
Abstract
Chronic venous disease (CVD) of the lower extremities constitutes a progressive clinical entity that compromises venous hemodynamics, leading to structural and functional alterations predominantly due to venous reflux. With an estimated global prevalence of approximately 60%, CVD exerts a substantial negative impact on quality of life. Historically dismissed as merely aesthetic, the condition is now recognized for its symptomatic burden, which can considerably impair daily functioning and well-being.
Objective
To describe the epidemiological and clinical profile of patients with CVD treated at a university hospital and to identify demographic, clinical, and behavioral factors associated with disease severity according to the Clinical-Etiology-Anatomy-Pathophysiology (CEAP) classification.
Methods
A cross-sectional prospective study was conducted with 674 patients evaluated with CVD at the Angiology Teaching and Clinical Care Unit of Pedro Ernesto University Hospital. Demographic, clinical, and behavioral data were analyzed according to the CEAP classification using ordinal logistic regression to identify factors associated with disease severity.
Results
A predominance of female patients (78.9%) was observed, with a mean age of 56.5 years. The most frequently reported symptoms were leg pain (reported by 80.7% of patients), lower-limb edema (68.7%), and burning sensation (63.8%). Higher Body Mass Index (BMI) was significantly associated with advanced CEAP stages (P < .001), identifying obesity as a key modifiable risk factor.
Conclusion
Higher BMI was the only modifiable variable independently associated with advanced stages of CVD.
Introduction
Chronic venous disease (CVD) encompasses a spectrum of long-standing morphological and functional abnormalities affecting the superficial and/or deep venous systems of the lower extremities. 1 These changes are frequently associated with clinical signs and symptoms that warrant diagnostic evaluation and therapeutic intervention. CVD exhibits a progressive course, often advancing with time and potentially leading to venous reflux in initially uncompromised venous segments. 2
Globally, the prevalence of CVD in the adult population is estimated at approximately 60%. 3 In Brazil, although epidemiological data remain limited, prevalence is estimated to be around 48%. 4 Multiple risk factors have been implicated in the pathogenesis of CVD, including older age, female sex, positive family history, obesity, and multiparity.2,3,5,7
Historically considered a condition of cosmetic relevance, CVD is now recognized as a major cause of physical discomfort, pain, reduced work productivity, disability, and deterioration in quality of life (QoL). Common symptoms include tingling, aching, burning, cramps, edema, throbbing sensations, pruritus, restlessness, fatigue, and limb heaviness. These symptoms are often exacerbated by prolonged standing or exposure to heat and are typically relieved by rest or limb elevation. 5
The Clinical-Etiology-Anatomy-Pathophysiology (CEAP) classification is a globally recognized standard for describing patients with CVD. It is widely used for reporting clinical research findings in scientific journals. Establishing a standardized clinical classification system for CVD is essential for understanding the disease's natural progression and for comparing different diagnostic and treatment methods. 6
In advanced stages, CVD is associated with considerable morbidity. Venous ulcers (VUs), a hallmark of late-stage disease, are painful, refractory to treatment, and prone to recurrence in the presence of chronic venous hypertension. Additionally, up to 60% of CVD patients may develop superficial venous thrombosis, which may evolve into deep vein thrombosis (DVT) in over half of cases. 7 Despite its high prevalence and clinical impact, Brazilian epidemiological data on CVD remain sparse, limiting the identification and management of key risk factors.
Objective
To describe the epidemiological and clinical profile of patients with CVD treated at a university hospital and to identify demographic, clinical, and behavioral factors associated with disease severity according to the CEAP classification.
Methods
A cross-sectional, prospective, descriptive observational study was conducted at the Angiology Teaching and Clinical Care Unit (Unidade de Docência Assistencial em Angiologia) of Pedro Ernesto University Hospital, affiliated with the State University of Rio de Janeiro (HUPE-UERJ). This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 8 guidelines for cross-sectional studies. The study protocol was approved by the Research Ethics Committee of HUPE-UERJ, on February 24, 2024 (CAAE: 76149523.6.0000.5259; Approval Number: 6.654.622). This study was conducted in accordance with the Declaration of Helsinki 1975, as revised in 2024.
