
Abstract
Objective
An aging or aged society is and has been a reality in many developed countries. Additionally, the incidence of subarachnoid hemorrhage (SAH) in elderly patients has been estimated to be increasing. However, the outcomes of SAH treatment by clipping or coiling in elderly patients are poor. Therefore, preventative surgery for elderly patients with unruptured cerebral aneurysm is becoming increasingly important. The aim of this study was to analyze the safety and efficacy of endovascular coil embolization for elderly patients with cerebral aneurysm.
Methods
A total of 252 patients (264 aneurysms) who underwent endovascular coil embolization for cerebral aneurysms between April 2012 and August 2018 at our institution were included. This study is retrospective observational study, and we retrospectively investigated treatment outcomes and perioperative complications in nonelderly patients and elderly patients with ruptured or unruptured cerebral aneurysms, who underwent endovascular coil embolization. We defined patients aged < 65 years as nonelderly and aged
Results
Among the elderly patients with unruptured aneurysms, there was a higher proportion of cases with residual aneurysm as an embolic state immediately after operation and high-intensity spots in magnetic resonance imaging–diffusion-weighted imaging on the day after the operation as compared with the nonelderly. However, there were no differences between nonelderly and elderly patients with regard to the number of cases with modified Rankin Scale 3–5 and 6 at discharge, the number of re-operation, and postoperative rupture.
Conclusions
In this study, endovascular coil embolization was determined to be a safe and efficacious procedure for elderly patients with unruptured cerebral aneurysm.
Introduction
In societies with a population experiencing progressively advancing aging, the number of elderly patients with stroke is increasing.1–3 In addition, the incidence of subarachnoid hemorrhage (SAH) due to ruptured cerebral aneurysm is also known to increase with age. 4 Therefore, the numbers of elderly patients with SAH as well as the total SAH incidence have been estimated to be increasing.5,6 However, the outcomes of SAH treatment in elderly patients by clipping or coiling are poor because initial SAH grade are poor, the brain is vulnerable, there is a high rate of vasospasm, and other organs tend to be diseased.7–13 Therefore, preventative surgery for elderly patients with unruptured cerebral aneurysm is becoming increasingly important.
The aim of this study was to analyze the safety and efficacy of endovascular coil embolization for elderly patients with cerebral aneurysm. In this study, we classified all patients into two groups: one with ruptured aneurysm and the other with unruptured aneurysm. Because the Japanese Ministry of Health, Labor, and Welfare categorizes a person > 65 years as “elderly,” we defined patients aged < 65 years as “nonelderly” and those aged > 65 years as “elderly.” We further classified both the groups (ruptured and unruptured) according to the defined aged (“nonelderly” and “elderly”). We retrospectively investigated the treatment outcomes and perioperative complications of the patients in the two groups (“nonelderly” and “elderly”) with ruptured/unruptured cerebral aneurysms, who underwent endovascular coil embolization.
Materials and methods
Population
A total of 252 patients (264 aneurysms) who underwent endovascular coil embolization for cerebral aneurysms between April 2012 and August 2018 at our institution were included. This study is retrospective observational study.
In Japan, Flow Divert (FD) was first approved in 2015 as an endovascular treatment for cerebral aneurysms. The first approved FD was Pipeline Flex (Medtronic, Minneapolis, Minnesota, USA), with indications being limited to the aneurysmal size of 10 mm or more and to the internal carotid artery centrally than the posterior communicating artery. However, FRED (Terumo Corporation, Aliso Viejo, CA, USA), an FD approved in 2019, is not limited to such indications and is now possible to place FD in a normal aneurysm. As a result, FD placement has also been performed more frequently in the treatment of aneurysms in the elderly. Therefore, this study focuses on coil embolization patients who underwent treatment up to 2018 in order to examine the outcome of treatment of coil embolization for cerebral aneurysms purely in the elderly.
We divided all the patients into the two groups: ruptured or unruptured. We further subdivided the patients in these two groups (the ruptured and the unruptured groups) into two subgroups: those aged < 65 years as “nonelderly” and those aged > 65 years as “elderly.”
