached in the online questionnaire, which identifies the requirements and condition of study accession before asking them to agree to participate in the study.
Informed consent
All participants provided an informed consent before filling the questionnaire.
Author contribution
RM and YJ wrote the manuscript and supervised this research; SGQ collected the data from the participants; MG analyzed the data with RM.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Jurisdictional neutrality policy
Authors, Editors, Editorial Board members, and other individuals identified in the journal and on this website are asked to provide their institutional affiliation and country/region. SAGE does not take a position with respect to geographic designations or the legal status of any country or region that may be a disputed territory.