A consecutive non-probabilistic convenience sampling method was adopted, including all eligible patients evaluated during routine outpatient visits between March 2023 and August 2024. This period corresponded to the time required to consecutively recruit the entire population of patients meeting the inclusion criteria at the study site. No formal sample size calculation was performed, as this study had an exploratory design. The final sample of 674 patients represents all individuals consecutively assessed during the study period and was considered adequate to explore associations between demographic, clinical, and behavioral factors and the clinical stages of CVD.
A total of 674 patients aged 18 years or older, presenting with clinical signs and/or symptoms consistent with CVD, were assessed with medical history and physical examination. There were no restrictions based on upper age limit or ethnicity. Patients under 18 years of age and those with complaints or physical findings inconsistent with CVD were excluded. The participants provided written informed consent, and all patient details were de-identified.
Data were collected prospectively using a standardized form completed by the attending physician during each clinical encounter. To reduce potential bias, all assessments were performed in person by trained angiologists using the same structured instrument to ensure uniform evaluation and documentation of clinical variables. Selection bias was minimized by enrolling all consecutive patients who attended the vascular outpatient clinic during the study period and fulfilled the eligibility criteria. Information bias was limited through direct clinical examination and patient interview conducted during the visit.
Analyses were based on objective criteria, including the CEAP classification, and multivariate models were applied to adjust for potential confounders. All recorded information reflected data routinely obtained in standard angiology practice.
The following variables were analyzed: age, sex, clinical signs and symptoms (heaviness, pruritus, cramps, evening edema, burning sensation, varicose bleeding), disease duration, family history of CVD prior DVT and/or erysipelas, smoking status (current or former), prolonged standing time (>6 hours/day), body mass index (BMI), physical activity level, number of pregnancies (in females), prior use of venoactive drugs for ≥30 days, and previous sclerotherapy or varicose vein surgery. Disease severity was graded according to the CEAP classification. For statistical purposes, CEAP clinical stages were stratified into two categories: C0–C2, denoting mild or early-stage disease, and C3–C6, denoting advanced disease. This classification is consistent with current literature, which considers CEAP stage C3 and above as indicative of the more severe spectrum of CVD. 10
All data were processed and analyzed using Jamovi® software (version 2.3). Descriptive statistics were applied to summarize the study population. Categorical variables are presented as absolute and relative frequencies, whereas continuous variables are expressed as means and standard deviations.
Associations between independent variables and disease severity, as defined by CEAP clinical stages, were examined using an ordinal logistic regression model. All collected variables were included in the multivariate model based on their clinical relevance to the progression of CVD, allowing simultaneous adjustment for potential confounders.
Adjusted odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were calculated. No formal subgroup or interaction analyses were performed, as this was not within the scope of the study design. Likewise, sensitivity analyses were not conducted. Only complete cases were included in the analysis. As the dataset was derived from routinely collected clinical information during in-person evaluations, missing data were minimal and did not impact the primary analysis.
Due to the use of consecutive convenience sampling, no weighting or adjustment based on the sampling strategy was required in the analytical model.
