
Abstract
Changes that occur naturally throughout the ageing process place the elderly population at greater risk of malnourishment. This review discusses the significance, causes, consequences and assessment of malnutrition in the elderly.
The elderly population: An expanding age group
A detailed understanding of the nutritional status of the elderly has become the focus of intense investigation in recent years, which has been in line with a significant global increase in the average human life expectancy (Figure 1). 1 Although there is no definitive United Nations (UN) standard age at which a person is considered elderly, the UN has established an agreed cut-off of ⩾60 years old. 2 A factsheet recently published by the World Health Organization (WHO) indicates that approximately 12% of the global population (900 million people) was aged ⩾60 years in 2015, with projections of this value almost doubling to 22% (2 billion people) by 2050. 3 Similar predictions have been made in research, with some suggesting that almost a quarter of the global population will be at least 60 years of age by 2050. 4 Indeed, the number of adults to reach the age of ⩾65 years has been estimated to be more than double that of the year 2000 by 2030. 5 Even more substantial claims have been made by other research groups predicting that 21% of the worldwide population will be at least 80 years old by 2050. 6 Considering current statistics and estimates for the future population, this already important public health issue will likely become even more pressing in the coming years.
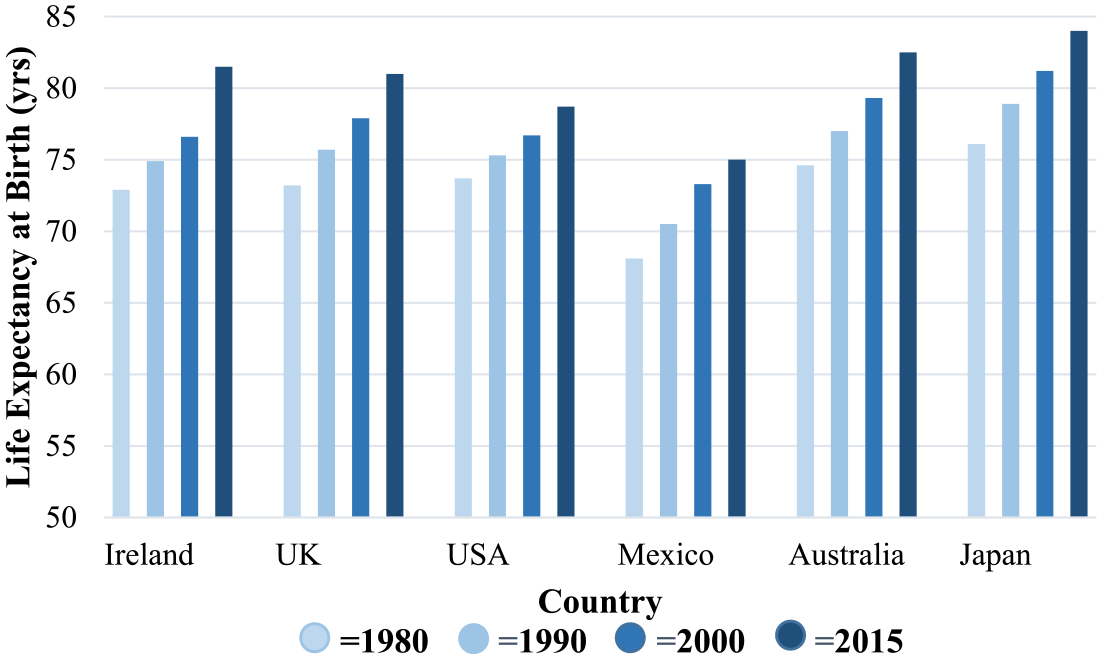
An overview of the global increase in human life expectancy.
