
Abstract
Introduction
The World Health Organization listed heart disease as the leading cause of death in 2022; 1 the number of Korean adults undergoing surgery for acquired heart disease is also rising. 2 Cardiac surgery is a complex and high-risk procedure that requires postoperative ventilator treatment, intensive observation in the intensive care unit (ICU), and transfer to a general ward when the condition improves. 3 Patients admitted to the ICU after surgery are at high risk of delirium due to various factors, such as drainage tubes and monitors attached to their bodies, movement restrictions and pain caused by ventilator application, day and night indistinguishable lighting, noise, and psychological anxiety. 4 Such treatment and environmental factors in the ICU impact the occurrence of delirium in both the ICU and general ward. 5
Delirium is a clinical syndrome characterized by a short-term lack of attention, poor concentration, sudden changes in consciousness, and decreased persistence; it is accompanied by various symptoms such as decreased reality and distorted cognition, illusion, and hallucination. 4 In a previous study, delirium occurred in 11–14% of hospitalized patients in the general ward and 34–50% of ICU patients, 6 and the incidence of delirium after cardiac surgery was 43–55%.7,8 The occurrence of delirium after cardiac surgery negatively impacts the prognosis and recovery of patients. Aggressive behavioral patterns and excessive excitement and sleep disorder by delirium delay ventilator departure after surgery, which increase both ICU and hospital stays and decrease treatment compliance; this leads to increased complications and mortality. 9 Additionally, the occurrence of delirium after cardiac surgery affects the patient's long-term cognitive function, increases the probability of hospital readmission after discharge, and reduces the quality of life. 10
Delirium can be recovered when the triggering factor is removed; hence, early detection and intervention through the identification of risk factors can prevent its occurrence in patients and improve its prognosis. 4 In addition, the delirium management guidelines recommend a higher level of nonpharmaceutical intervention to alleviate delirium symptoms than drug administration therapy after delirium occurs. 11 Managing delirium in patients is crucial and requires early identification of risk factors, prevention, and timely intervention; however, in a busy work environment, the importance of nursing for patients with severe disease and delirium management may be overlooked. 12 Considering that the unresolved risk factors in the ICU may influence the occurrence of delirium after transferring to the general ward after 2–3 days in the ICU, it is important to continuously monitor the associated factors for delirium management in the ICU even after transfer to the general wards. 9
Delirium is not caused by a single factor but rather results from the interaction of various factors. 6 Patient age, preoperative alcohol consumption, and smoking are associated with postoperative delirium.6,13 Fasting time, sedative administration time, disease severity, ICU stay and ventilator application period, and application of continuous renal replacement therapy (CRRT) are factors that affect the occurrence of delirium.4,14,15 In addition to the disease-related factors identified as risk factors for delirium in cardiac surgery patients, various complex risk factors associated with patients need to be analyzed, including factors such as nursing needs, postoperative sleep disturbances, bedsores, and catheter number.6,7,16
Delirium occurrence after overseas cardiac surgery is 13.3–17.5% in ICU and 39–50% in general wards, suggesting that delirium occurs even after moving patients from ICU to general wards after surgery.6,9 Considering the current trend where cardiac surgery patients spend less time in the ICU and more time in general wards, 17 it is necessary to assess the continuity and sustainability of the occurrence of delirium after surgery in both ICU and the general wards. 9 Accordingly, this study expanded the scope of adult cardiac surgery patients beyond the postoperative ICU admission period to determine the timing and extent of delirium occurrence and identified the risk factors that impact the occurrence of delirium; thus, we can provide basic data for the development of nursing interventions for delirium management.
Methods
Research design and subjects
This is a retrospective research study to identify the timing and extent of delirium occurrence after surgery in adult patients undergoing cardiac surgery and to identify the risk factors for delirium occurrence. This study included a total of 195 subjects who met the selection criteria, excluding 167 who met the exclusion criteria, out of 362 subjects who underwent heart surgery at Yeungnam University Hospital during the period from January 2020 to June 2021. The specific selection criteria for study subjects were adult patients over the age of 18 who had cardiac surgery, patients who did not develop delirium before cardiac surgery, patients without cognitive impairment, and patients who were able to physically act. The specific exclusion criteria for participants in this study are patients with a history of neurological treatment due to neurological problems caused by brain lesions after heart surgery, patients diagnosed with neuropsychiatric diseases and dementia before heart surgery or taking related drugs, and patients who reentered the ICU during the post-heart surgery investigation period. The sample size of this study was calculated as a two-sided test for logistic regression using the G-power 3.19 program, 19 predictors, .85 power, and .05 significance level, and the minimum sample size was 178 people based on the above criteria.