Results
Demographic and clinical characteristics
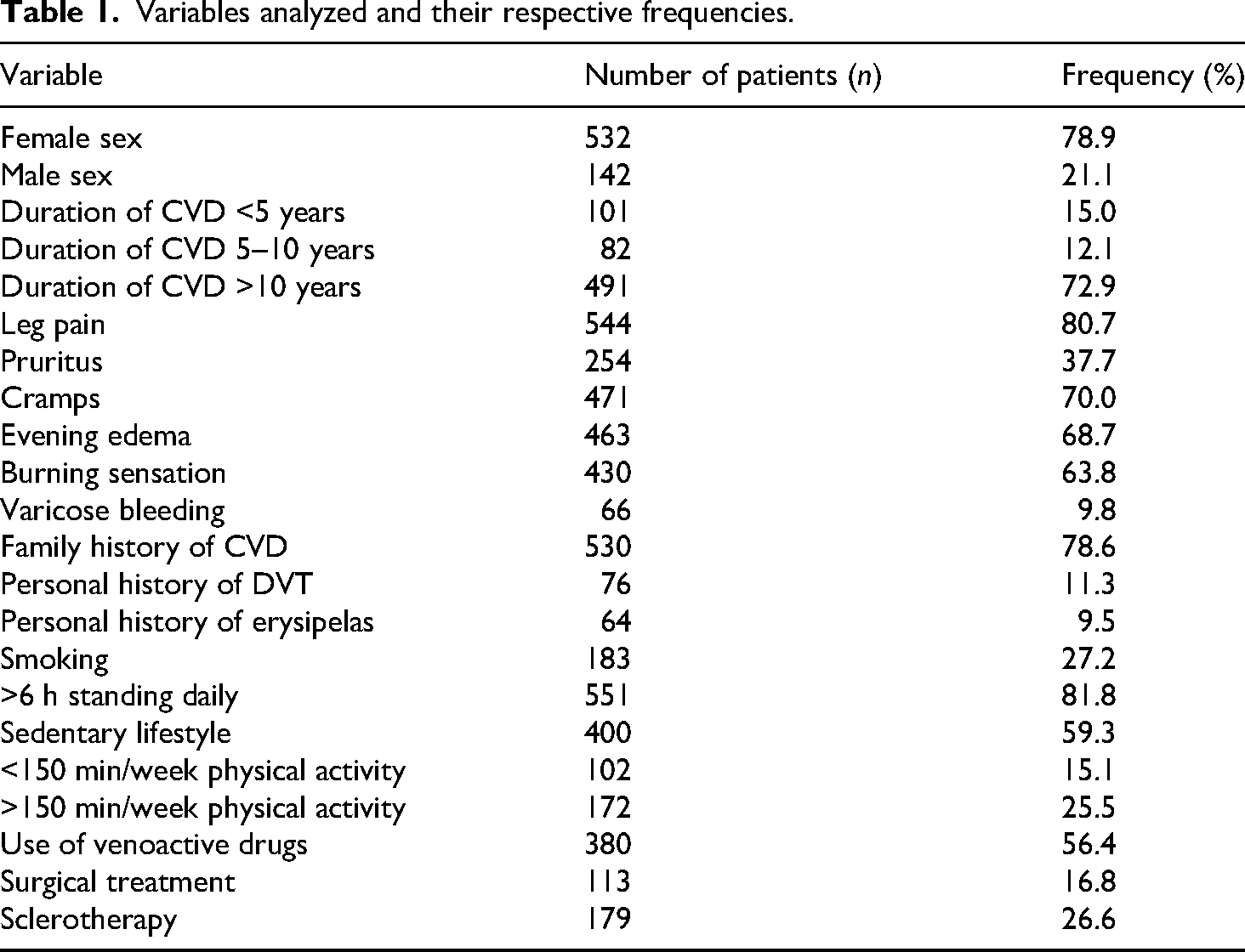
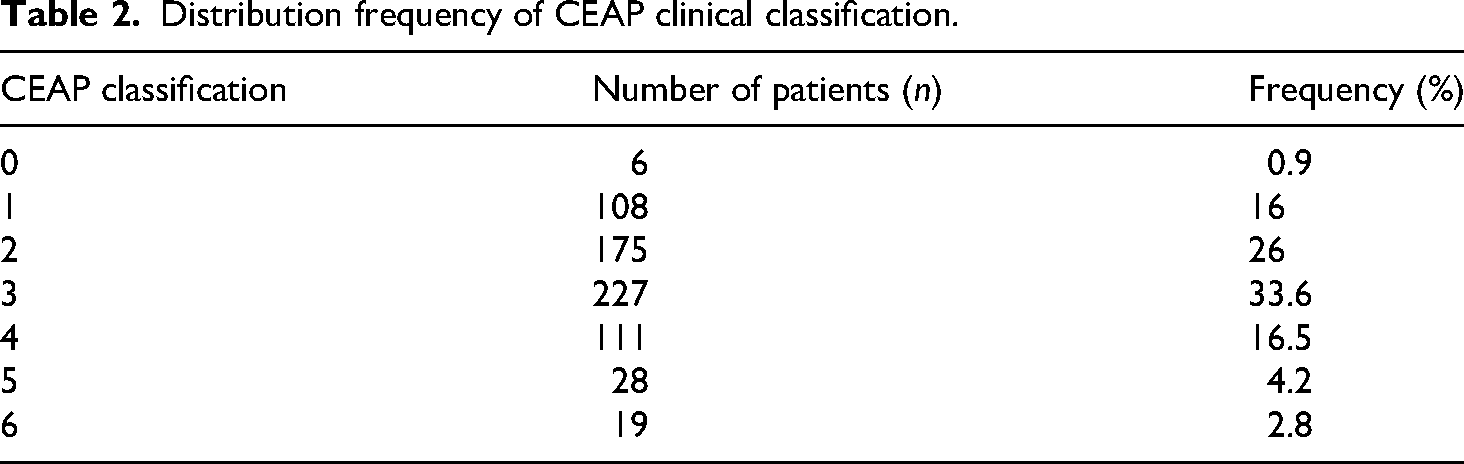
During the study period (March 2023–August 2024), 675 patients were assessed for eligibility during routine outpatient visits at the Angiology Teaching and Clinical Care Unit of HUPE-UERJ. Of these, 674 patients were included in the study, and 1 patient was excluded due to age under 18 years or findings inconsistent with CVD. A total of 674 patients with a clinical diagnosis of CVD were evaluated. The patients’ characteristics are summarized in Table 1. The majority were female (n = 532; 78.9%), while 142 (21.1%) were male. The mean age of participants was 56.5 years (median 57 years). According to the CEAP classification, the most common clinical stage was C3 (n = 226; 33.6%), mainly characterized by lower limb edema (Table 2).
Variables analyzed and their respective frequencies.
