
Abstract
Objective
To explore the latent profile classification of dyspnea catastrophizing in elderly patients with chronic obstructive pulmonary disease (COPD) and its relationship with emotional-social loneliness.
Methods
A total of 287 elderly patients with COPD were prospectively and consecutively recruited from five respiratory wards of the Respiratory Center at the Sixth People's Hospital of Nantong between October 2024 and April 2025. This cross-sectional study assessed dyspnea catastrophizing cognition and emotional-social loneliness using the Breathlessness Catastrophizing Scale and the emotional-social loneliness inventory. Latent profile analysis was conducted to identify potential categories of catastrophizing. Multivariate analysis of variance and generalized linear model (GLM) were used to examine the differences in emotional-social loneliness among different types of patients and the robustness of the grouping effect.
Results
The categorization of dyspnea catastrophization can be divided into three distinct profiles: C1, the “Catastrophic-Fixation Group” (18.1%), C2, the “Vigilant-Fear Group” (50.9%), and C3, the “Adaptive-Management Group” (31.0%). These three groups of patients exhibited graded differences across each dimension of emotional-social loneliness, with C1 and > C2 >showing greater differences than C3 (P < 0.001). Notably, the dimension with the greatest difference was social isolation (Δ = 10.0 points). After controlling for confounding variables using the GLM, the catastrophizing subtype still independently accounted for 21%–26% of the variance in loneliness (η²p = 0.21–0.26, P < 0.001).
Conclusion
There is significant variability in the catastrophizing cognition of dyspnea among elderly patients with COPD. The three latent profiles are progressively associated with emotional-social loneliness, offering a targeted foundation for precise psychological interventions.
Keywords
Introduction
Dyspnea, a core symptom of chronic obstructive pulmonary disease (COPD), not only causes physical distress but also triggers complex psychological and cognitive responses.1,2 This includes dyspnea catastrophizing, where individuals interpret their dyspnea in catastrophic terms, such as “I might suffocate to death” or “This feeling will never be controlled,” which has been shown to amplify the subjective symptom experience, accelerate lung function decline, and significantly reduce patients’ quality of life. 3 Studies indicate4,5 that COPD patients with high levels of catastrophizing have a 12% increased risk of emergency department visits, and are associated with higher rates of depression and mortality. However, much of the existing research treats catastrophizing as a uniform construct, neglecting the potential for varied cognitive response patterns among patients.
At the same time, elderly patients with COPD face unique emotional and social dilemmas. 6 The decline in physiological function and the change in social role make them more susceptible to a multi-dimensional dilemma of emotional isolation (lack of emotional connection), social isolation (limited social participation), emotional loneliness (desire for intimate relationships), and social loneliness (perceived alienation in relationships).7,8 This complex state of loneliness has been shown to be directly related to an increased risk of acute exacerbation of COPD and decreased treatment adherence.9,10 It is noteworthy that catastrophizing cognition and emotional-social loneliness may form a two-way vicious cycle. Catastrophizing thinking exacerbates patients’ social avoidance, while the lack of emotional support further intensifies their fear of symptoms. 11 This cycle is particularly pronounced in older COPD populations with limited access to resources. 12
Previous research has several important limitations. Most existing literature employs regression or structural equation models and treats catastrophization as a single continuous variable,5,13 which makes it challenging to capture the heterogeneous subtypes within the patient population. Many studies measure overall loneliness without differentiating between isolation and loneliness in the emotional or social dimensions. 14 There is also a deficiency in the in-depth analysis of the “cognitive-emotion” interaction among the elderly, particularly the basis for targeted interventions tailored to the characteristics of subgroups. 15 Latent profile analysis (LPA) offers a new approach to address these challenges. By identifying latent subtypes within a population, LPA can uncover heterogeneity patterns that traditional methods may obscure.
This study introduces LPA into the field of geriatric COPD research, utilizing culturally adapted and validated measures—the Breathlessness Catastrophizing Scale (BCS) and the four-dimensional Emotional–Social Loneliness Inventory (ESLI). It aims to achieve two primary objectives: first, to identify the latent subtypes of dyspnea catastrophizing cognition among elderly COPD patients; and second, to examine the differential patterns of these catastrophizing subtypes across four dimensions of loneliness—emotional isolation, social isolation, emotional loneliness, and social loneliness. Notably, it is essential to explore the possibility that dyspnea catastrophizing cognition and emotional–social loneliness may form a specific vicious cycle in elderly COPD patients. Catastrophizing is not merely a negative emotional state but can directly trigger maladaptive behaviors—such as avoiding social situations due to fear of dyspnea attacks in public, or refraining from seeking emotional support for fear of becoming a burden. 16 These behaviors further impair the quality and scope of patients’ social connections, manifesting prominently as social loneliness and social isolation. The resulting lack of social support, in turn, diminishes patients’ psychological resources for coping with symptoms, thereby intensifying feelings of loss of control and fear related to dyspnea and reinforcing catastrophizing cognition. 17 This cycle is particularly destructive in older adults who already experience declining physical function and fragile social networks.
Therefore, moving beyond generalized research on “catastrophizing” or “loneliness,” precisely elucidating the interactive mechanisms within this cycle is a critical prerequisite for developing effective psychological interventions. Against the backdrop of a rapidly aging population and the increasing disease burden of COPD, 18 the findings of this study are expected to provide an empirical basis for formulating precise, subtype-specific psychosocial intervention strategies. This will significantly advance the implementation of integrated “biopsychosocial” care models in the field of geriatric respiratory health.