Research tool
Delirium
In this study, based on the Nursing Delirium Screening Scale (Nu-DESC) developed by Gaudreau et al., delirium was evaluated with the approval of the original author and translator 18 and the Korean Nu-DESC, which was modified by Kim et al. to suit the Korean situation. 19 The tool consists of five questions: decreased persistence, inappropriate behavior, inappropriate conversations, auditory hallucinations, and psychotropic delay items, which are screened as delirium when they score 2 or more out of 5 points in total. The tool has a sensitivity of .85 and a specificity of .73 when calculated based on a psychiatrist's delirium diagnosis. This is similar to the sensitivity .77–.89, and specificity .72–.75 of the most widely used delirium analysis tool Confusion Assessment Method for the ICU. 19
Characteristics of the subjects’ delirium generation
Disease and treatment-related characteristics were investigated for comorbid diseases, type of surgery, operation time, postoperative pain, postoperative inflammatory reactions, postoperative nothing per os (NPO) time, postoperative time to use sedatives, Acute Physiology and Chronic Health Evaluation Ⅱ (APACHE Ⅱ) score, 20 length of ICU stay, ventilator application period, CRRT application, postoperative demand of nursing, sleep disorders, postoperative pressure ulcer, and the number of catheters. The postoperative nursing demands of the patient were investigated by categorizing them into four groups based on the total score measured by the Korean Patient Classification System ICU after surgery. 21
Data collection
This study received approval for data collection from the Institutional Review Board of Yeungnam University Hospital (YUMC202112046-HE001). This study is a retrospective investigation study, which was exempted from the requirements for written or oral consent of the subject from the institutional review committee; the researcher checked the subject's medical records and collected data. The identification information of the study subjects was managed by assigning an arbitrary study subject number, and all related documents were encrypted and stored in a researcher's private space with a double stash device so that only the researcher could access it. In this study, the delirium screening period was based on previous studies, and the average hospital stay after cardiac surgery was 8 days, and the occurrence of delirium was investigated for 10 days after cardiac surgery, considering that delirium occurred from 2 to 6 days after surgery.3,5,22 Patients who had delirium at least once were classified as the delirium group, and those who had never had delirium were classified as the nondelirium group. To confirm the reliability between evaluators, the degree of agreement between one nurse with more than 5 years of clinical experience and a sample of 25 out of the 195 subjects was analyzed using percentage agreement and Kappa values. As a result of analyzing the degree of agreement between investigators, the percentage of agreement was 96.0%, and the Kappa value was confirmed to be .91.
Analysis method
Data collected in this study were analyzed by setting the significance level below .05 using the IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA). The general characteristics, disease, and treatment-related characteristics of the subjects were demonstrated by real numbers and percentages, mean, and standard deviation. Postoperative delirium incidence and delirium patterns of patients were presented by real numbers, percentages, mean, and standard deviation. The difference in characteristics according to the presence or absence of delirium was analyzed by independent t-test and chi-square test. Risk factors for the development of postoperative delirium were analyzed using logistic regression analysis, with variables with statistically significant differences between the delirium and nondelirium groups as independent variables and the presence or absence of delirium as the dependent variable.
Results
Patient characteristics
The mean age of the 195 subjects in this study was 66.56 ± 11.31 years: 145 (74.4%) of them were male and 50 (25.6%) were female. A total of 119 (61.0%) of the subjects were accompanied by high blood pressure, and coronary artery bypass surgery was the most common in 107 subjects (54.9%). The average operation time was 5.97 ± 1.39 h, and the NPO time after surgery was 28.53 ± 12.58 h. Patients’ postoperative sedative use time averaged 24.89 ± 22.43 h, APACHE Ⅱ score averaged 17.19 ± 5.98 points, mean length of ICU stay was 2.33 ± 1.87 days, ventilator application period was 1.33 ± 0.92 days, and 22 subjects (11.3%) applied CRRT. Patient's postoperative demand for nursing was the highest with 116 (59.5%) critically ill patients in group 3. There were 161 (82.6%) patients who did not have sleep disorders after cardiac surgery, and 142 (72.8%) subjects who did not develop pressure ulcers. The average number of catheters after cardiac surgery was 8.57 ± 0.96 (Table 1).
