
Abstract
Background:
Both polypharmacy and potential drug-drug interactions (pDDIs), especially those at the pharmacokinetic level, are common in hospitalized patients and are associated with adverse effects and failure of therapy;
Objective:
The aim of the present study is to investigate retrospectively the prevalence of polypharmacy and the risk of potential pharmacokinetic drug-drug interaction among hospitalized patients;
Methods:
The medical documentation of hospitalized patients in the unit of internal diseases at the hospital “St Marina” in Varna, Bulgaria for a period of six months (January–July 2016) was retrospectively reviewed. Lexicomp® Drug Interaction software was used for the detection of pDDI. Descriptive statistic and logistic regression were used for data analysis;
Results:
In this study, 294 patients out of 510 (57%) were selected with polypharmacy. The number of detected potential pharmacokinetic DDIs (pPKDDIs) was only 216 (or 12,4%), but almost 40% of patients with polypharmacy were exposed to at least one pPKDDIs. The most common pPKDDIs occur at the biotransformation level – 78 (36,1%), and the most common enzyme form that is involved in these interactions is cytochrome 3A4 (44 or 20,4%). The number of prescribed medications (>7) was found to increase the possibility of having pDDIs (OR 25.535, 95% CI 12.529 to 52.042; p = <0.001) and pPKDDIs (OR 5.165, 95% CI 3.430 to 7.779; p = <0.001) as well;
Conclusion and Relevance:
Caution should be taken in patients taking more than seven drugs and careful assessment of the pPKDDIs should be made. When such interactions are detected, they need to be properly evaluated and managed.
Keywords
Introduction
Combination pharmacotherapy is the basis of the progress made in the treatment of many socially significant diseases in areas such as cardiology, oncology, infectious diseases, etc., but also it is the reason for the occurrence of higher frequency of adverse reactions, because of the increased number of used drugs.1–3 This complex pharmacotherapy is, in most cases, referred to as polypharmacy, and the most used definition of polypharmacy (used also for the purposes of the article), is the receiving of five or more medications from one patient. 4
The two types of drug interactions, pharmacokinetic and pharmacodynamic, can cause significant adverse reactions if not taken into account. Most physicians are well versed and can predict potential pharmacodynamic drug interactions, while the pharmacokinetic ones are more difficult for understanding and for prediction as well as are not fully confirmed in most cases. 5 Pharmacokinetic interactions can generally be presented as occurring at the four levels, very often presented with the following abbreviation – ADME (absorption, distribution, metabolism and excretion). Transport proteins, e.g. organic anion transporter (OAT), P-glycoprotein (P-gp), etc., and metabolizing enzymes, e.g. cytochrome P450 (CYPs), are involved in all pharmacokinetic processes, such as absorption, distribution and elimination. Drugs could be substrates or modulators (inhibitors inducers) of metabolizing enzymes and/or transport proteins that are responsible for the elimination of many drugs used in clinical practice. These interactions exactly are more significant and with greater consequences for the clinical practice.6,7 In addition, other factors, such as genetic variation (at the level of metabolizing enzymes, drug transporters, or both), further complicate the prediction of such interactions, and must also be taken into account. 8 That is why one of the main goals of drug research and development is to generate scientific reliable information about the potential pharmacokinetic drug-drug interactions (pPKDDIs) so that the physicians can have the necessary data to conduct safe clinical treatment when there is a danger of such interactions.
The main purpose of the present study was to review retrospectively hospitalized patients with polypharmacy for pPKDDIs, to determine the levels of interactions, their prevalence and their clinical significance.
Materials and methods
Design of the study
The medical documentation of hospitalized patients in the unit of internal diseases at the hospital “St Marina” in Varna, Bulgaria for a period of six months (January–July 2016) was retrospectively reviewed at the discharge. For the purposes of the article, the main selection criteria were – patients who received five or more drugs (polypharmacy). Prescribed pharmacotherapy in these patients has been screened for potential drug-drug interactions (pDDIs). Additionally, those patients with observed pPKDDIs were selected for a more detailed examination, such as level and main alleged mechanism of interaction, severity and risk rating of reaction and management recommendations. The Committee on Research Ethics at the Medical University “Paraskev Stoyanov” Varna, Bulgaria approved the current study. The complete patient information was kept private and was not available to the public.