Subjects and methods
Subjects
In this study, LPA was employed to investigate the relationship between subtypes of dyspnea catastrophization and emotional-social loneliness. Given that LPA lacks a conventional sample size formula, it is essential to verify the differences in loneliness scores among the subtypes through core hypothesis testing. Following methodological recommendations,
19
the correlation coefficient test between key variables served as the foundation for calculating the sample size. The sample size formula, based on correlation tests between variables, is as follows:
The study was approved by the Ethics Committee of the Sixth People's Hospital of Nantong (Approval No: NTLYLL2024061; Date of Approval: 4 September 2024). All patients provided informed consent. The reporting of this study conforms to STROBE guidelines. 23
Methods
Survey tools
General information questionnaire. The table was designed by referring to relevant literature and expert consultation, mainly including ① general demographic data: gender, age, education level, BMI, and economic burden; ② Disease characteristics: duration of COPD, GOLD stage, and number of acute exacerbation hospitalizations in the past year; ③ Psychosocial resources: frequency of social activities and mobile phone use ability.
Emotional-social loneliness psychological assessment. The Emotional-Social Loneliness Questionnaire (ESLI) was used for evaluation, which was developed by Vincenzi and Grabosky, 24 including four dimensions of emotional isolation, social isolation, emotional loneliness, and social loneliness, with a total of 30 items. The Likert 0-3 scoring method was used for each item, and dimension scores were positively correlated with the severity of loneliness/isolation. The clinical cut-off values were set as follows: isolation score ≤8 was defined as no isolation, 9–12 as isolation, and ≥13 as severe isolation. A loneliness score ≤10 was defined as no loneliness, 11–14 as loneliness, and ≥16 as severe loneliness. The Cronbach's α coefficient of ESLI was 0.964, which had good reliability and validity. Permission has been obtained from the copyright owner for this questionnaire.
Catastrophization assessment of dyspnea. The Dyspnea Catastrophizing Cognitive Scale (BCS) was utilized to assess the outcomes. Adapted by Solomon et al. 25 from the Pain Catastrophizing Scale, it is a unidimensional self-assessment tool comprising 13 items designed to evaluate patients’ cognitive responses to dyspnea episodes. Responses were rated on a 5-point Likert scale, ranging from 0 (“never”) to 4 (“always”). The total score spanned from 0 to 52, with higher scores indicating a greater severity of catastrophizing cognition. In this study, the Chinese version of the BCS was employed to validate the psychometric properties of the scale in 330 COPD patients. The Cronbach's α coefficient was 0.96, the Spearman-Brown coefficient was 0.89, and the test-retest reliability was 0.90. 26 Permission has been obtained from the copyright owner for this questionnaire.
Statistical methods
In this study, SPSS 27.0 was utilized for data management and conducting basic statistical analyses, while Mplus 8.3 was employed for latent profile modeling and validation. A two-tailed P-value of < 0.05 was adopted as the threshold for statistical significance across all hypothesis tests. (1) Measurement data: variables that followed a normal distribution were presented as mean ± standard deviation, with normality confirmed through the Kolmogorov-Smirnov test (P > 0.05). Enumeration data were detailed by the count and percentage of cases, and missing data were handled appropriately. Items from key scales (BCS/ESLI) with more than 10% missing data were excluded, affecting a total of nine cases. The remaining missing values were processed using the chain equation multiple imputation method (MICE). Pearson correlation analysis was employed to assess the correlation between the total score of the BCS and the four dimensions (emotional isolation, social isolation, emotional loneliness, and social loneliness) of the ESLI. The Bonferroni method was employed to correct for multiple comparisons. Utilizing the 13 items of the BCS scale as the key variables, the latent profile model was incrementally fitted across one to five categories. The optimal model was defined by the following criteria: ① entropy > 0.8; ② bootstrap likelihood ratio test (BLRT) or Lo-Mendell-Rubin likelihood ratio test (LMR) P-value <0.05; ③ the lowest Bayesian information criterion (BIC) value. 24 Pillai's Trace statistic was utilized. When multivariate analysis of variance (MANOVA) indicated significance (P < 0.05), one-way analysis of variance (ANOVA) was conducted to calculate partial eta squared, with values >0.01 considered a small effect, >0.06 a moderate effect, and >0.14 a large effect. A generalized linear model (GLM) was constructed to assess the robustness of the validation group effect, with the ESLI dimension as the dependent variable, modeled as follows: ESLI dimension = β0 + β1 (grouping from LPA) + β2 (age) + β3 (GOLD status) + β4 (number of exacerbations) + ɛ, with the sum of squares evaluated using Type III tests for significant main effects.
An exploratory factor analysis was conducted on a total of 43 items from the BCS (13 items) and ESLI (30 items) using the Harman single-factor method. The results indicated that the first factor accounted for 28.7% of the variance, which is below the critical value of 40%, suggesting that there was no significant common method bias in this study. To ensure patient privacy and confidentiality, all participant identifiers were removed from the dataset during the data analysis phase. The analyzed data were completely anonymized.
Results
General information survey results
A total of 287 valid questionnaires were collected for this study, with an average age of 70.21 ± 4.33 years. There were 172 males (59.9%) and 115 females (40.1%). See Table 1 for further details.
General characteristics of the study subjects (n = 287).

BMI: body mass index; COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Lung Disease.
Descriptive statistics and related results analysis
Person correlation analysis revealed that dyspnea catastrophizing was positively correlated with all dimensions of emotional-social loneliness (r = 0.43−0.61, P < 0.01), with the strongest correlation observed with emotional loneliness. There was a significant correlation between each dimension of emotional-social loneliness (r = 0.51−0.68, P < 0.01), and the correlation between emotional isolation and social isolation was the highest. All correlation coefficients indicated medium and above effect sizes, as detailed in Table 2.
Descriptive statistics and correlation analysis of dyspnea catastrophizing and emotional-social loneliness (n = 287).