Patient characteristics (n = 195).

Data are presented as number (%) or mean ± standard deviation.
APACHE, Acute Physiology and Chronic Health Evaluation; CABG, coronary artery bypass graft; CRF, chronic renal failure CRRT, continuous renal replacement therapy; CVA, cerebrovascular accident; ICU, intensive care unit; NPO, nothing per oral; KPCS-ICU, Korean Patient Classification System-Intensive Care Unit.
Multiple response.
Incidence and symptoms of delirium after cardiac surgery
As a result of checking the degree of delirium occurrence after heart surgery, 67 (34.4%) of the total 195 patients had delirium. According to an analysis of 67 patients (34.4%) who had delirium after cardiac surgery, 36 (53.7%) had delirium in the ICU, and 31 (46.3%) in the general ward. In terms of the patient's delirium pattern, inappropriate communication was the most common with 60 (30.8%), followed by inappropriate behavior with 53 (27.2%), disorientation with 36 (18.5%), illusions/hallucinations with 20 (10.3%), and psychomotor retardation with 12 (6.2%) (Table 2).
Incidence and symptoms of delirium after cardiac surgery (N = 67).

Data are presented as number (%) or mean ± standard deviation.
ICU, intensive care unit; POD, postoperative day.
Multiple response.
Comparison of characteristic differences between delirium and nondelirium groups
There were significant differences in age, preoperative stroke comorbidities, surgery type, postoperative inflammatory response, postoperative fasting time, sedative administration time, APACHE Ⅱ score, length of stay in the ICU, ventilator application period, and CRRT application. The average age of the delirium group was 7.6 years, which was higher than that of the nondelirium group (t = 4.66, p < 0.001), many patients had preoperative strokes (χ2 = 5.96, p = 0.015), and two or more surgeries were performed at the same time (χ2 = 16.08, p = 0.001). In addition, compared to the nondelirium group, the delirium group has an average operation time (t = 2.60, p = 0.010) and NPO time (t = 3.99, p < 0.001), time to use sedatives (t = 3.77, p < 0.001), length of ICU stay (t = 5.37, p < 0.001), and the ventilator application period was long (t = 3.77, p < 0.001). The delirium group, rather than the nondelirium group, had a postoperative inflammatory response (χ2 = 20.25, p < 0.001), and there were many applications of postoperative CRRT (χ2 = 24.77, p < 0.001); the APACHE Ⅱ score indicating the severity of the disease was high (t = 4.58, p < 0.001). On the other hand, the nondelirium group had a lower need for postoperative demand of nursing (χ2 = 13.20, p = 0.001), postoperative sleep disorders (χ2 = 8.46, p = 0.004), and a lower number of catheters (t = 2.64, p = 0.009) than the group with delirium (Table 3).
Comparison of characteristic differences between delirium and nondelirium groups (n = 195).

Data are presented as number (%) or mean ± standard deviation.
APACHE, Acute Physiology and Chronic Health Evaluation; CABG, coronary artery bypass graft; CRF, chronic renal failure CRRT, continuous renal replacement therapy; CVA, cerebrovascular accident; ICU, intensive care unit; NPO, nothing per oral; KPCS-ICU, Korean Patient Classification System-Intensive Care Unit.
Multiple response.
Risk factors for delirium occurrence
To identify the risk factors for the subjects for developing delirium after surgery, a logistic regression analysis was performed using variables that showed significant differences between the delirium and nondelirium groups as independent variables and the presence or absence of delirium as the dependent variable. As a result of performing the Hosmer–Lemeshow model fit test, the goodness-of-fit of the regression model was significant (χ2 = 9.88, p = 0.274), and Cox & Snell's coefficient of determination (R² = .42), which indicates the explanatory power of the model, showed 42% explanatory power, Nagelkerke's coefficient of determination (R² = .58) showed an explanatory power of 58%.