Distribution frequency of CEAP clinical classification.
Prevalence of symptoms and signs
The most reported symptom was leg pain, present in 544 patients (80.7%). Edema was reported by 463 patients (68.7%), followed by burning sensation in the lower extremities in 430 patients (63.8%).
Risk factors
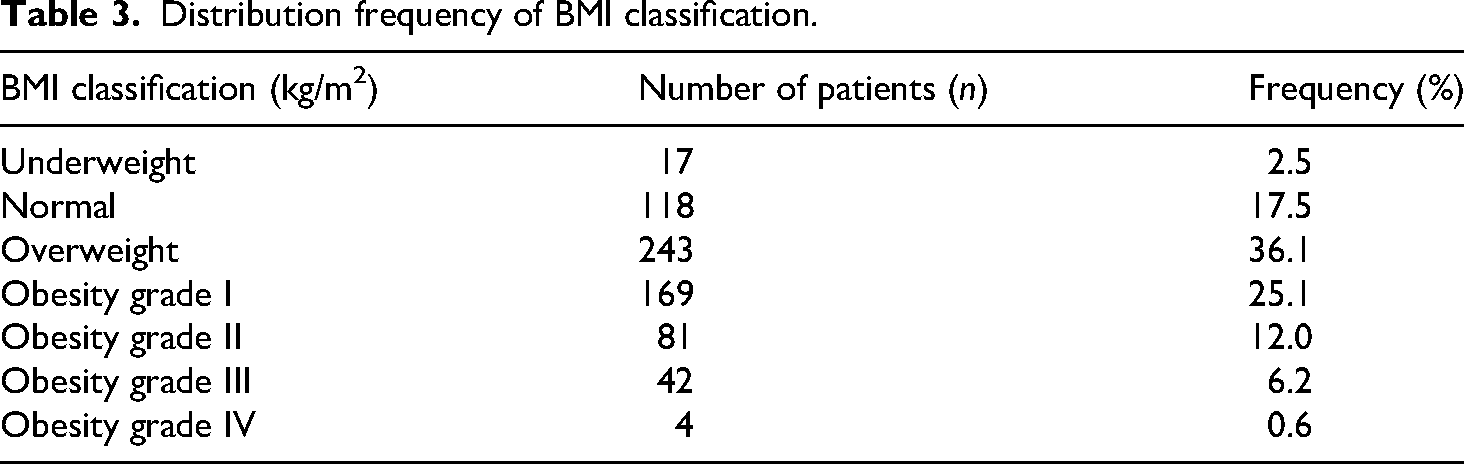
A positive family history of CVD was reported by 530 individuals (78.6%). Sedentary lifestyle was reported by 400 patients (59.3%), and 114 (16.9%) were active smokers. Regarding BMI, 213 patients (31.6%) were overweight (BMI 25–29.9 kg/m2), and 296 (43.9%) were classified as obese (BMI ≥30 kg/m2). Only 118 participants (17.5%) had a normal BMI (Table 3). Additionally, 76 patients (11.3%) reported a history of DVT, and 64 (9.5%) had experienced at least one episode of erysipelas. A significant proportion of the sample (n = 551; 81.8%) remained in a standing position for more than 6 hours daily.