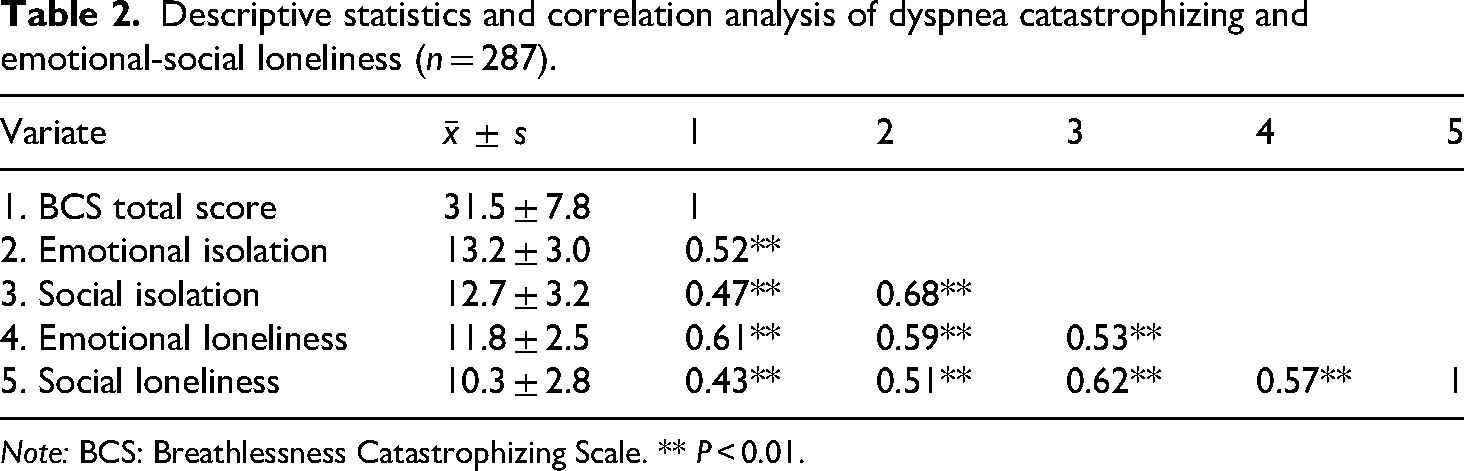
Note: BCS: Breathlessness Catastrophizing Scale. ** P < 0.01.
Potential profile analysis of dyspnea catastrophizing
To determine the optimal number of latent profiles, models with one to four classes were sequentially estimated. While the four-class model demonstrated marginally lower AIC and aBIC values, the three-class solution was retained as optimal based on a combination of statistical and substantive criteria. The three-class model showed a statistically significant improvement over the two-class model, as indicated by significant LMR-LRT and BLRT values (P < 0.05). In contrast, the four-class model did not yield a significant improvement over the three-class solution (P > 0.05). Furthermore, the three-class model exhibited higher entropy (0.912) compared to the four-class model (0.855), reflecting superior classification accuracy. Finally, the four-class model produced one small class comprising only 9.2% of the sample, which raised concerns regarding its stability and clinical interpretability. The three-class solution, with its well-proportioned classes and clear gradient of catastrophizing severity, was therefore selected for its statistical adequacy, classification precision, and clinical meaningfulness, as shown in Table 3.
Fit indices of the latent profile model for dyspnea catastrophizing (n = 287).
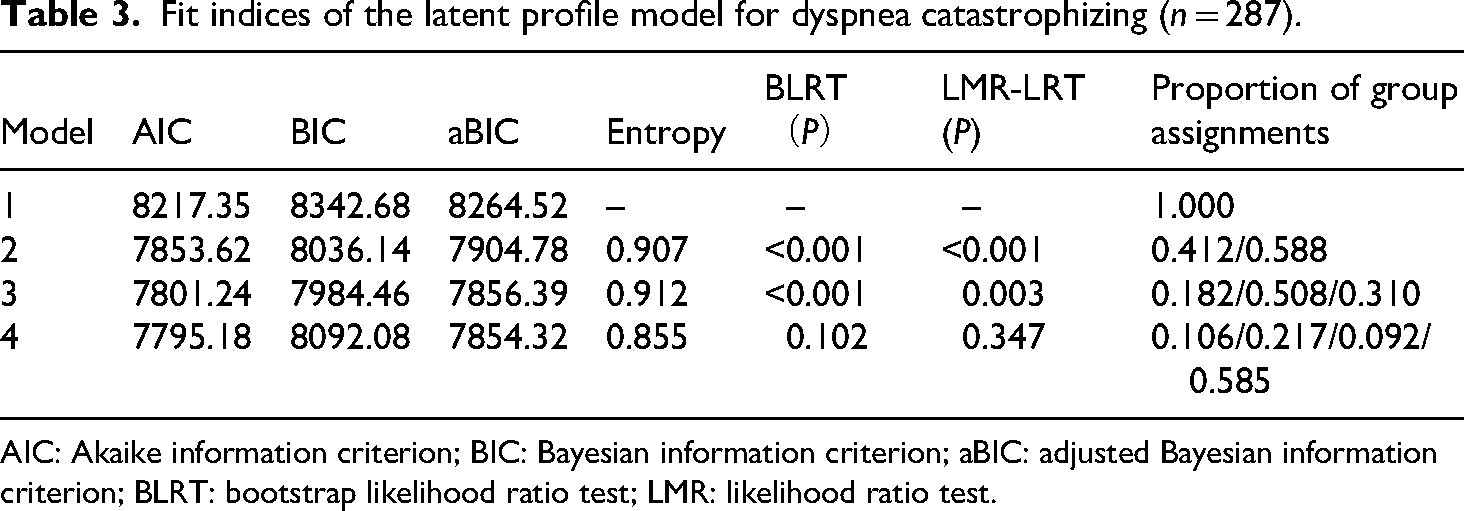
AIC: Akaike information criterion; BIC: Bayesian information criterion; aBIC: adjusted Bayesian information criterion; BLRT: bootstrap likelihood ratio test; LMR: likelihood ratio test.
Probability distribution and nomenclature of catastrophization of dyspnea
In this study, the average probability of subjects being classified into the three latent types was calculated, and the results are presented in Table 4. The primary class attribution probability for individuals in Class 1 was 0.981, with a cross-class contamination probability of <0.019. For Class 2, the primary class attribution probability was 0.973, and all non-target class probabilities were <0.022. The primary class attribution probability for Class 3 was 0.978. Other class probabilities were all <0.001, and the primary class attribution probability for all individuals exceeded 0.97, which satisfied the Nylund criterion. 27
Distribution of potential class attribution probability (n = 287).