As a result of the analysis, those aged 70 or older had 6.23 times (95% confidence interval [CI] = 1.70–22.84, p = 0.006) higher delirium incidence rate than those under 60, the postoperative inflammatory response is 10.18 times (95% CI = 2.39–43.31, p = 0.002), the application of postoperative CRRT is 9.05 times (95% CI = 1.90–43.21, p = 0.006), subjects with length of ICU stay between 2 and 4 days had 3.83 times (95% CI = 1.13–12.97, p = 0.031) higher risk of delirium occurrence than those with a stay of fewer than 2 days. Patients with a history of stroke had 3.71 times (95% CI = 1.12–12.33, p = 0.033), higher risk of delirium after surgery a higher APACHE Ⅱ score had 1.12 times (95% CI = 1.03–1.21, p = 0.006) higher risk of delirium, and a 1.01 times higher risk of delirium with a longer operating time (95% CI = 1.00–1.01, p = 0.042). Subjects’ postoperative sleep disorder increased the risk of delirium by 8.98 times (95% CI = 2.91–27.76, p < 0.001) and also increased the risk of delirium by 1.53 times (95% CI = 2.91–27.76, p < 0.001) as the number of postoperative catheters increased (Table 4).
Risk factors of delirium after cardiac surgery (n = 195).
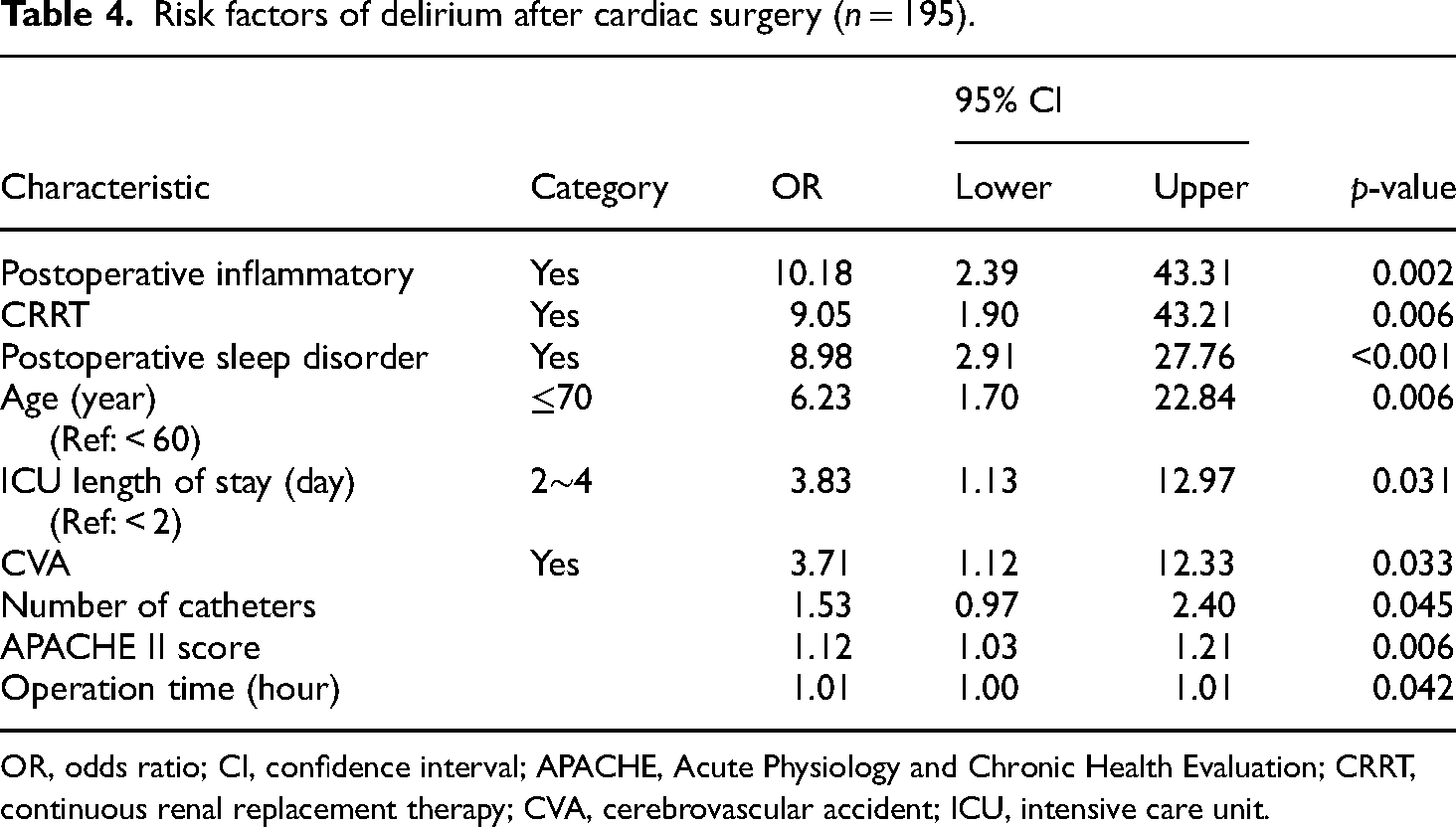
OR, odds ratio; CI, confidence interval; APACHE, Acute Physiology and Chronic Health Evaluation; CRRT, continuous renal replacement therapy; CVA, cerebrovascular accident; ICU, intensive care unit.
Discussion
This study was conducted to provide basic data on the development of nursing interventions for delirium management by identifying the timing and extent of delirium occurrence after surgery in adult patients who underwent cardiac surgery and identifying the risk factors that impact delirium occurrence.
In this study, the occurrence of delirium was 34.4%, similar to or different from 15% to 50% of previous studies.7,9,23 This may be due to the difference in the delirium evaluation period after surgery. In this study, among all patients who developed delirium, 53.7% experienced it in the ICU, and 46.3% experienced delirium after moving to a general ward, showing that postoperative delirium occurs not only in the ICU but also after moving to a general ward. This suggests that it is crucial to prepare a nursing strategy for careful observation and prevention of delirium occurrence even after the patients move from the ICU to the general ward after cardiac surgery.