Malnutrition
Nutrition is a key factor in the ageing process and a significant contributor to future health, helping to maintain good health and reduce the risk of chronic disease.4,7 –9 Malnutrition in the elderly further increases an individual’s risk of naturally developing general poor health or chronic diseases, such as sarcopenia and cardiovascular disease.4,8 –10 Malnutrition can be used to describe an overall state of poor nutritional status, including undernutrition and overnutrition of macronutrients and/or micronutrients. According to the American Society for Parenteral and Enteral Nutrition (ASPEN) and the Academy of Nutrition, a minimum of two of six criteria, low energy intake, weight loss, loss of muscle mass, loss of subcutaneous fat, fluid accumulation and hand grip strength, need to be fulfilled in order to diagnose an individual as being malnourished. Whereas, the Global Leadership Initiative on Malnutrition (GLIM) suggests that at least one phenotypic criterion, non-volitional weight loss, low body mass index (BMI) or reduced muscle mass, and at least one etiologic criterion, reduced food intake/assimilation or inflammation/disease burden, must be present for a diagnosis of malnutrition to be made.8,9,11 In this review, we apply the term malnutrition according to the European Society for Clinical Nutrition and Metabolism’s definition as undernutrition.8,12
The prevalence of malnutrition in the elderly population
With ever-increasing life expectancy comes an increased risk of health problems and illnesses, many of which can be prevented, delayed or improved by maintaining a healthy diet. 5 The elderly diet is influenced by several internal and external factors, including the ‘9 ds’ outlined by Poulia et al., 13 as dentition, dysgeusia, dysphagia, diarrhoea, depression, disease, dementia, dysfunction and drugs. Some of these factors can influence the environment of the elderly population, which has been shown to have a significant impact on nutrition. If an elderly person is residing in a hospital or care home facility, it has been shown that they are more likely to have a poor nutrition status compared to a community-dwelling elderly person.6,13 –16 Indeed, some investigators have shown that up to 60% and 80% of European geriatric hospital patients are malnourished.6,13,15 Though research related to care facilities and people receiving home help was less extensive, similar results were observed in these environments, while only 15% of community-dwelling elderly people presented as malnourished.6,15
Determinants of malnutrition
The elderly population are at an increased risk of malnutrition due to several risk factors for reduced nutritional intake and body weight that develop throughout the ageing process.7,9,12,17 The ‘anorexia of aging’ is a term used to describe the age-related changes that occur as individuals grow older, which reduces their energy intake and increases their likelihood of becoming malnourished.7,8,10,18 Some of the involved factors include sarcopenia, cachexia, decreased sensory function and changes in the gastrointestinal tract.7,8,10,12,14,17
Sarcopenia
Sarcopenia has been defined as a progressive, age-related loss of skeletal muscle mass and function.8,10,12,17 There is an approximate 8% decline in muscle mass during the age of 40–70 years, which increases 15% every decade thereafter. Furthermore, 5%–13% of 60- to 70-year-olds, and 11%–50% of individuals above the age of 80 years, have sarcopenia in Europe 12 . Reduced physical activity significantly contributes to sarcopenia, causing muscle disease, and over time, muscle loss.7,17 It is also thought that certain hormonal, neural and cytokine activities can stimulate sarcopenia.7,19,20 Muscle loss is caused by acute-phase proteins, generated from increased cytokine activity. 7 The cytokines most commonly associated with the development of sarcopenia, when present in elevated concentrations, include CRP, IL-6, TNF-α and IL-10.19,20 Cytokine activity can be increased by reduced sex hormone, glucocorticoid and catecholamine levels, which occurs as part of the ageing process. 7 Muscle loss can result from a loss of neurones in the spinal cord and neurone cell death, which can occur after a stroke or neural disease. 7 Some studies have indicated that a combination of nutrition guidance, such as vitamin D supplementation, to help downregulate metabolic pathways involved in muscle wasting, and/or increased intake of n-3 polyunsaturated fatty acids (PUFAs), to improve muscle volume and strength, 19 as well as resistance training may be effective in preventing or reducing the action of sarcopenia. 10
Cachexia