This study was conducted in accordance with the Helsinki Declaration of 1975 as revised in 2024. And this study is in accordance with the STROBE guidelines. 14
Endovascular coil embolization procedure
For unruptured cerebral aneurysms, two antiplatelet agents (aspirin 100 mg/day [Bayaspirin™; Bayer Yakuhin Co. Ltd, Osaka, Japan] and clopidogrel 75 mg/day [Plavix R; Sanofi-Aventis Co. Ltd, Tokyo, Japan] or clopidogrel tablets 75 mg [SANKI; Nichi-Iko Pharmaceutical Co. Ltd, Toyama, Japan]) and a gastric mucosal protective agent (proton pump-inhibitor) were administered starting from 7 days before treatment, and 4000–5000 units of heparin (heparin sodium injection 5000 units/5 mL [MOCHIDA; Mochida Pharmaceutical Co. Ltd, Tokyo, Japan]) was intravenously administered during the procedure, which was controlled between 200 and 300 s by activated clotting time. For ruptured cerebral aneurysms, regardless of the presence or absence of antiplatelet agents, 3000 units of heparin were intravenously administered after sheath puncture. All patients were treated under general anesthesia.
Data analysis
The subjects were evaluated for mean age, sex, location, aneurysmal size, presence of the adjunctive technique, embolization status immediately after treatment and at follow-up, reoperation rate, tortuosity of the vessel (difficult access), perioperative complications (trouble with puncture site, perioperative extravasation, and perioperative thrombosis), morbidity, mortality, and reoperation. With regard to the aneurysmal size, a maximum diameter of < 3 mm was considered as tiny, 3–11 mm as small, and 11–25 mm as large. We used the simple technique with/without a distal access catheter, the balloon assist technique, the stent assist technique, and the double microcatheter technique. The embolic state was set to complete obliteration (CO), residual neck, and residual aneurysm (RA) according to the Raymond–Roy occlusion classification.15,16 Additionally, we defined “difficult access” as the cases in which system changes (such as catheter and wire changes) and access route changes were made because of the tortuosity of the vessel. For only ruptured cerebral aneurysms, we examined the Hunt-Kosnik (H-K) grade and the modified Rankin scale (mRS) at discharge. The clinical severity of SAH was classified according to the H-K grade, with grade 1–2 defined as good and grade 4–5 as poor. 17 Blinded coauthors M.F. and S.K. independently assessed the outcome, and a consensus discussion was held. We defined independent living at discharge as mRS score of 0–2. A mRS score of 3 indicated that the patient could not completely engage in daily life activities and required some assistance for needs such as elimination, bathing, and dressing. Thus, patients with a mRS score of 3–5 at discharge were defined as requiring care. And, a mRS score of 6 indicated death. We performed endovascular coil embolization for all reoperations. For only the unruptured group, the number of lesions in the high-signal area of the magnetic resonance imaging–diffusion-weighted imaging (MRI-DWI) 1 day postprocedure was examined.
Statistical analysis
JMP pro R14 (SAS Institute Inc., Cary, NC, USA) was used for statistical data processing software, and p < 0.05 was considered statistically significant. This study was approved by the Ethics Committee of Osaka Medical College (No. 2840 ; Approval date: 24 January 2020). Additionally, we obtained informed consent from all the patients to use their treatment data.
Results
Ruptured aneurysms
For ruptured cerebral aneurysm group, the mean age of the patients in the nonelderly and elderly groups was 51.8 and 72.0 years, respectively. Furthermore, the number of aneurysm in the nonelderly and the elderly was 20 aneurysms in 20 patients and 22 aneurysms in 21 patients, respectively. There were no differences in the patient backgrounds (sex and proportion of H-K grade 1–2) and aneurysm characteristics (location, aneurysmal size, and case of multiple aneurysm) between the nonelderly and the elderly patients (Table 1). And there were no differences in the used technique (simple technique, adjunctive technique, and parent artery occlusion) during endovascular coil embolization between the nonelderly and the elderly patients (Table 2). Additionally, there were also no differences in the embolization status, difficult access, perioperative complications, the case of mRS 3–5 and 6 at discharge, the re-operation, or re-bleeding among the age groups (Table 3).