Used software for detection of pDDIs
For determination of pDDIs were used Lexicomp® Drug Interactions (Wolters Kluwer, Hudson, OH). 9 The reason for choosing this software is that it shows high sensitivity and specificity in detecting and characterizing pDDIs. 10 The software classified the interactions into five categories: A (No known interactions), B (No action needed), C (Monitor therapy), D (Consider therapy modification) and X (Avoid combination). Each interaction was also indicated by the severity of the reaction in four stages - major, moderate, minor and N/A. In the description of the interaction there was also a paragraph describing the presumed mechanism of the interaction, which for the purposes of the article emphasizes was on the different levels of pPKDDIs.
Data reporting and analysis
The reporting data of this study conforms to the STROBE guideline. 11 The characteristics of patients and the pDDIs were shown as numbers (n) or percentage (%) and were analyzed using descriptive methods of means and standard deviations for continuous data. We have performed logistic regression analysis to determine the presence of correlation between separate variables, such as number of prescribed drugs, hospital stay and age, and the occurrence of pDDIs and pPKDDIs as binary variables (yes/no). For each predictor odds ratio (OR) with a 95% confidence intervals (CIs) were determined. p-value <0.05 was considered as statistically significant. The data were analyzed using Excel 2010 or SigmaPlot 11.0 software.
Results
Sociodemographic and clinical characteristics of patients included in the survey
After reviewing the prescribed medications at discharge for six months (January–July 2016) of all the patients – 510, which have passed through the internal unit of the “St Marina” University Hospital in Varna, Bulgaria, 294 patients were selected, based on the polypharmacy (receiving ≥ 5 drugs). The general characteristics of the selected patients are shown in Table 1.
Main patient's characteristics included in the study.

Abbreviations: eGFR, estimated glomerular filtration rate; COPD, Chronic obstructive pulmonary disease.
Out of 294 selected patients, 157 (53.4%) were female and 137 (46.6%) were male. According to age, the majority of the patients were in the elderly group (>60)—224 (76.2%), as the number of those between 40 and 59 was 66 (22.5%) and under 40 – only 4 (1.4%). The average age was 68.1 (±12.22 SD).
Prevalence of pDDIs detected by Lexicomp®
The total number of pDDIs was 1742, or approximately 5.9 (±4.9 SD) pDDIs per one person. Overall, 95% of selected patients with polypharmacy had at least one pDDI, regardless of type. The most common drug interactions with respect to the risk rating were in group C—1463 (84.0%), requiring careful monitoring of patients. One hundred and seven patients (6.1%) were in group D of their pDDIs, for which it is advisable to consider changing the therapy used. Contraindicated pDDIs (group X, 0.5%) with recommendation to avoid them, were detected in only nine patients. Based on severity of reaction, the most pDDIs were in moderate group – 1510 (86.7%), while those in major group were 98 (5.6%). All results are summarized in Table 2.
Classification of detected pDDIs.

A (No known interactions); B (No action needed); C (Monitor therapy); D (Consider therapy modification); X (Avoid combination).
Potential pharmacokinetic drug-drug interactions (pPKDDIs)
Most of the detected interactions (>85%) are pharmacodynamic in nature or have an unclear mechanism. pPKDDIs cover a relatively small proportion of all detected interactions – 216 (12.4%). However, the studied medical cards of the selected patients were 294, 113 of them showed at least one pPKDDIs, or approximately 40 percent (38.4%). The data are summarized in Table 3.
Potential pharmacokinetic drug-drug interactions (pPKDDIs) detected in patients included in the study.

Abbreviations: AUC, area under the curve; PPB, plasma protein binding; OATP, organic anion transporting polypeptides; BCRP, breast cancer resistance protein; P-gp, P-glycoprotein; CYP, Cytochrome P450; OAT, organic anion transporter; OCT, organic cation transporter; MATE, multidrug and toxic compound extrusion.
As can be seen from the table, the most common pPKDDIs occur at biotransformation level – 78 (36.1%), and the most common enzyme form that is involved in these interactions is cytochrome 3A4 (44 or 20.4%). Interactions associated with altered absorption showed the next higher prevalence among pharmacokinetic interactions – 52 (24.1%), followed by altered excretion – 50 (23.1%) and distribution – 36 (16.7%) respectively.
The most common pairs of individual pharmacokinetic levels of interactions and their management are presented in Table 4. As most pPKDDIs are highly dependent on the used dose and the chosen dosing regimen, the table shows those of the interacting drugs, as well as a comment on their effect in the given case.
pPKDDIs, their putative mechanism and management.