Cachexia is characterised as the involuntary loss of fat-free mass (muscle, organ, tissue, skin and bone) or body cell mass, caused by catabolism.7,17 It has been defined as ‘a complex metabolic syndrome associated with underlying illness and characterised by a loss of muscle with or without loss of fat mass’.8,10 Cachexia can cause an acute immune response which releases pro-inflammatory cytokines that alter hormone production and metabolism, leading to an increase in resting energy expenditure.7,10 Acute-phase proteins are produced from a shift in albumin production, causing a negative nitrogen balance and muscle mass loss. 7 Movement of amino acids from muscle to the liver and increased gluconeogenesis also contribute to this negative nitrogen balance. 7 Cachexia is commonly associated with several chronic conditions, such as cancer, chronic obstructive pulmonary disease (COPD), heart failure and rheumatoid arthritis. However, the general increased prevalence of malnutrition, immobility and sarcopenia with ageing also puts the elderly population at a higher risk of developing cachexia.7,8,10,21 In relation to cancer, cachexia has been categorised into three progressive stages of pre-cachexia, cachexia and refractory cachexia, each contributing to an increasing risk of malnutrition.8,10 It is commonly diagnosed after observations of weight loss, reduced BMI, reduced muscle mass and function and disease with on-going elevated inflammatory activity.8,21 Suggested treatment options for cachexia include an optimised diet, appetite stimulants, combination pharmacological therapies and exercise.10,21
Decreased sensory function
Sensory function declines with ageing, which significantly reduces the enjoyment of eating in the elderly population.7,12 It is thought that a loss of taste may be due to a progressively reducing number of taste buds per papilla on the tongue, while the deterioration in sense of smell may be associated with changes in the olfactory epithelium, receptors and neural pathways.7,12,17 Some medications including certain Parkinson’s treatments and anti-depressants have also been shown to negatively influence taste. 7 Indeed, a recent study by Siddique et al. 12 found that up to 74% of elderly subjects experienced taste impairment, while Ahmed and Haboubi 7 determined that more than 60% of subjects aged 65–80 years, and 80% of subjects above the age of 80 years, had a reduced sense of taste and smell. By contrast, less than 10% of subjects below the age of 50 years experienced these same issues. 7 Reduced taste and smell significantly increases an individual’s risk of becoming malnourished, as their appetite, interest in food and the variety of the diet being consumed all reduce with a decline in smell and taste.7,12,17 Indeed, deterioration of taste capabilities has been shown to increase the risk of malnourishment 2.5-fold, while difficulty in swallowing can cause an individual to be five times more likely to become malnourished. 12
Changes in the gastrointestinal tract
There are a variety of changes that occur throughout the digestive system, as individuals age, that can affect their food intake and/or nutrient uptake. 17 Digestive difficulties have been shown to be significant in terms of nutrition, with elderly individuals being 85% more likely to become malnourished when experiencing digestive problems. 12 Gastric acid and pepsin secretion gradually reduce with age, which can limit the metabolism of certain nutrients such as vitamin B12, iron and protein.17,22,23 While reduced pepsin secretion has been shown to be a natural aspect of the ageing process, a decline in gastric acid secretion has been linked to the increased prevalence of Helicobacter pylori infection and atrophic gastritis in the elderly population.7,24 There is also a decrease in the production of saliva, with some evidence indicating that approximately one-third of people above the age of 65 years have reduced saliva production, 25 which slows down peristalsis and increases the likelihood of constipation.17,23 Slower peristalsis can also delay oesophageal emptying, contributing to early satiety.17,23 Early satiety is a substantial contributor to reduced food intake in the elderly population.7,12 This can be caused by changes in sensitivity to gastrointestinal distension, which is associated with an age-related impairment of receptive relaxation of the gastric fundus, causing antral filling of the stomach to occur more quickly. 7 This can further be affected by an increase in satiety hormones, CCK and PP, which prolong satiety by slowing the rate of antral emptying.7,24,25 Generally, the elderly also experience elevated insulin levels, which further emphasises satiety as it can amplify leptin, a hormone associated with satiety when present in high levels, while inhibiting ghrelin, the only known hormone to stimulate hunger.7,25
Malnutrition-associated health problems
The increasing prevalence of malnutrition in the elderly has been associated with several health problems including nutrient deficiency–related symptoms, decreased bone mass leading to osteoporosis, immune dysfunction, and delayed healing and recovery.6,7,17
Nutrient deficiencies
The reduced intake and absorption of nutrients in the elderly population can result in vitamin deficiencies, which can lead to several adverse effects in the body. 7
