
Abstract
Introduction:
We investigated the risk factors that increased the frequency of blood transfusions in elderly patients with intertrochanteric hip fractures to determine blood transfusion risk before surgery and to take selective precautionary measures in the group at high risk for transfusion to ensure safe surgery.
Materials and methods:
We retrospectively reviewed the electronic medical records of 203 patients who underwent surgical fixation of intertrochanteric hip fractures from January 2015 to December 2020. We hypothesized that patient sex, age, body mass index, preoperative hemoglobin, preoperative platelet count, glomerular filtration rate (GFR), preoperative albumin level, American Society of Anesthesiologist score, intraoperative blood loss, duration of surgery, method of anesthesia, and time from injury to surgery would affect the need for blood transfusion. Student's t-test, Chi-squared test, and the one-way analysis of variance test were used to determine whether differences between variables in the transfusion and non-transfusion groups were significant.
Results:
Unstable fractures (P = 0.002), general anesthesia (P = 0.028), lower preoperative hemoglobin levels (P < 0.001), and lower GFRs (P < 0.001) were identified as related to blood transfusions in univariate analysis. In multivariate logistic analysis, the need for allogeneic blood transfusion in unstable fractures was approximately 2.949 times higher than in stable fractures (P = 0.009). The risk in general anesthesia patients was about 2.953 times higher than in spinal anesthesia patients (P = 0.007). In addition, the need for allogeneic blood transfusion increased by about 1.293 times as preoperative hemoglobin levels decreased by 1 g/dL (P = 0.017) and increased by about 1.017 times as the GFR decreased by 1 mL/min/1.7m2 (P = 0.006).
Conclusion:
Low preoperative hemoglobin levels, low GFRs, general anesthesia, and unstable fractures in elderly patients with intertrochanteric hip fractures increased the risk of blood transfusion.
Introduction
The incidence of intertrochanteric hip fractures in elderly people has increased annually recently due to extended life expectancy and the increased number of elderly patients with osteoporosis. 1 Despite the advances in internal fixation devices and surgical techniques, intertrochanteric hip fractures are still associated with a high frequency of transfusions. 2 Allogeneic blood transmission is essential for hemodynamic stability, but it can cause hematogenic infection, deep vein thrombosis, impairment in coagulation status, and immunosuppression after surgery, which may increase mortality and morbidity in patients with intertrochanteric hip fractures.3–6 For this reason, surgeons are trying to reduce the frequency of allogeneic blood transfusions by treatment strategies such as autologous transfusion, erythropoietin, tranexamic acid, and iron supplementation before surgery.7–12 As a result, the frequency of allogeneic transfusions after surgery has steadily decreased. However, these strategies are difficult to apply to all patients in terms of cost-effectiveness. Therefore, we conducted this study to evaluate the risk factors that increased the frequency of blood transfusions in patients with intertrochanteric hip fractures to determine the risk before surgery and to take selective precautionary measures in the high-risk transfusion group so that surgery can be performed safely.
Materials and methods
Patient population
We conducted a retrospective study of patients who underwent surgical fixation of their intertrochanteric fracture by a single surgeon in our hospital from January 2015 to December 2020. Of 335 patients who had surgery from 2015 to 2020, 203 patients were included in the study. Patients with multiple fractures, gastrointestinal bleeding, those taking antithrombotic agents, who had blood transfusions before and during surgery, and those who underwent surgery more than one week after injury were excluded (Figure 1).

Flow chart of the patients.
Surgical techniques
Among 203 subjects, 44 subjects with stable fractures were managed with a dynamic hip screw (DHS) (4CIS CHS System®; Solco Inc., Pyeongtaek, Korea), and 159 subjects with unstable fractures were managed with a DHS with an additional trochanteric stabilization plate (TSP) (Figure 2). The type of hip fracture (stable/unstable) was documented based on a review of preoperative and postoperative radiographs. An unstable fracture was defined by satisfying the criteria of Gargan et al. 13 (four-part fracture, medial cortical comminution, reverse obliquity, subtrochanteric extension, and large posterior trochanteric fragment). The direct lateral approach was used in all cases. A lag screw was inserted in the center of the femoral head, if possible, or was inserted on the posteroinferior side of the femoral head under C-arm fluoroscopic guidance in the anteroposterior and lateral views. Additional wiring was applied at the surgeon's discretion.