Patient backgrounds and aneurysm characteristics between nonelderly and elderly patients in the ruptured / unruptured group.

A-com A: anterior communication artery; ACA: anterior cerebral artery; AN: aneurysm; H-K grade: Hunt-Kosnik grade; ICA: internal carotid artery; MCA: middle cerebral artery; BA: basilar artery; VA: vertebral artery; PCA: posterior cerebral artery.
*Statistically significant with p < 0.05.
Used technique during endovascular coil embolization between nonelderly and elderly patients in the ruptured / unruptured group.

*Statistically significant with p < 0.05.
The evaluation of the efficacy and the safety of endovascular coil embolization between nonelderly and elderly patients in the ruptured / unruptured group.
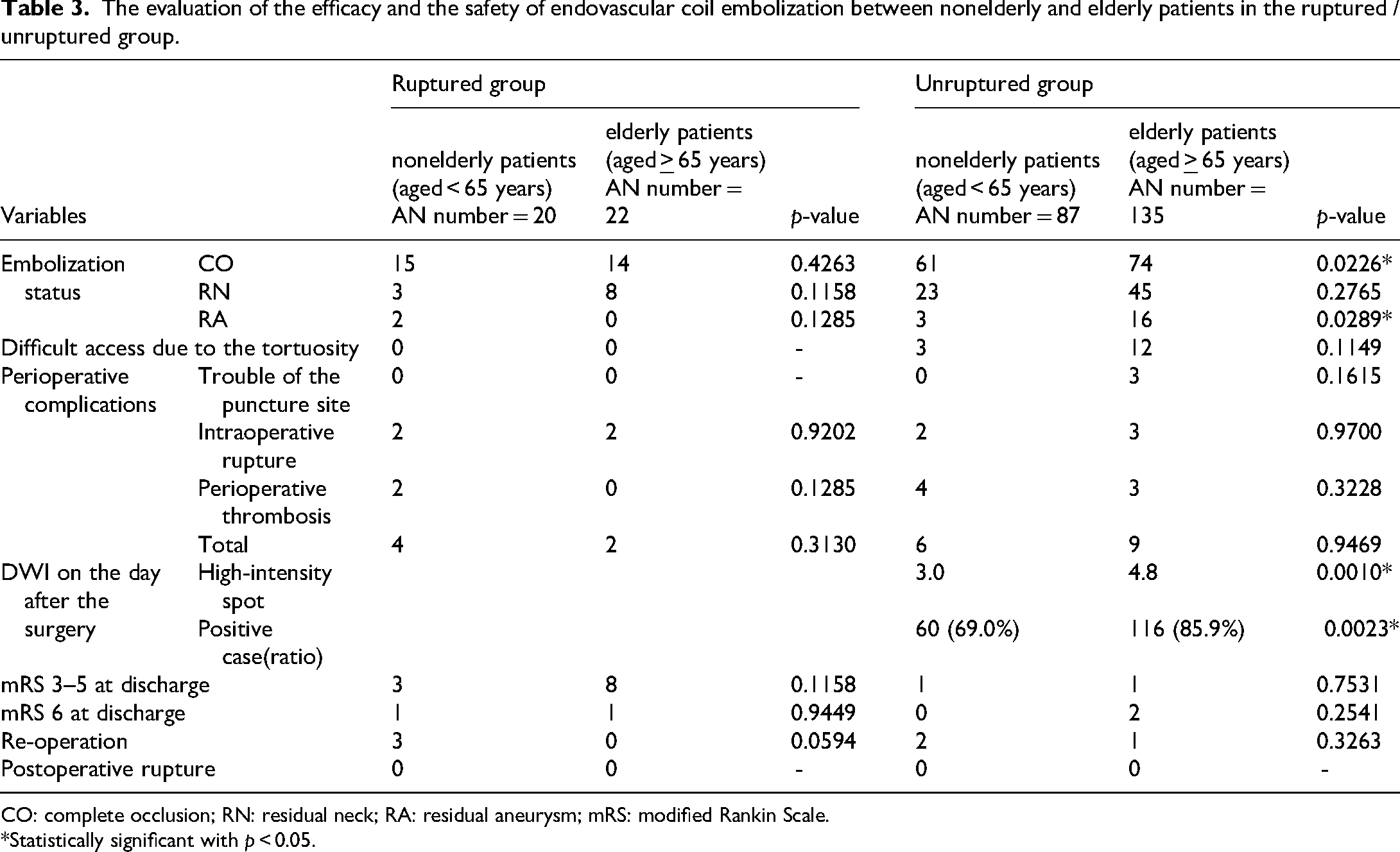
CO: complete occlusion; RN: residual neck; RA: residual aneurysm; mRS: modified Rankin Scale.