Distribution frequency of BMI classification.
Previous treatments
Regarding prior therapeutic interventions, 380 patients (56.4%) were using venoactive drugs at the time of the consultation, while 113 (16.8%) had undergone invasive treatment (conventional varicose vein surgery or sclerotherapy) for CVD.
Correlation between variables and CEAP classification
A univariate ordinal logistic regression analysis was conducted to assess the association between each independent variable and CEAP clinical stages (0–6) as the dependent variable. Variables significantly associated with more advanced CEAP stages (P = .05) included leg pain (P = .193), cramps (P = .144), burning sensation (P = .293), family history of CVD (P = .104), smoking status (P = .585), standing time >6 hours/day (P = .223), prior surgery (P = .302), and prior sclerotherapy (P = .733). Confidence intervals for unadjusted estimates were not calculated due to the focus on multivariable analysis in this study.
Ordinal logistic regression analysis revealed that several variables were significantly associated with more advanced CEAP clinical stages (Table 4). Among them, BMI emerged as the only modifiable factor with a statistically significant correlation to disease severity (P < .001). Age (P < .001; OR = 1.024; 95% CI: 1.013–1.036) and male sex (P < .001; OR = 2.596; 95% CI: 1.777–3.805) were also independently associated with more advanced stages.
Correlation between dependent variables and CEAP clinical classification.

Clinical signs such as evening edema (P < .001; OR = 2.496; 95% CI: 1.784–3.503), pruritus (P = .002; OR = 1.648; 95% CI: 1.207–2.252), and history of varicose bleeding (P < .001; OR = 3.500; 95% CI: 2.070–5.956) also showed statistically significant associations with greater disease severity.
Disease duration between 5 and 10 years (P = 0.008; OR = 1.783; 95% CI: 1.161–2.746), history of DVT (P = .001; OR = 2.172; 95% CI: 1.364–3.468), and previous erysipelas (P < .001; OR = 3.288; 95% CI: 1.912–5.680) were other relevant predictors.
Conversely, former smokers exhibited a lower likelihood of presenting with advanced disease (P = .006; OR = 0.510; 95% CI: 0.315–0.824).
The overall regression model demonstrated satisfactory fit (likelihood ratio test, P < .001), supporting the robustness of these associations.
Discussion
CVD is a highly prevalent clinical condition, affecting approximately 60% of the global adult population and approximately 48% of adults in Brazil. 4 Although associated with low mortality, CVD imposes considerable morbidity, adversely impacting QoL and contributing to elevated healthcare and social security expenditures due to recurrent hospitalizations, reduced work productivity, and prolonged treatments.2,5 In Brazil, CVD ranks as the 14th most frequent cause of temporary work disability, with over 61,000 hospital admissions recorded in 2000. Of those, 13,000 hospitalizations were due to active VUs. 9
The present study revealed a predominance of female patients (78.9%) and a mean age of 56.5 years, consistent with epidemiological profiles described in the literature. 10 The CEAP stage C3—defined by the presence of lower limb edema—was the most frequent, affecting 33.6% of participants. Individuals classified as CEAP C3 to C6 are considered to have chronic venous insufficiency (CVI), representing the more severe spectrum of CVD. 11
As expected, the most frequently reported symptoms were pain (80.7%), edema (68.7%), and burning sensations (63.8%). This is in line with clinical findings that associate these symptoms with disease progression and increased functional limitation.2,3,5 Beyond the physical burden, CVD has also been associated with mental health impairment, particularly in advanced stages. Studies have demonstrated a higher prevalence of depression and anxiety in patients with CVI, attributed to chronic pain, reduced mobility, and impaired self-esteem.12–15
Among the evaluated risk factors, family history of CVD was notably prevalent (78.6%), while sedentary lifestyle affected more than half of the sample. Although not statistically significant, physical inactivity may indirectly contribute to disease progression by promoting weight gain and obesity. In this cohort, 43.9% of patients were classified as obese, reinforcing national trends indicating a growing prevalence of obesity in Brazil. 16