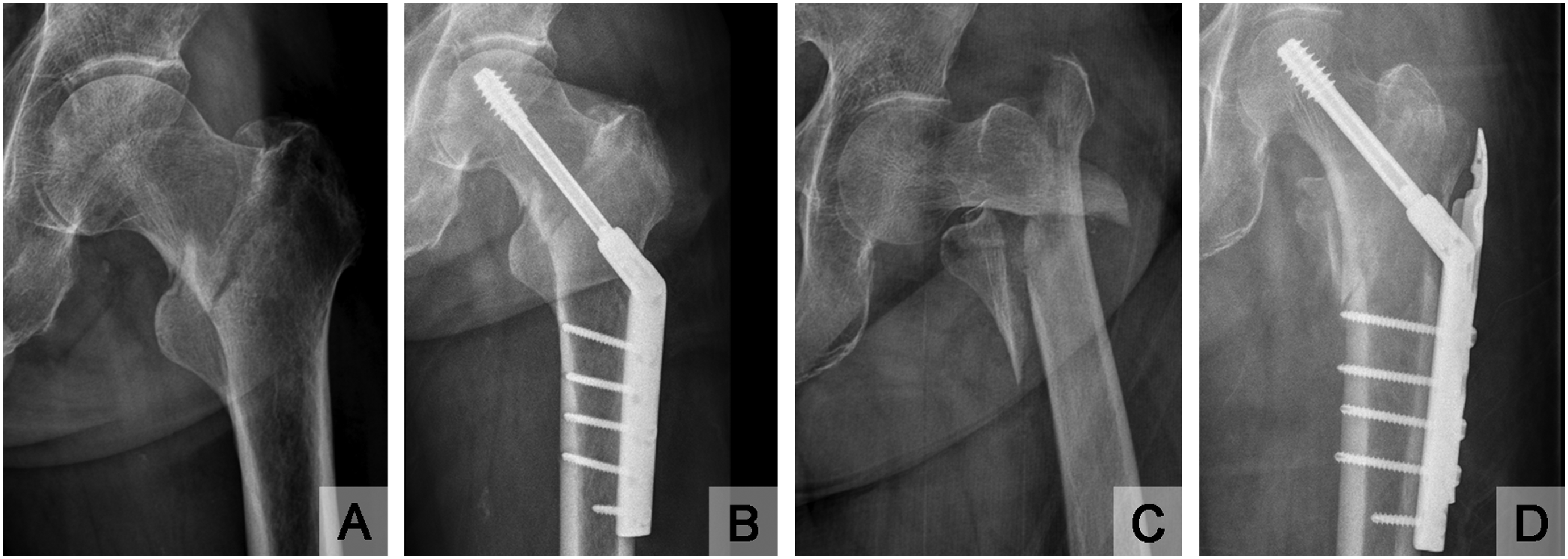
Radiographic hip images.
Blood transfusion analysis
We hypothesized that patient sex, age, body mass index (BMI), preoperative hemoglobin, preoperative platelet count, GFR, preoperative albumin level, American Society of Anesthesiologist (ASA) score, intraoperative blood loss, duration of surgery, method of anesthesia, and time from injury to surgery would affect the need for blood transfusion. These factors were collected from the electronic medical records, and fracture type (stable/unstable) was determined before surgery using a picture archiving and communication system. We counted blood transfusions within three days of surgery. Patients received allogeneic concentrated red blood cell transfusions when their hemoglobin level was less than 8 g/dL or they had symptoms of anemia such as dizziness, chest pain, tachycardia, and persistent hypotension within three days of surgery.14–16 In all patients, thromboembolic prophylaxis was delivered through a pneumatic pump throughout the hospitalization period.
Statistical analysis
All analyses were performed with IBM SPSS version 19.0 software (SPSS Inc., Chicago, IL, USA) for windows. We used the Student's t-test for continuous variables and the Chi-squared test for categorical variables. The one-way analysis of variance test was used for categorical variables when more than two categories were used to determine whether the difference between variables in the transfusion and non-transfusion groups was significant. A P-value of less than or equal to 0.05 was considered to indicate statistical significance. A logistic regression analysis was used to assess the relative contributions of patient factors to the frequency of transfusion.
Ethical statement
This trial was conducted with approval from the Institutional Review Board (IRB) of Daegu Catholic University Medical Center (approval number: CR-21-020) and conducted in accordance with local ethical guidelines. A Waiver of Documentation of Consent was granted by the IRB because this was a retrospective study based on medical records and the data obtained were protected in secured storage. This study also has no possibility of benefitting or harming the involved patients.