Abbreviations: PRN, as needed; BID, twice daily; TID, three times daily; NSAID, nonsteroidal anti-inflammatory drug.
Factors associated with pDDIs
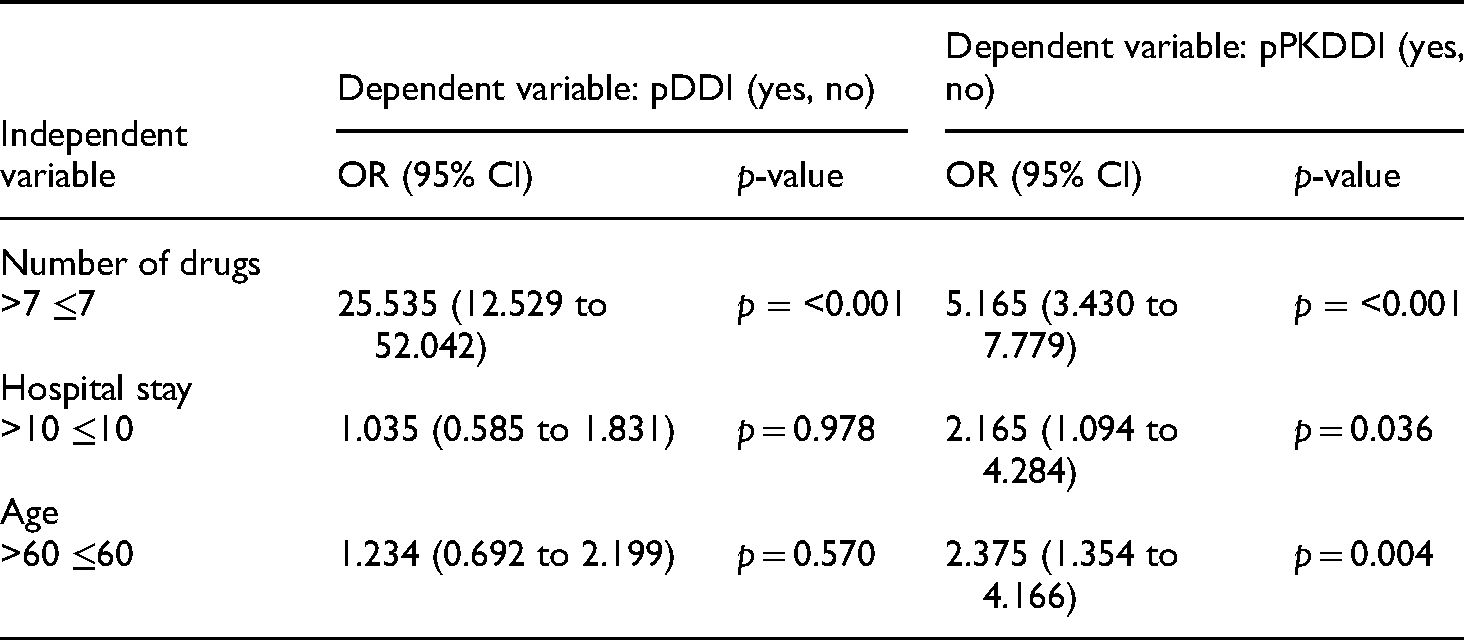
After performing the analysis, the results have shown positive correlation of the number of the prescribed drugs and the occurrence of the pDDIs – OR 25.535 (95%CI 12.529 to 52.042; p = <0001). For the other predictors, such as age and hospital stay, no statistically significant difference was observed – 1.234 (95% CI 0.692–2.199, p = 0.570) and 1.035 (95% CI 0.585–1.831, p = 0.978), respectively (Table 5). The occurrence of pPKDDIs has shown positive correlation with all studied factors – number of prescribed drugs (OR 5.165; 95% CI 3.430–7.779; p = <0.001), hospital stay (OR 2.165; 95% CI 1.094 to 4.284; p = 0.036) and age (OR 2.375; 95% CI 1.354 to 4.166; p = 0.004) (Table 5).
Predictors associated with pDDIs and pPKDDIs.