Class 1 exhibited cognitive fixation and absolute helplessness on item 9 (inability to divert attention from symptoms) and item 12 (lack of effective methods), earning the label of catastrophic-fixation group. The average score for Class 2 on item 3 (worry about asphyxia) and item 13 (fear of bad occurrences) exceeded 2.9, suggesting a dominant disaster expectation. Consequently, based on the fear avoidance model of cognitive psychology, 28 Class 2 was designated as the vigilant-fear group. Class 3 had the lowest BCS score, with item 8 (“desire to be symptom-free”) scoring 1.3, indicating an active management motivation. Therefore, Class 3 was named the adaptive-management group. The distribution of scores for potential types of dyspnea catastrophizing across the 13 items is depicted in Figure 1.

Mean scores of the three potential categories of dyspnea catastrophizing across 13 items.
Differences in BCS theoretical subscale scores across the three latent classes
The one-way ANOVA results (presented in Table 5) indicated statistically significant differences among the three latent classes across all three theoretical subscales of the BCS: helplessness (F = 285.6, P < 0.001), rumination (F = 301.2, P < 0.001), and magnification (F = 198.4, P < 0.001). Post-hoc tests revealed that the catastrophic-fixation group scored significantly higher than both the vigilant-fear and adaptive-management groups on all three subscales (all pairwise comparisons P < 0.001). Furthermore, the vigilant-fear group scored significantly higher than the adaptive-management group (P < 0.001). Specifically, the catastrophic-fixation group obtained the highest mean scores on the subscales, the adaptive-management group obtained the lowest, and the vigilant-fear group scored intermediately. These results demonstrate a clear severity gradient, confirming that the empirically derived latent profile classification not only has a solid empirical basis but also aligns strongly with the core theoretical constructs of dyspnea catastrophizing.
Validation of latent profiles on BCS theoretical subscales.
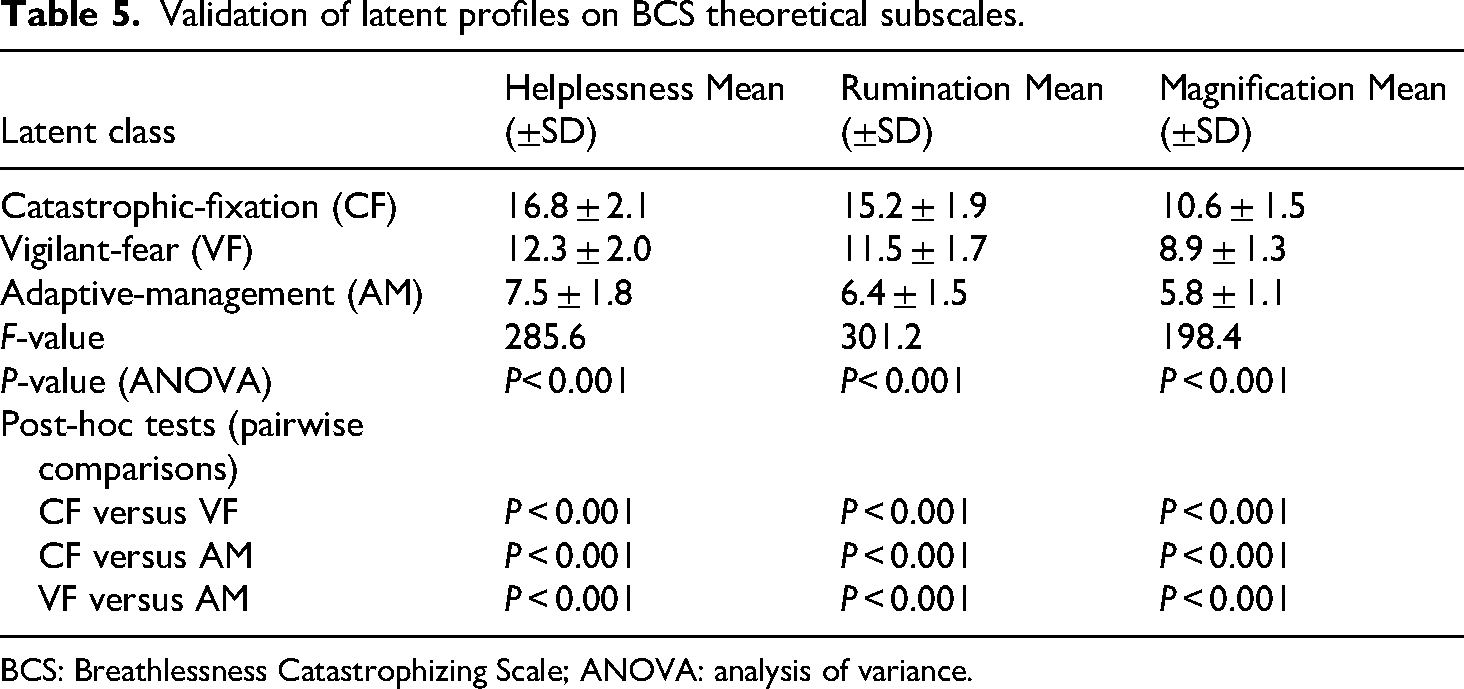
BCS: Breathlessness Catastrophizing Scale; ANOVA: analysis of variance.