Results
Demographic characteristics
Patient basic characteristics, including transfusion rates, are presented in Table 1. The average age of the patients was 78.9 years old, with a total of 156 women (mean, 80.7 years old) and 47 men (mean, 74.5 years old). The mean preoperative hemoglobin level was 10.8 g/dL, the preoperative platelet count was 208,000/μL, the albumin level was 3.8g/dL, and the GFR was 73.4 mL/min/1.7m2. Thirty-nine patients had general anesthesia and 164 had spinal anesthesia. There were 44 stable fractures (21.7%) and 159 unstable fractures (78.3%). The mean intraoperative blood loss volume was 143.2 mL. The mean duration of surgery was 60.3 min and the time from injury to surgery was 97.9 h. Ninety-three subjects (45.8%) had blood transfusions after surgery.
Basic characteristics of all participants.

Abbreviation: N = number, F = female, M = male, GFR = glomerular filtration rate.
Univariate analysis
Unstable fractures (P = 0.002), general anesthesia (P = 0.028), lower preoperative hemoglobin levels (P < 0.001), and lower GFRs (P < 0.001) were identified as related to blood transfusions in univariate analysis.
Age (P = 0.447), sex (P = 0.109), BMI (P = 0.323), preoperative platelet count (P = 0.906), preoperative albumin level (P = 0.905), ASA score (P = 0.090), intraoperative blood loss (P = 0.378), duration of surgery (P = 0.093), and time from injury to surgery (P = 0.206) were not statistically significant.
Multivariate logistic analysis
The need for allogeneic transfusion was significantly associated with unstable fractures in the multivariate logistic analysis and the risk was approximately 2.949 times higher than in patients with stable fractures (P = 0.009). In general anesthesia patients, the transfusion risk was about 2.953 times higher than in spinal anesthesia patients (P = 0.007). The need for allogeneic transfusion was increased by about 1.293 times for preoperative hemoglobin decreases of 1 g/dL (P = 0.017) and increased by about 1.017 times for GFR decreases of 1 mL/min/1.7m2 (P = 0.006) (Table 2).
Multiple variables logistic regression analysis between transfusion group and non-transfusion group.
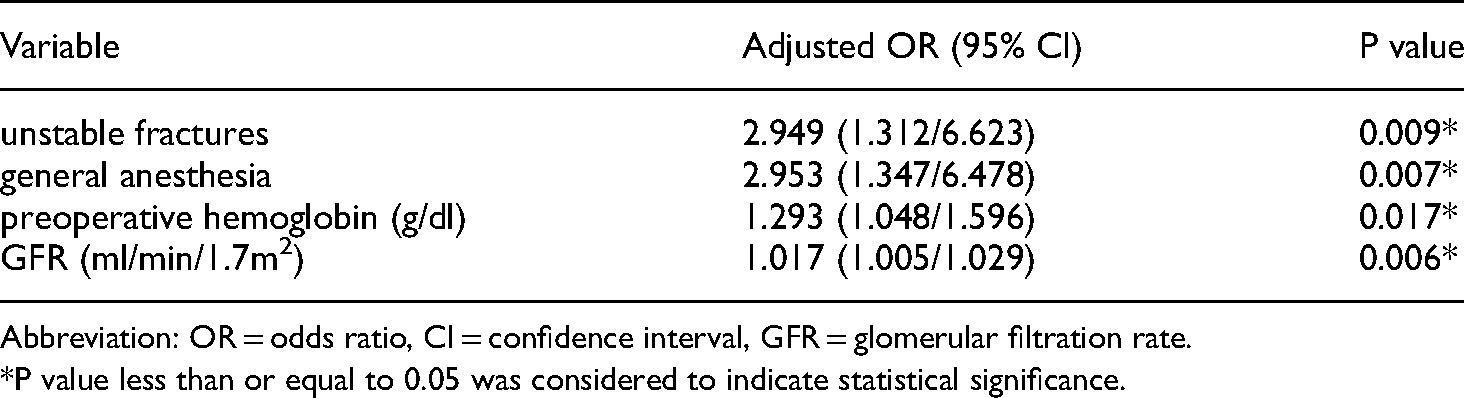
Abbreviation: OR = odds ratio, CI = confidence interval, GFR = glomerular filtration rate.
*P value less than or equal to 0.05 was considered to indicate statistical significance.
Discussion
In elderly patients with intertrochanteric fractures, complications such as cardiovascular and pulmonary complications, infections, bleeding, and thrombosis can lead to death. In particular, perioperative anemia caused by bleeding from these fractures is a common complication and is highly associated with mortality,17,18 so surgeons want to address anemia with blood transfusions. Several studies have reported that the frequency of perioperative allogeneic blood transfusions in patients with senile hip fractures was 30 to 70%.19,20 In elderly patients with intertrochanteric fractures, many factors can affect blood transfusion frequency, and not many studies have systematically studied the risk factors for blood transfusion. Therefore, we conducted this study to predict high-risk patients by retrospectively evaluating the blood transfusion risk of patients after osteosynthesis using a DHS in elderly patients with intertrochanteric fractures.