Vitamin B12 deficiency is common among the elderly population, generally linked to an age-related reduction of intrinsic factor weakening its absorption in the gut.23,24 Approximately 12%–14% of community-dwelling and up to 25% of institutionalised individuals above the age of 65 years were deficient in vitamin B12 in 2010. 7 This deficiency is associated with macrocytic anaemia, cognitive impairment and elevated levels of homocysteine. It is a risk factor for cardiovascular disease and is associated with reduced bone density and increased risk of hip fracture.7,26
Folate deficiency has similar outcomes to vitamin B12 deficiency. It is present in up to 50% of the elderly population, being more commonly observed in institutionalised individuals.7,26 In addition to anaemia, cognitive impairment, increased risk of cardiovascular disease and skeletal deterioration, folate deficiency has been associated with an increased risk of colorectal cancer, dementia and depression.7,27
Reduced food consumption and changes in the gastrointestinal system can lead to insufficient levels of vitamin D.7,24 This is associated with a decline in bone density, reduced mobility and an increased risk of falling. 7 Vitamin D and calcium deficiencies can increase the elderly’s risk of developing osteoporosis, so supplementation of both is recommended for individuals above the age of 65 years to reduce their risk of hip fracture.7,26 It would become increasingly difficult for the elderly population to meet their recommended intake through diet alone, especially for those experiencing a reduced appetite or malnourishment, as vitamin D requirements increase with age, due to decreased skin production, thinning of the skin and less exposure to sunlight.7,26
Osteoporosis
The elderly population have an increased risk of developing osteoporosis due to insufficient vitamin D and calcium levels in the body, as well as the general wear and tear the bones are exposed to throughout the ageing process.7,15,26 In a study carried out by van Bokhorst-de van der Schueren et al., 15 29% of malnourished or at-risk-of-malnourishment elderly people had osteoporosis, while only 11% of adequately nourished elderly people presented with the condition. Increased risk of bone fracture is associated with osteoporosis. Such fractures can be exacerbated due to the delayed healing and recovery time that comes with malnourishment. It is therefore important to prevent the development of osteoporosis, where possible, with the aid of dietary modification and supplementation.7,26
Immune dysfunction
Malnutrition negatively impacts the immune system of individuals above the age of 65 years, leading to an increased risk of developing sepsis.17,26 During the ageing process, the human body accumulates damage to molecules, cells and organs which causes impaired immune function and increased risk of disease. 28 This immune-related biological ageing is referred to as immunosenescence, which contributes to a progressive deterioration of immune function and vaccine-response and increased risk of cancer and chronic and autoimmune diseases.28,29 Vitamin and mineral deficiencies, such as vitamin E and zinc, as a result of malnutrition, can further add to this issue by causing an overall decline in immune function, including an impaired T-cell response, decreased lymphocyte proliferation and reduced delayed-hypersensitivity response.7,26,28 In addition to maintaining optimal micronutrient levels, the use of n-3 PUFAs and probiotics has also been researched for their potentially positive impact on the elderly immune system.28,29 It is thought that n-3 PUFAs have immunomodulatory effects and that consuming probiotics could improve the variety and quality of gut microbiota, enhancing immune function.28,29
Diagnosis of malnutrition
Given the negative impact of malnutrition, including increased morbidity, need for hospitalisation and mortality, it is important to diagnose the condition as early as possible, so that timely and effective nutritional intervention treatment can begin.13,30 –32 The need to carry out nutritional screening as part of a regular check-up is becoming increasingly more important, particularly as malnutrition in the elderly continues to go underdiagnosed due to the natural physiological changes associated with the ageing process.30,33 This is illustrated by the fact that up to one-quarter of nutritionally-at-risk patients, in contact with health care professionals, are currently not receiving nutritional intervention.6,30,31,33 There are primarily three approaches to assessing nutrition: use of biochemical and clinical indices; the combination of anthropometry, mobility, cognitive state and self-perception of health and nutrition; and the combination of medical history and clinical data with subjective evaluation of an individual. 13 Examples of these assessment methods include the Mini Nutritional Assessment (MNA), the Malnutrition Universal Screening Tool (MUST), the Geriatric Nutritional Risk Index (GNRI) and the Nutritional Risk Screening 2002 (NRS-2002) (Table 1).