*Statistically significant with p < 0.05.
Unruptured aneurysms
For patients with unruptured cerebral aneurysms, the mean age of the patients in the nonelderly and elderly groups was 53.6 and 72.8 years, respectively. The rate of female was found significantly higher in the elderly than in the nonelderly patients (p = 0.0007). And there were significantly difference in the location of aneurysm (middle cerebral aneurysm (p = 0.0081) and posterior cerebral aneurysm (p = 0.0298)) among the age groups. On the other hand, there were no differences in other aneurysm location and aneurysmal size, and case of multiple aneurysm (Table 1). Regarding used technique during endovascular coil embolization, only the double microcatheter technique showed a significant difference (p = 0.0234) (Table 2). As a result of embolization at the end of the treatment, the CO ratio was significantly higher in the nonelderly group than in the elderly group (70.1% and 54.8% in each age groups, respectively; p = 0.0226). In contrast, the RA ratio was significantly higher in the elderly than in the nonelderly patients (11.9% and 3.4% in each age groups, respectively; p = 0.0289). High-intensity areas, as seen by MRI-DWI on the next day of operation, were found in the aneurysm's mother vessel's area. The number of lesions in each age group was 3.0 and 4.8; these numbers were also significantly higher in the elderly group than in the nonelderly group (p = 0.0010), and the DWI positive rate was significantly different between the two groups (p = 0.0023). However, there were no differences in perioperative complications, mRS 3–5 and mRS 6 at discharge, and re-operation rate between the age groups (p = 0.9469, 0.7531, 0.2541, and 0.8406, respectively). Furthermore, no cases of rupture were observed after endovascular coil embolization (Table 3).
Discussion
Many developed countries currently face the realities of an aging or aged society, and in this context, the treatment of elderly patients with ruptured cerebral aneurysms has become a challenge. In the International Subarachnoid Aneurysm Trial (ISAT) reported in 2002, a patient group that underwent endovascular detachable coil treatment for ruptured intracranial aneurysms was compared with a patient group that underwent neurosurgical clipping, and the proportion of patients with good functional prognosis (mRS 0–2) after 1 year was significantly higher in the patient group that underwent endovascular treatment (76.3% vs. 69.4%). 18 Therefore, endovascular coil embolization for ruptured cerebral aneurysms is now the standard treatment. In an ISAT subanalysis that extracted only elderly patients with ruptured cerebral aneurysms reported later, the proportion of patients with good functional prognosis (mRS 0–2) after 1 year was higher in the patient group that underwent endovascular coil embolization (60.1% vs. 56.1%), 19 but the proportion was low overall. Therefore, it is thought that treatment should be performed as much as possible in the unruptured state to prevent SAH of the elderly, but there is an issue of age. With regard to the age limitations of treatable elderly patients with SAH, recent reports have reached a consensus that patients with SAH and aged <70 years have a great potential to achieve a favorable outcome.7,20–25 Some reports have recommended a treatment cutoff at 74 years of age.26,27 On the other hand, the age limitation of treatable elderly patients with unruptured cerebral aneurysm is debatable. Although it has been reported that the complication rate is higher in elderly patients with unrupture aneurysms, 28 no study has investigated the age cutoffs for treatment.