The distribution of potential categories of dyspnea catastrophizing among different elderly patients with COPD in terms of demographic variables
The potential categories of dyspnea catastrophization were tested across various demographic data (Table 6), revealing statistically significant differences among the groups in terms of gender, age, education level, GOLD classification, acute exacerbation hospitalization, frequency of social activities, and ability to use mobile phones (P < 0.05). The proportion of males in the catastrophic-fixation group (73.1%) was significantly higher than that of females (26.9%), whereas the proportion of females in the adaptive-management group (43.8%) was higher than that of males (56.2%). The proportion of elderly patients (>75 years old) was highest in the catastrophic-fixation group (57.7%), significantly exceeding that of the vigilant-fear group (46.6%) and the adaptive-management group (41.6%). The catastrophic-fixation group had the highest proportion of moderate to very severe patients (46.2%), and 84.6% of patients experienced ≥2 acute exacerbations per year, a rate significantly higher than that of other groups. Patients with no social activities per month accounted for the highest proportion (76.9%) in the catastrophic-fixation group, and the proportion of patients with no ability to use mobile phones was significant (53.8%) in the catastrophic-fixation group. Patients with a primary school education or below accounted for the highest proportion of the catastrophic-fixation group (69.2%).
Distribution of various potential categories of dyspnea catastrophizing across demographic variables.

GOLD: Global Initiative for Chronic Obstructive Lung Disease.
The differences in the catastrophization of dyspnea among different potential categories
The MANOVA analysis of 287 patients revealed Wilks’ λ = 0.58, F(8562) = 26.84, P < 0.001, and a multivariate η²p of 0.28 (95% CI: 0.24–0.32). Univariate analysis indicated significant differences across all dimensions (P < 0.001). Post-hoc tests with Bonferroni correction demonstrated that all dimensions of emotional-social loneliness significantly differed among the three patient types (P < 0.001). The catastrophic-fixation group exhibited the highest scores in emotional isolation (18.7 ± 2.9) and social isolation (18.5 ± 3.1), whereas the adaptive-management group had the lowest scores, with a difference ranging from 8.0 to 10.0 points (P < 0.001). For further details, refer to Table 7 and Figure 2.
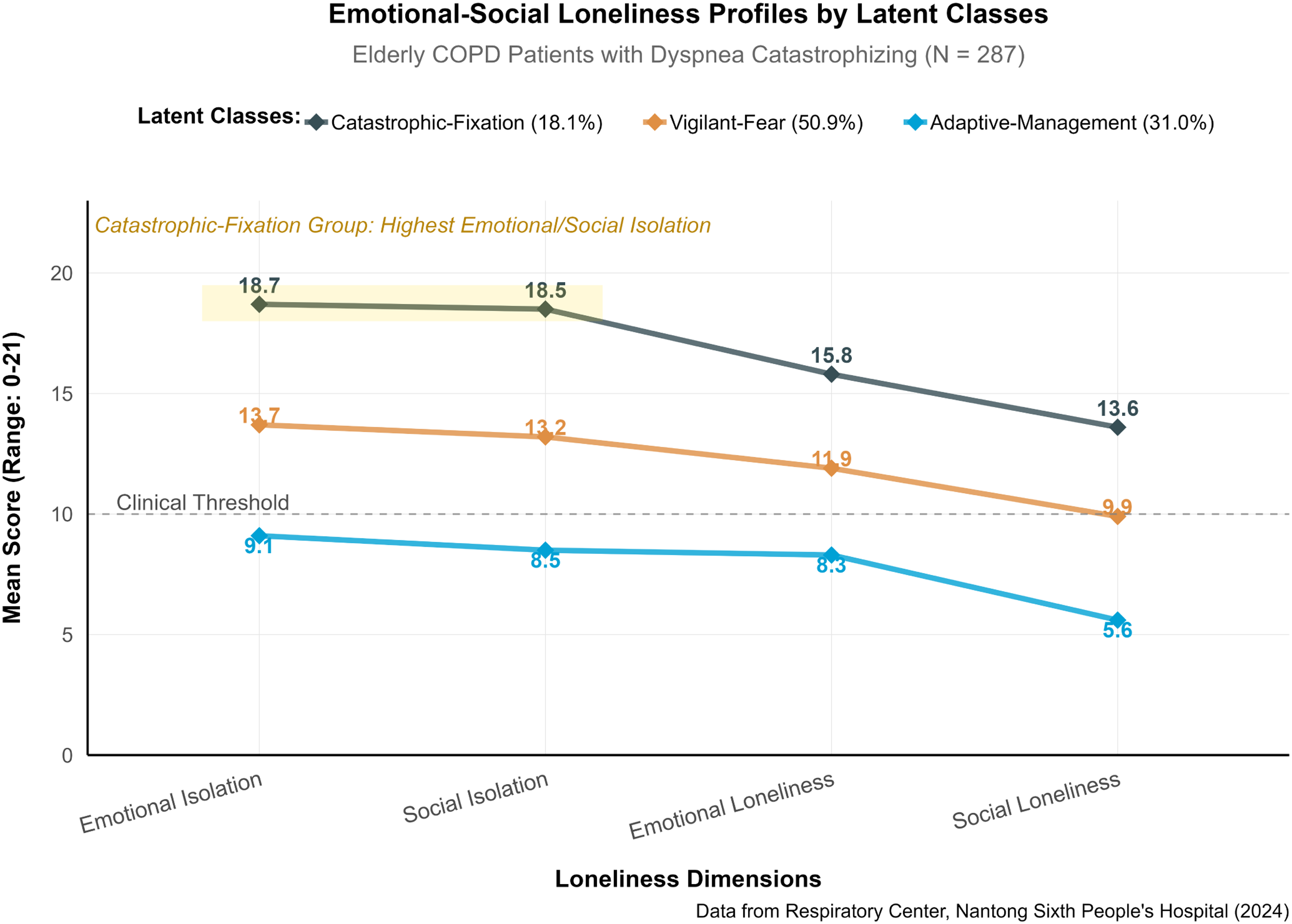
Emotional-social loneliness profiles by latent classes.
Test and comparison of emotional-social loneliness scores of patients with different types of dyspnea catastrophization (

Note: *** P < 0.001.