Age is identified as a risk factor for delirium occurrence and a history of stroke is highly related to delirium occurrence in most hospitalized patients, including cardiac surgery patients.6,7,14 Older patients are more prone to acquire comorbidities due to aging, and the vulnerability to drug toxicity increases due to decreased metabolic function.13,14 Brain region lesions caused by stroke are reduced in activity of the cholinergic nervous system, resulting in reduced ability to cope with acute stress situations such as surgery. 24 In particular, imbalances in neurotransmitters, such as acetylcholine secretion deficiencies involved in arousal and concentration, increase the risk of delirium development and emphasize the importance of delirium management in the elderly. 6 Therefore, elderly patients over 70 years of age and stroke victims who have undergone imaging surgery will be classified as high-risk groups for delirium; efforts for early detection and active delirium prevention activities will be important strategies.
Patients who have undergone cardiac surgery must be treated in the ICU for the application of ventilators and intensive observation after the surgery. However, holding a conduit in the ICU after cardiac surgery, application of CRRT, and length of stay were identified as risk factors for delirium occurrence. Mechanical noise in the ICU and conduit retention and immobility, separation from family cause stress and anxiety in patients, increasing the risk of delirium. 25 However, it should be noted that delirium management may be overlooked due to the nature of the ICU, where nursing care for seriously ill patients takes priority. To manage delirium, nurses classify and manage patients who have been in the ICU for more than two days as a high-risk group; cooperation and efforts among medical staff are required to periodically assess unnecessary catheters and remove them early.
Unlike the findings of Siew et al., 15 which suggested that the application of postoperative CRRT in the ICU reduces the risk of delirium by removing inflammatory mediators, metabolites, and neurotoxins in patients with kidney injury, 15 this study identified it as a risk factor for delirium occurrence. Discomfort related to immobility and mechanical noise resulting from the application of CRRT after surgery in the ICU may increase the risk of developing delirium. 25 In addition, CRRT can be affected by differences in patient severity and various variables; hence, repeated studies are needed to confirm the association with the occurrence of delirium.