In this study, we analyzed 222 unruptured aneurysms divided into aged < 65 years as “nonelderly” and those aged > 65 years as “elderly.” A significantly higher proportion of cases in the elderly group had high-intensity spots on MRI-DWI on the day after the operation, and an embolization status of “RA” compared with the cases in the nonelderly group (p = 0.0010 and 0.0289, respectively). However, the proportion of patients with an embolization status of “CO” was significantly higher in the nonelderly group (p = 0.0226). However, there were no differences in total perioperative complications, mRS 3–5 and 6, and re-operation between the nonelderly and elderly groups (p = 0.9469, 0.7531, 0.2541, and 0.3263, respectively). Furthermore, no cases of rupture were observed after endovascular coil embolization. Therefore, we demonstrated that endovascular coil embolization is a safe and effective treatment for elderly patients (> 65 years) with unruptured cerebral aneurysm. In fact, the efficacy of endovascular coil embolization for cerebral aneurysm in some elderly patients has already been reported in Japan. 29
In this study, we conducted further statistical analysis to evaluate the risk factors and cutoff age for endovascular coil embolization in patients aged 65 years or older with unruptured cerebral aneurysms. We performed a branching analysis using decision tree analysis on the presence or absence of DWI high-signal intensity on the day after surgery in 135 patients aged 65 years or older with unruptured cerebral aneurysms. The presence or absence of DWI high-signal intensity on the day after surgery was significantly higher in elderly patients, with the cutoff age being 65 years (Table 4).
The decision tree analysis for 135 patients aged 65 years and older.

CO: complete occlusion; RN: residual neck; RA: residual aneurysm; DWI: diffusion-weighted image.
*Statistically significant with p < 0.05.
Conclusion
In this study, we investigated the outcomes of endovascular coil embolization for ruptured and unruptured cerebral aneurysms by age group (< 65 years and > 65 years). For ruptured cerebral aneurysms, there was no significant difference in the prognosis at discharge between nonelderly patients (< 65 years) and elderly patients (> 65 years). In patients with unruptured cerebral aneurysm, the proportion of elderly patients with high-intensity spots on MRI-DWI on the day after the operation, and an embolization status as “RA” were significantly higher than in nonelderly patients. However, there were no differences in discharge mRS 3–5 and 6, perioperative complications, re-operation, and postoperative rupture between the nonelderly and elderly patients. Therefore, this study renders endovascular coil embolization as a safe and efficacious procedure for unruptured cerebral aneurysms in the elderly.
However, this study was retrospective, and there is a possibility that the patient selection was biased. We believe that future prospective studies should be conducted in a wider range of age groups.
Footnotes
Acknowledgments
The authors would like to thank the endovascular team, particularly Ryo Hiramatsu and Hiroyuki Ohnishi, and the professors from Department of Neurosurgery.
Ethic statement
This study was approved by the Ethics Committee of Osaka Medical College (No. 2840).
Consent to participate
Written or electronic consent was obtained from all study participants or the participant's legally authorized representative if the participant could not provide consent.
Authors’ contribution
RY collected the data. RH contributed to the study conception. RY, RH, HO, and SM contributed as a surgeon. RH and MF drafted the plan for the data analysis. RY and RH drafted the manuscript and conducted data analysis. NN, SK, TK, and MW supervised the manuscript. All authors were involved in interpretation of the results and revision of the manuscript, and all approved the final version of the manuscript. SZ and OR are guarantors. The corresponding author attests that all the listed authors meet the authorship criteria and that no others meeting the criteria have been omitted. RY and RH contributed equally to this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data will only be shared following publication, upon receiving a written request and approval from the corresponding author.