In our study, among numerous factors, preoperative hemoglobin levels, GFRs, anesthesia methods, and fracture types (stable/unstable) were shown to be associated with the frequency of transfusion.
Several studies have already shown that the lower the preoperative hemoglobin level, the higher the frequency of transfusions.21–23 Our study found statistically significant differences in preoperative hemoglobin levels in patients receiving postoperative blood transfusions (10.36 ± 1.51 g/dL) and in patients without blood transfusions (11.26 ± 1.53 g/dL) (P < 0.001). In multivariate logistic analysis, the risk of transfusion increased by about 29% when the preoperative hemoglobin level decreased by 1 g/dL (P = 0.017).
The study also found that the lower the GFR level, the higher the frequency of transfusions. Lejus et al. 24 found that moderate-to-severe renal impairment (GFR < 60) was 2.35 times higher in patients with frequent transfusions when calculated using the Modification of Diet in Renal Disease (MDRD) equation. 25 In our study, as GFR decreased by 1 mL/min/1.7 m2, the need for allogeneic transfusion increased by about 1.017 times (P = 0.017). This was associated with an increased risk of bleeding by hemostatic abnormalities due to platelet dysfunction, the impaired release of tissue plasminogen activator (tPA), increased plasminogen activator inhibitor-1, elevated fibrinogen and D-dimer, and increased TF/Factor VIIa ratios in patients with chronic renal impairment. 26
In orthopedic surgery, it is generally reported that regional anesthesia can reduce the requirement for blood transfusion compared to general anesthesia.27–29 A comparative study of hip fracture patients by Fields et al. 30 recently reported that regional anesthesia could reduce the frequency of transfusions compared to general anesthesia, suggesting that regional anesthesia is advantageous in older patients with hip fractures. Regional anesthesia is considered to lower regional arterial and venous flow pressure, causing less bleeding and thus, requiring less transfused blood. In this study, the risk of transfusion in general anesthesia patients was about 2.953 times higher than in spinal anesthesia patients, which was statistically significant (P = 0.007). In general, anesthesia methods in surgery for elderly patients with hip fractures are mostly determined by the patient's co-morbidities, surgeon preferences, and the ability of anesthesiologists. However, based on this study, spinal anesthesia was considered to have a significant advantage in reducing the frequency of transfusions.
There were several limitations to this study. First, the results could be affected by excluding the group of patients who received blood transfusions before and during surgery. In our study, we wanted to determine the frequency of postoperative blood transfusions, and it was not expected to have a significant impact because few patients received blood transfusions before and during surgery. Second, the transfusion risk was higher in patients with unstable fractures than in those with stable fractures. It was unclear whether the fracture type influenced it or whether the treatment methods (DHS versus DHS with a TSP) affected it. However, since fixing with a DHS and TSP is a currently established rationale for unstable fractures, it can be concluded that the risk differed depending on the fracture type. Third, although proximal femoral nails have been more widely used in the treatment of unstable intertrochanteric fractures, DHSs and TSPs were used in this study. The surgeon in this study still advocates for the DHS fixation method, which has many advantages. Also, the DHS fixation method is familiar to the operator, which he uses for most intertrochanteric fractures.
This study found that low preoperative hemoglobin levels, low GFRs, general anesthesia, and unstable fractures in elderly patients with intertrochanteric fractures increased the risk of blood transfusion. In conclusion, our study evaluated the risk factors that affected the blood transfusion rate of patients with intertrochanteric hip fractures, which can enable the use of selective, preoperative precautionary measures for patients with these risk factors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Myung-Rae Cho is Professor Orthopaedics at Daegu Catholic University. He received his MD from Kyungpook National University, school of medicine and received his master’s degree and PhD in Orthopedics from Kyungpook National University. He has published widely on Arthoplasty, Hip and Pelvic fracture.
Young-Jae Cho is resident at Daegu Catholic University. He received his MD from Chonbuk National University School of Medicine.
Suk-Kyoon Song is an Assistant Professor of Orthopaedics at Daegu Catholic University. He received his MD from Daegu Catholic University, school of medicine and received his master’s degree in medicine from Kyungpook National University, school of medicine, and undergoing PhD in Orthopedics from Daegu Catholic University. He has published widely on Arthoplasty, Hip and Pelvic fracture, Osteoporosis and Sarcopenia.