Robustness check of group effects in GLMs
To control for the influence of confounding factors, a GLM was used to examine the independent effect of potential subgroups of dyspnea catastrophizing on emotional-social loneliness. The model was constructed as follows: ESLI dimension = β₀ + β₁ (LPA subgroup) + β₂ (age) + β3 (GOLD grade) + β₄ (number of exacerbations) + ε. Type III sum of squares was used to assess the significance of the main effects, and the results are presented in Table 8. After controlling for age, disease severity, and exacerbation frequency, the LPA subgroup still had a significant main effect on all dimensions of loneliness (P < 0.001). The GLM analysis confirmed that the subgroup of dyspnea catastrophizing was a strong predictor of emotional-social loneliness, and its effect was independent of GOLD grade and exacerbation frequency.
Prediction effects of GLM on emotional and social loneliness (Type III SS).
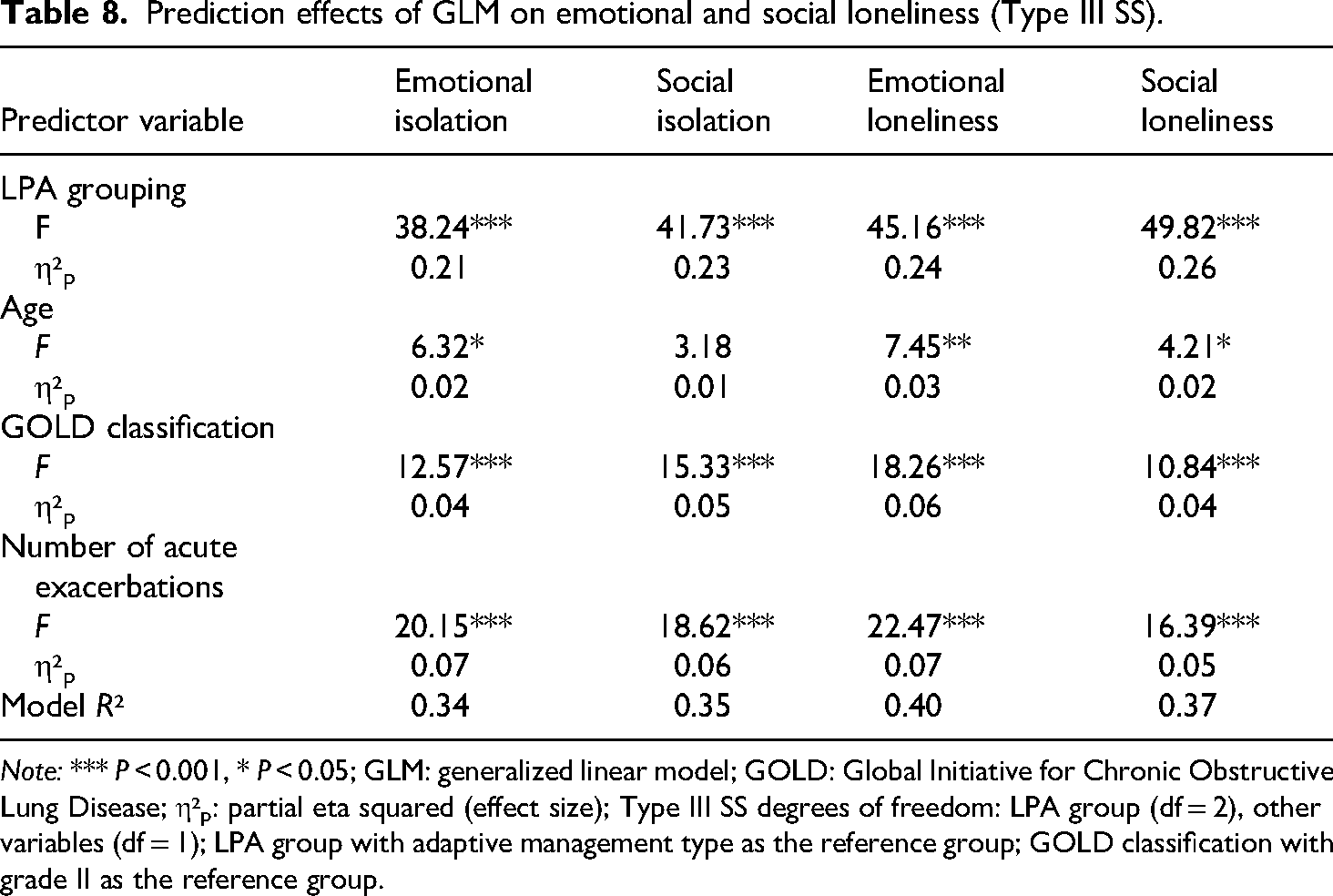
Note: *** P < 0.001, * P < 0.05; GLM: generalized linear model; GOLD: Global Initiative for Chronic Obstructive Lung Disease; η²p: partial eta squared (effect size); Type III SS degrees of freedom: LPA group (df = 2), other variables (df = 1); LPA group with adaptive management type as the reference group; GOLD classification with grade II as the reference group.
Discussion
This study focused on the elderly population with COPD in China. Employing a multi-dimensional data analysis system, it explored the prevalence characteristics, heterogeneous profiles, and mechanisms influencing dyspnea catastrophization. The key findings not only provided localized evidence for understanding the psychopathological characteristics of this demographic but also established a theoretical foundation and practical framework for clinical practice and public health decision-making.