Efficacy evaluation of nutritional screening tools.
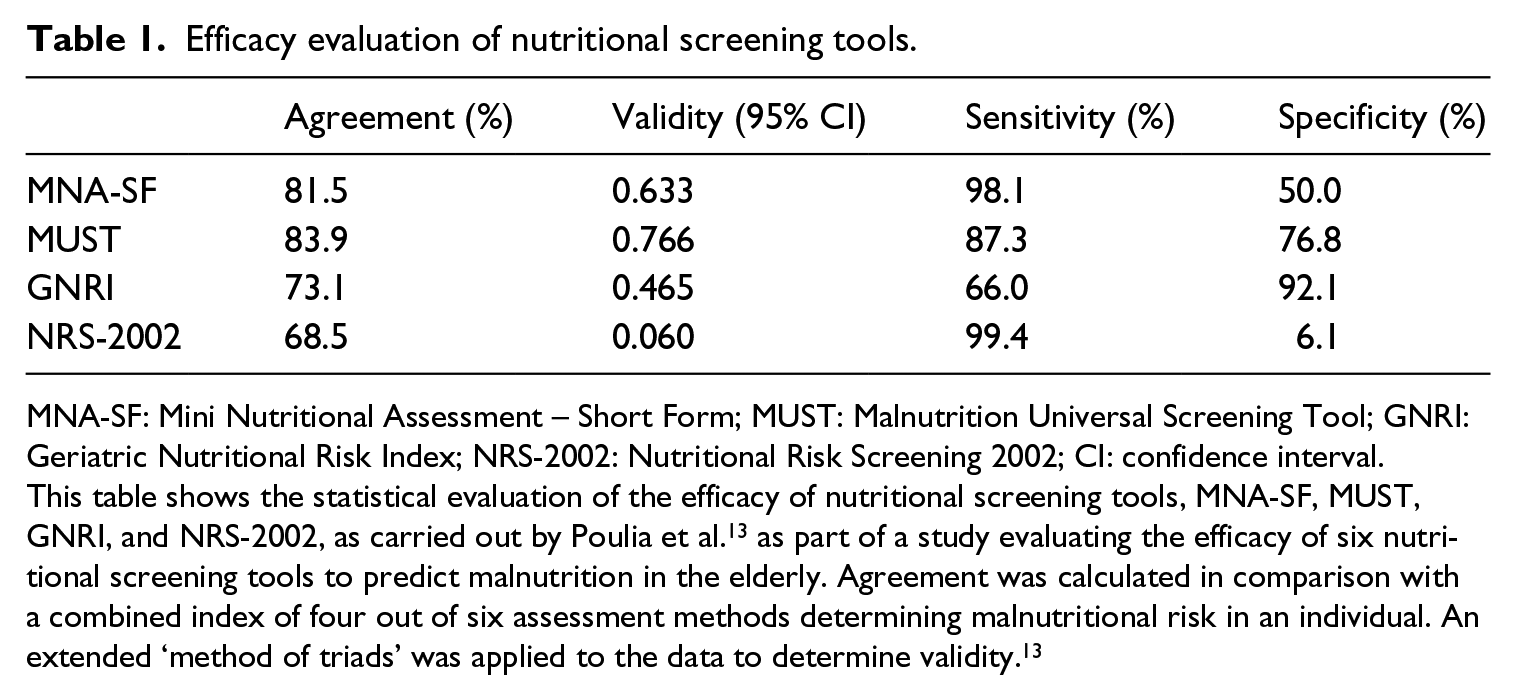
MNA-SF: Mini Nutritional Assessment – Short Form; MUST: Malnutrition Universal Screening Tool; GNRI: Geriatric Nutritional Risk Index; NRS-2002: Nutritional Risk Screening 2002; CI: confidence interval.