Discussion
Potential drug-drug interactions are common in hospitalized patients. Knowledge of these interactions and how to manage them can reduce the frequency of side effects and increase the degree of effectiveness. Therefore, the purpose of this study is to provide information on the most commonly observed pDDIs (with an emphasis on pPKDDIs) in prescriptions of hospitalized patients, their prevalence and type depending on the severity of the reaction and the pharmacological mechanism of the interaction and how to manage them.
In the present study, prevalence of the polypharmacy (≥5 drugs) was detected in 294 medical charts (selected for the present study) out of 510 examined, which means that every second patient had a prescribed polypharmacy. Excessive polypharmacy (≥10 drugs) was identified in 55 medical charts (∼11%). Out of these selected patients with polypharmacy, at least one pDDIs was detected in 280 of them (95%) or approximately 5.9 (±4.9 SD) pDDIs per one person. According to the polypharmacy, these results are close to those reported by recently published data conducted in elderly patients with cardiovascular disease in a hospital in Ethiopia by Assefa et al. 12 and by other authors as well.13–15 The frequency of pDDIs among patients with polypharmacy was quite identical to the data reported by Nusair et al. 16 with slight differences about mean values – 4.2 ± 3.0 vs. 5.9 ± 4.9 (in the present study) per patient. In general, it can be concluded that polypharmacy is a common phenomenon in hospitalized patients and should be taken into account by physicians, because of its direct relation to the possibility of developing pDDIs.
The most common detected types of pDDIs were in the risk category C (84.0%) and based on the severity of the reaction – in the moderate group (86.7%). These interactions do not require, in most of the cases, any special action, but rather close monitoring of the patients. Those results correspond to our previously published article 17 and also to that from other authors,18,19 with slight change in the percentage, but in the same range. Major pDDIs, in the risk categories D and X, were relatively rare – 6.1% and 0.5% respectively (Table 2), but they deserve special attention because in most cases they are associated with drugs with low therapeutic index (e.g. statins, anticoagulants, cardiac glycosides, antithrombotics, methotrexate etc.) and can significantly harm the patient's health.17,20,21
Pharmacokinetic drug interactions occur when a drug alters absorption, distribution or elimination (disposition) of a simultaneously administered drug, leading to changes in its plasma concentration levels. 5 As mentioned in the result section, relatively small amount of pPKDDIs (216 or 12,4% of all pDDIs) were recognized by the software program. The involved pharmacokinetic levels are represented in Table 3. Interactions occurring at the level of metabolizing enzymes and transport proteins are considered to be with the greatest clinical significance. Inhibition or induction of these enzyme systems and transport proteins is highly dependent on the doses and the dosing regimens used. 6 In our study, these interactions were predominant and almost equally prevalent – those of them involving metabolizing cytochrome enzymes (CYPs) and transport proteins were – 76 (4.4%) and 78 (4.5%) respectively. Other authors report a significantly higher frequency of pPKDDIs (CYPs or transporter). In the study published in 2018 by Bajracharya et al. reported 36.9% pharmacokinetic interactions out of 657 DDIs. 22 Doan et al. detected 80% of CYP-mediated DDIs among patients with polypharmacy, as this risk increases as a function of the number of medications dispensed. 23 Zakrzewski-Jakubiak et al. revealed the same incidence of CYP-mediated DDIs as the most involved CYPs are 3A4, 2D6 and 2C9 with 70.2%, 22.7% and 3.4% respectively. 24
Usually, pharmacokinetic interactions are described as involving one of the levels, but sometimes the mechanisms are complex – they may affect both the distribution and elimination processes of the influenced drug or involve both pharmacokinetic and pharmacodynamic mechanisms. Of the pharmacokinetic interactions presented in Table 4 (an example of such complex) interaction is acenocoumarol and co-trimoxazole (sulfamethoxazole/trimethoprim). Оn the one hand, displacement of acenocoumarol from the plasma proteins binding sites and on the other hand inhibition of metabolism (via CYP2C9) by sulfonamide (sulfamethoxazole) are the putative pharmacokinetic mechanisms. Alteration of GI flora responsible for production of vitamin K by co-trimoxazole may be involved in pharmacodynamic mechanisms. Lexicomp software classifies the reaction as D and based on severity as major, and recommends reducing the dose of coumarin anticoagulant by 10% to 20% prior to starting the sulfonamide antibiotic and then monitoring INR closely to further guide dosing. Some authors are more critical and recommend the use of alternative antibiotics instead of adjusting the dosage regimens of the two drugs.25,26 Another similar complex interaction (not shown in Table 4) is between acenocoumarol and levothyroxine, which was detected in one of the patients. Several mechanisms have been proposed: (1) binding of coumarin anticoagulants to plasma proteins may be decreased in hyperthyroid patients (PK); (2) thyroid hormone increases the affinity of vitamin K-dependent epoxide reductase for coumarins (PD); (3) more pronounced metabolism of vitamin K-dependent blood clotting factors in patients with increased thyroid function (PD). The software program classifies the reaction as C and based on severity as moderate, and recommends monitoring by the physicians for increased anticoagulant effects of vitamin K antagonists and regularly review the patient's thyroid status. 