Dyspnea catastrophizing is a significant cognitive bias in the psychological adjustment process of COPD patients, with its prevalence and manifestations varying considerably across regions and populations. This study, for the first time, confirmed through a large sample survey that the overall score of dyspnea catastrophizing among elderly COPD patients in China was 31.5 ± 7.8, higher than the 28.0 score reported by domestic scholars. 29 The elevated state of respiratory catastrophizing in this study is not isolated but results from the interaction of multiple factors, including unique physiological-psychological-social mechanisms. From a physiological standpoint, 56.1% of the patients with GOLD III–IV levels in the sample, and 36.6% of those experiencing ≥2 acute exacerbations annually, exhibited a significant negative correlation between lung function indices and the catastrophizing score. This suggests that a severe decline in lung function may directly induce catastrophizing cognition by continuously amplifying physical signals. 30 This finding aligns with the conclusion of a positive correlation between “symptom intensity and catastrophizing degree” from foreign studies, 5 potentially related to the increased perception sensitivity of elderly patients to physical changes with age. 31 This is further compounded by weak social support systems. The study revealed that 35.5% of patients lacked regular social activities, and 22.7% were completely unable to use smart terminals. This digital divide made it challenging for patients to access disease management information and to alleviate anxiety caused by symptoms through social interaction, creating a vicious cycle of “symptom fear, social withdrawal, and information occlusion.” 32 The role of cognitive aging cannot be overlooked.33,34 In this study, 28.2% of the patients were over 75 years old, indicating that the decline in cognitive regulation due to advanced age may impair the patients’ ability to interpret dyspnea rationally. The dyspnea catastrophizing in elderly COPD patients in China exhibits the characteristics of “three highs”: high prevalence, high physiological correlation, and high social vulnerability. This not only encompasses commonalities consistent with the global trend 35 but also features the “three highs.” It also highlights the distinctiveness of the superposition of “multiple chronic diseases + digital divide + cognitive aging” in the aging process of China.36,37
Most traditional studies have regarded catastrophizing of dyspnea as a single-dimensional cognitive bias. However, this study identified three distinct patterns through LPA, namely, the catastrophic-fixation group (18.1%), the vigilant-fear group (50.9%), and the adaptive-management group (31.0%). The core feature of the catastrophic-fixation group is the inability to shift attention away from dyspnea, and its neural mechanism may be related to the dysregulation of the prefrontal cortex—amygdala circuit. 38 Relevant fMRI data indicate that the functional connectivity strength between the dorsolateral prefrontal cortex (DLPFC) and the amygdala in this subtype during symptom imagination tasks is significantly lower than that of normal individuals, 39 suggesting that the prefrontal cortex's regulation of the emotional center is compromised, resulting in patients being caught in a continuous monitoring of symptoms. The cognitive characteristic of the vigilant-fear group is an excessive sensitivity to interoceptive signals, and its neural basis may be related to the excessive activation of the insula, which may lead patients to interpret minor physical discomfort as a signal of “deteriorating condition.” 40 At the behavioral level, the frequency of social activities of this subtype of patients has decreased compared to before the onset of the disease, and avoidance of going out is particularly prominent, which is highly consistent with the “fear–avoidance” model's path of “overinterpretation of somatic signals–behavioral withdrawal.” 41 The adaptive-management group patients exhibit strong cognitive regulation ability. At the behavioral level, this subtype of patients can effectively use self-management strategies such as abdominal breathing, providing empirical support for understanding the positive path of “cognitive resilience–disease adaptation.” This classification model breaks through the limitations of the traditional “single-dimensional scoring” and provides a theoretical basis for subsequent precise intervention.
This study revealed that patients with catastrophic-fixation exhibited a significant clustering of seven vulnerability traits, suggesting that physiological, cognitive, and social factors do not operate independently but instead create a malignant feedback loop through their dynamic interplay. Advanced age (57.7%) results in diminished cognitive regulatory functions in the prefrontal cortex, 42 coupled with a health information decoding impairment due to a low level of education (69.2% or less than primary school education), 43 which together diminish the patient's capacity for rational cognitive processing of dyspnea and predispose them to interpret symptoms as life-threatening. Patients with GOLD IV (46.2%) and a persistent symptom burden, along with frequent acute exacerbations (84.6%) and traumatic memories, 44 experienced intensified catastrophizing thoughts via amygdala sensitization and PTSD-like responses. Social isolation (76.9% lacking social interaction) and digital rejection (53.8% not using mobile phones) further severed social support networks, thereby exacerbating the feeling of loss of control.45,46 The multi-factorial superposition accelerates the deterioration of patients’ catastrophic cognition and significantly increases the utilization rate of emergency departments and the risk of readmission. Clinical interventions require the implementation of multi-dimensional collaborative strategies for spiral nodes. Neurocognitive training can improve prefrontal function, 47 visualization tools adapted for low-literacy groups, such as cartoon illustrations of symptoms and whistle feedback training, can enhance self-management skills, 48 VR graded exposure therapy can gradually reduce the fear of asphyxiation, 49 and voice AI assistants can bridge the digital divide. The key to breaking this vicious cycle is to build a three-tiered prevention system that includes screening, intervention, and multidisciplinary management, and to implement precise interventions for high-risk groups with three or more vulnerability factors. This model offers a new perspective for understanding the complexity of psychological issues in patients with multiple chronic diseases and provides empirical support for developing differentiated prevention and treatment strategies.
In this study, a generalized linear model was employed to verify the difference analysis among groups of patients experiencing emotional and social loneliness. This systematically uncovered the graded association and independent impact between cognitive classification of catastrophization and emotional-social loneliness. The findings indicated that the three patient groups exhibited a strict gradient of “CF > VF > AM” in terms of emotional and social loneliness (P < 0.001). Moreover, the difference in the social isolation dimension was the most pronounced (Δ10.0). All patients diagnosed with the catastrophic-fixation group met the clinical criteria for social isolation, indicating that this subtype necessitates immediate psychological intervention. The catastrophic interpretation of dyspnea (e.g. “fear of suffocation” and “absolute helplessness”) in patients with the catastrophic-fixation profile may directly trigger two key social behavioral patterns: first, active social avoidance—refusing to participate in activities for fear of experiencing embarrassing dyspnea symptoms in social settings; and second, illness-related shame—believing that one's condition will become a burden to others or a topic of discussion, thereby proactively shrinking one's social network. 50 These behavioral patterns directly damage the quantity and quality of their social relationships, leading to a significant reduction in perceived social support and, consequently, the most pronounced disadvantage on the dimension of social loneliness. In contrast, emotional loneliness relates more to internal affective experiences, whose formation may involve deeper personality traits and early life experiences. Social loneliness, however, more directly reflects the immediate impact of current illness-related cognitions and behaviors on social functioning. Therefore, catastrophizing cognition likely influences social loneliness through a more direct pathway, highlighting the urgency of psychological interventions focused on social participation and relationship reconstruction. Even after accounting for physiological factors, such as GOLD classification (η²p = 0.04–0.06) and the frequency of acute exacerbations (η²p = 0.05–0.07), GLM analysis confirmed that catastrophism classification could independently account for 24%–26% of the variance in loneliness. The effect size was significantly greater than that of traditional physiological indicators. The explanatory power (R² = 0.40) was utilized to validate the model's robustness.