It can be seen that, the longer the patient's surgery time, the higher the risk of delirium due to increased use of anesthetics and surgical-related drugs that affect delirium occurrence.13,26 Meanwhile, the use of a cardiopulmonary bypass during surgery can cause delirium due to nerve damage caused by a cerebral inflammatory response, as blood inside the body stagnates outside the body through an artificial circuit. 27 Considering the fact that the use of a heart-lung machine during surgery is necessary due to the nature of cardiac surgery, repeated research is needed to confirm the relationship between the patient's operation time and the time of artificial heart-lung machine use with the occurrence of delirium. The patient's inflammatory response is a risk factor for delirium,13,28 and this study also found that the risk of delirium after surgery was approximately six times higher. Stimulations such as surgery and infection activate immune cells in the body, causing inflammatory reactions and cerebral inflammation, which lead to nerve damage in the brain and neurotransmission imbalance, thereby increasing the risk of delirium. 29 This suggests that providing nursing activities to prevent infection after cardiac surgery is a crucial strategy for preventing delirium.
The APACHE Ⅱ score, which represents a patient's disease severity, contains variables related to delirium, such as the Glasgow Coma Scale and age, which can identify a patient's neurological problems as evaluation items. In addition, the higher the severity of the disease, the lower the body's ability to defend against acute stress situations such as surgery, and the higher the risk of delirium.6,13,30 For this reason, it can be seen that patients with a high APACHE Ⅱ score are vulnerable to delirium occurrence; this was also identified as a risk factor for delirium occurrence in this study. Early detection and intervention through the identification of delirium risk factors can prevent the occurrence of delirium in patients and improve the prognosis of the disease. 4 Therefore, priority should be given to checking the APACHE Ⅱ score of cardiac surgery patients after surgery, conducting periodic assessments, and preventive nursing interventions for the occurrence of delirium in patients with high disease severity.
Finally, the subjects’ postoperative sleep disorder has been identified as a risk factor for delirium, which is consistent with the results of several previous studies.16,31 A patient's sleep disorder causes fatigue, anxiety, attention deficit, and poor concentration, thereby increasing the risk of delirium.6,13 It is important to note that the occurrence of delirium after cardiac surgery affects the patient's prognosis and recovery.9,26 This suggests that to prevent delirium, the patient's sleep status after cardiac surgery should be closely monitored, and nursing intervention to improve sleep is necessary.
In this study, the degree of delirium after cardiac surgery and the risk factors were analyzed. In addition, ICU-related factors were continuously observed even after the patient moved to the general ward. In clinical practice, it is important to consider ICU-related risk factors and to continue observation and management even after patients are moved to a general ward. This is crucial for managing delirium that occurs after cardiac surgery. Furthermore, based on the results of this study, it will be important to develop and apply an intervention program in clinical practice to prevent delirium occurrence in patients who have undergone cardiac surgery.
Limitations of this Study
This study has the following limitations. First, since this study confirmed the degree of delirium occurrence during the period up to 10 days after surgery, it was not possible to confirm the occurrence of delirium after 10 days. Further research suggests that an expanded study that observes the entire hospital stay period after surgery is needed to accurately confirm the occurrence of delirium. Second, this study is a retrospective research study, and there is a limitation for not considering environmental factors such as noise and lighting that can affect the occurrence of delirium after surgery.
Conclusion
In this study, the degree and risk factors of delirium occurrence after cardiac surgery were analyzed, and ICU-related factors were continuously observed even after the patient moved to the general ward. To manage delirium in adult cardiac surgery patients, nurses must recognize the importance of continuously observing the risk factors related to delirium in the ICU even after they move to a general ward. Various risk factors for delirium after cardiac surgery have been identified. Based on the results of this study, developing and applying nursing interventions to prevent delirium will be a critical strategy for delirium management.
Footnotes
Acknowledgements
Thank you to the dedicated patients who gave their time to participate for this study.
Authors’ contribution
Study conception and design: K-SH. Data collection: K-MS. Data analysis and interpretation: K-SH, K-MS. Drafting of the article: K-SH, K-MS. Critical revision of the article: K-SH.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
For this study's data collection, medical records were collected with approval from the medical information center of the affiliated institution after the Institutional Review Board (IRB) approval (YUMC202112046-HE001).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.