27 In some cases, both drugs may interact with each other, affecting their pharmacokinetics, therefore the final result may be difficult to predict. An example of such interaction is rosuvastatin and telmisartan. Telmisartan inhibits ABCG2-efflux transporter (also known as BCRP), which takes part in the disposition of rosuvastatin, thereby increasing plasma concentration of the last one. In turn, rosuvastatin could increase exposure of telmisartan, by competition for the hepatic uptake transporter – OATP1B3 and glucuronidation by UGT1A3. The software characterizes it as insignificant (B/minor), which has been confirmed in clinical trials.28,29 The given examples were intended to present the complexity and difficulties in predicting, evaluating, and managing pPKDDIs. In most cases, they require a special approach. On the one hand, the use of appropriate software for their detection, while on the other hand, a specialist, such as a clinical pharmacist, is needed, with experience in the field of drug interactions, to suggest a course of action. As mentioned above, dose and dosing regimen play an important role in interactions. In our study, several patients with doses above the recommended and concomitantly using interacting drug were detected – one patient taking amlodipine and a high dose of simvastatin – 40 mg (recommendations are no more than 20 mg dose) and four patients taking high doses of methotrexate - >15 mg weekly with NSAIDs. In the latter case, NSAIDs are prescribed only when necessary, which reduces the risk of serious interactions.
After performing the analysis, we haven't found statistically significant association between age, hospital stay and pDDIs (Table 5). However, we found a significant one between the number of drugs taken (>7) and the pDDIs. The frequency of pPKDDIs increases with all analyzed factors (number of taken drugs, hospital stay and age) with statistical significance. In addition, almost every second patient (38.4%) with polypharmacy is with an increased risk of pPKDDIs, which is an indication that there is a need to know the mechanism of pharmacokinetic interactions and the ways to manage them. In our previously cited study in patients with heart failure, no correlation was found between age and pDDIs, while such was observed between the number of drugs taken and pDDIs. 17 Moura et al. 30 have demonstrated a link between the length of hospital stay in intensive care units and the risk of developing potential drug interactions. Other authors confirm this relation, as well as that between age, number of taken drugs and the risk of developing pDDIs.19,31,32 A study conducted in patients over 45 years of age in Primary Care, Southern Brazil by Teixeira et al., 33 have found no statistically significant association regarding age, but a significant one when the patients take three or more drugs and risk of pDDIs.
Limitations of the study
A single software was used to detect pDDIs and pPKDDIs. The reasons for this were that the software has one of the largest databases and that it has a high sensitivity. 10 Also, the assessment of pPKDDIs has not been evaluated in terms of timing of administration since we had no information about time window.
Conclusions
In the present study, a high incidence of polypharmacy and pDDIs observed in hospitalized patients in the unit of internal diseases was shown. Therefore, caution should be taken in patients with more than seven prescribed drugs and careful assessment of the risk of the possible pDDIs. pPKDDIs generally comprise a small proportion of all interactions, but almost 40% of patients with polypharmacy were exposed to at least one pPKDDIs. Their risk increases with the number of drugs taken, and significantly less with the hospital stay and age, and should be taken into account. They are difficult to predict and therefore require a specific approach – the use of appropriate software or a clinical pharmacist with experience in the field of drug interactions.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank the colleagues from the Internal Disease Unit at St Marina University Hospital in Varna, Bulgaria for the provided data.
Declaration of conflicting interests
The Autors declare that there is no conflict of interest
Ethics approval
Ethical approval to report this case was obtained from ethics committee of medical university “Prof. Dr Paraskev Stoyanov” – Varna, ethics approval number 105/18.08.2021.
Informed consent
Informed consent for patient information to be published in this article was not obtained because this is a retrospective study and all patient details are de-identified.