This study reveals a key clinical insight: precisely targeted interventions addressing dyspnea catastrophizing cognition may hold greater significance for alleviating loneliness in elderly COPD patients than solely improving pulmonary function. Based on the distinct characteristics of each subtype, we propose a stratified intervention strategy: For the catastrophic-fixation subtype, acceptance and commitment therapy (ACT) combined with cognitive defusion techniques should be employed, focusing on reducing catastrophic associations such as “dyspnea equals a life-threatening threat,” enhancing psychological flexibility, and helping patients detach thoughts from reality to diminish the control of catastrophic thinking over emotions. For the vigilant-fear subtype, virtual reality (VR) graded exposure therapy can be utilized, using controlled scenario exposure to break the “dyspnea → fear → social avoidance” vicious cycle and rebuild a sense of safety and control. For the adaptive-management subtype, the emphasis should be on maintaining and strengthening existing positive coping strategies and social support networks through means such as peer support groups. Therefore, clinical practice should consider incorporating the catastrophizing subtype assessment into the routine comprehensive evaluation system for COPD. This provides a crucial basis for optimizing the precise allocation of psychological intervention resources and advancing an integrated healthcare model from “treating the lung” to “treating the whole person.”
This study has several limitations. First, the sample representativeness is limited. As a single-center study drawing participants from one hospital and focusing primarily on elderly patients, it does not encompass a broader population with varying disease severity or diverse comorbidities (such as comorbid anxiety or heart failure). Therefore, the generalizability of the findings requires further validation. Future research should involve multi-center collaborations across regions such as North China and Western China, including patients with different severity levels and comorbid conditions, to test the external validity of the classification model. Second, the cross-sectional design limits causal inference. While this study reveals associations between dyspnea catastrophizing cognition and emotional-social loneliness, it cannot determine the direction of causality or temporal sequence. For example, does catastrophizing cognition lead to social loneliness, or does social isolation exacerbate catastrophizing thinking? This question warrants further investigation through prospective cohort studies or interventional trials. Third, potential cultural influences on the assessment of loneliness were not fully considered. The scales used in this study were developed within a Western cultural context, whereas expressions of “loneliness” among Chinese elderly may be shaped by traditional cultural beliefs, family expectations, and illness-related stigma. Consequently, certain emotional experiences may not be fully captured by these scales. Future studies could incorporate qualitative interviews to explore the unique connotations of loneliness within the Chinese cultural context more deeply. Finally, this study focused exclusively on elderly COPD patients and did not include middle-aged and younger adults. Thus, it cannot reveal age-related trajectories in the relationship between catastrophizing cognition and loneliness. Subsequent research could expand to include all age groups to explore how the interaction patterns between these two psychological traits evolve across different life stages. Despite these limitations, this study is the first to identify heterogeneous subtypes of dyspnea catastrophizing among Chinese elderly COPD patients and to reveal their specific associations with multidimensional loneliness, providing an important foundation for developing targeted psychological interventions.
Conclusion
This study employed latent profile analysis to categorize the dyspnea catastrophizing cognition among elderly COPD patients, ultimately identifying three distinct latent profiles: the “Catastrophic-Fixation Group,” the “Vigilant-Fear Group,” and the “Adaptive-Management Group.” The three patient groups exhibited a clear gradient across each dimension of emotional and social loneliness, with the catastrophic-fixation group scoring highest in all dimensions. Based on the heterogeneous characteristics of these patient types, a classification intervention strategy was proposed. For the catastrophic-fixation group, cognitive dissociation was used to help break the attention fixation. The vigilant-fear group underwent VR exposure therapy to disrupt the negative cycle, while the adaptive-management group had their community support network strengthened to maintain psychological resilience. It is recommended that dyspnea catastrophizing screening be incorporated into the management screening protocols for COPD in hospitals, and that hospital-community psychological first aid be initiated for elderly, less-educated, and severely affected patients.
Supplemental Material
sj-doc-1-sci-10.1177_00368504251407184 - Supplemental material for The potential profiles of dyspnea catastrophizing and the relationship between emotion-social loneliness in elderly patients with chronic obstructive pulmonary disease
Supplemental material, sj-doc-1-sci-10.1177_00368504251407184 for The potential profiles of dyspnea catastrophizing and the relationship between emotion-social loneliness in elderly patients with chronic obstructive pulmonary disease by Li Feng, Haiyan Ji, Qing-qing Yang and Mengyao Liang in Science Progress
Footnotes
Acknowledgements
We thank the respiratory medicine staff at Nantong Sixth People's Hospital for their assistance.
Ethical approval and consent to participate
The study was approved by the Ethics Committee of the Sixth People's Hospital of Nantong (Approval No: NTLYLL2024061; Date of Approval: 4 September 2024), and all patients had signed written informed consent. All patients provided informed consent. This study was prepared in accordance with the Declaration of Helsinki.
Consent for publication
Written informed consent for all data has been obtained from the patient, who consented to publication.
Authors’ contributions
ML and LF contributed to the design of the study; LF and QY contributed to the manuscript writing; QY and HJ contributed to data collection, analysis, and interpretation; ML reviewed the manuscript and approved the final version of the manuscript. All authors have read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Research Project of Nantong Health Commission (grant no. QN2023044).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant raw data are available by contacting the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.