BMI emerged as a modifiable variable independently associated with advanced clinical stages (P < .001). Obesity exerts its deleterious effects on venous hemodynamics by increasing intra-abdominal and venous pressures, impairing valvular function, and promoting reflux.2,17 Additionally, it may hinder the efficacy of conservative and invasive treatments, increase the incidence of postoperative complications, and prolong VUs healing time, particularly in patients with comorbid diabetes. Obesity also limits the use of compressive therapy and contributes to higher recurrence rates after interventions. Yet obese individuals are often underrepresented in clinical trials, leading to a gap in evidence-based strategies for this population. 17
Regarding therapeutic practices, 56.4% of patients were using venoactive drugs, while only 16.8% had undergone procedural treatment. This aligns with international guidelines that recommend conservative management in early stages and reserve surgical or endovenous procedures for patients with significant symptoms or complications.3,5
Taken together, these results highlight the importance of identifying and addressing modifiable risk factors such as obesity and sedentary behavior in the prevention and management of CVD. Early detection and intervention may mitigate disease progression, improve QoL, and reduce long-term healthcare costs.
Limitations
This study has limitations that should be acknowledged. The use of convenience sampling in a tertiary hospital may limit the generalizability of findings to broader community populations, as patients attending a tertiary care center may present with more severe disease. Furthermore, the cross-sectional design precludes the establishment of causality between risk factors, such as obesity, and disease progression. The absence of subgroup analyses may have limited the identification of specific risk factors in distinct populations (e.g., by age or sex). Finally, unmeasured confounders, such as genetic predispositions or socioeconomic factors, may have influenced the observed associations. Despite these limitations, the study provides valuable epidemiological insights into CVD in a Brazilian hospital setting, highlighting the burden of modifiable risk factors—particularly obesity—on disease severity. Such data are essential to guide prevention strategies, inform public health policies, and support the development of targeted interventions aimed at reducing the prevalence and progression of CVD.
Conclusion
In this cross-sectional prospective analysis, obesity was identified as the only modifiable variable independently associated with more advanced clinical stages of CVD according to the CEAP classification, alongside non-modifiable factors such as age and male sex. These results reinforce the epidemiological relevance of obesity within the clinical spectrum of CVD and may contribute to the understanding of its demographic and clinical distribution in a Brazilian outpatient hospital setting.
Footnotes
Acknowledgments
We express our deep appreciation to Dr Rodrigo Kikuchi for his critical review and insightful contributions, which greatly enhanced the scientific rigor and clarity of this work. His guidance was of immeasurable value throughout the development of this manuscript.
We also extend our sincere gratitude to Dr Lilian Câmara da Silva for her invaluable support during the patient data collection phase of this study. Her dedication and professionalism were essential to ensuring the quality and integrity of the dataset.
ORCID iDs
Ethical considerations
This study was approved by the Research Ethics Committee of HUPE-UERJ (CAAE: 76149523.6.0000.5259; Approval Number: 6.654.622).
Consent to participate and publication
The participants provided a written informed consent to use personal information, which has been anonymized. The written informed consent was approved by the Research Ethics Committee.
Authors’ contributions
Conception and design: Isabel de Castro Nunes Senfft, Marcos Arêas Marques, Juliana de Miranda Vieira. Acquisition, analysis and interpretation of data: Isabel de Castro Nunes Senfft, Marina Araujo Zulchner, Marianne Freire Peixoto, Marcela do Couto Soares de Paula Barros, Jorge Eduardo da Silva Soares Pinto. Drafting of the article and literature search: Isabel de Castro Nunes Senfft, Marcos Arêas Marques, Maurício Faria Corvisier. Critical revision: Carmen Lucia Lascasas Porto, Ana Letícia de Matos Milhomens. Final approval: all authors contributed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.