This table shows the statistical evaluation of the efficacy of nutritional screening tools, MNA-SF, MUST, GNRI, and NRS-2002, as carried out by Poulia et al. 13 as part of a study evaluating the efficacy of six nutritional screening tools to predict malnutrition in the elderly. Agreement was calculated in comparison with a combined index of four out of six assessment methods determining malnutritional risk in an individual. An extended ‘method of triads’ was applied to the data to determine validity. 13
MNA
The MNA is the most widely used and recommended research method for assessing malnutrition in the elderly, as it has been specifically designed and adapted for the elderly population.13,31,34,35 A short-form version of this tool, the MNA-SF, is more commonly used for screening than the full MNA, as it is quicker and easier to carry out.13,31,36 The MNA-SF is made up of 6 components including weight loss, appetite, mobility, psychological stress, neuro-psychological problems, and BMI, whereas the full MNA is composed of 18 questions.13,31,32,34,36 Each of the parameters listed are scored from 0 to 2 or 0 to 3, to give an overall score of between 0 and 14.13,31,36 The results from carrying out the MNA-SF determine whether an individual is well nourished (score of 12 to 14), at risk of malnutrition (score of 8 to 11) or malnourished (score of 0 to 7).13,31,32,34,36 While it is widely considered as the best option for malnutrition screening and assessment in the elderly, use of the MNA is not appropriate in cases where the individual is not capable of providing reliable information about themselves or is receiving nutritional support via nasogastric tube feeding.13,31,32
MUST
The MUST is a nutritional screening tool that involves three primary considerations: current BMI, weight loss over time and the presence of an acute disease that would significantly decrease the individual’s nutritional intake for more than 5 days.13,30 –32,37 It has been developed for and is applied to adults across all health care settings.13,30,37 Based on the results of the MUST, individuals are diagnosed as being at either low (score of 0), medium (score of 1) or high (score of 2 or more) risk of malnutrition.13,31,32,37 If patients are assessed to be at medium risk of malnutrition, their nutritional status must be monitored, whereas treatment should be initiated for those at high risk of malnutrition.31,37 The MUST is simple and quick to carry out, but not specific for the elderly population.13,30,31
GNRI
The GNRI is an indicator of the risk of elderly individuals developing nutrition-related health problems. Derived from the general Nutritional Risk Index (NRI), it is specifically targeted towards the elderly population. 13 It involves the consideration of serum albumin levels, current body weight and optimal body weight to assess nutritional status.13,34 The GNRI has also been shown to predict mortality in hospitalised elderly patients but has not been validated in a community-dwelling elderly population.13,34 Low serum albumin concentrations in conjunction with weight loss act as indicators of risk of malnutrition-related health problems as assessed by the GNRI. 34 GNRI values are calculated using the following equation

A GNRI greater than 98 suggests there is no risk of nutrition-related health problems, an index between 92 and 98 indicates a low risk, an index between 82 and 91 indicates a moderate risk and an index less than 82 suggests a major risk of nutrition-related complications.13,34
NRS-2002
The NRS-2002 is a screening tool which takes into consideration an individual’s current BMI (>20.5 kg/m2), their recent weight loss, any recent decrease in food intake and the severity of their illness.30,31 A ‘nutritional score’ and ‘severity of disease score’ of 0 to 3 each is applied as part of the NRS-2002.13,31 If the patient being screened is above the age of 70 years, an extra point is added to their score.13,30,31 This method means that a score range from a minimum of 0 to a maximum of 7 can be determined.13,31 The potential benefit from nutritional support is subjective to the assessor when carrying out the NRS-2002. However, in certain research settings, individuals scoring 0 are considered to be at no risk of malnutrition, between 1 and 2 are considered at low risk, between 3 and 4 at medium risk and 5 or more at high risk.13,31 Research has shown that the NRS-2002 is highly sensitive and has a low predictive value, which sometimes leads to incorrect classification of malnourishment or risk thereof, making it a potentially unreliable screening tool.13,30
Conclusion
With age-related risk factors already associated with the elderly population developing malnutrition, it is essential to minimise the risk from inadequate dietary intake, either through supplementation, dietary modifications or a combination of both. The risk of developing certain chronic diseases and conditions in the elderly population can be significantly reduced, and the overall quality of life can be improved, through adequate and timely nutritional intervention. While some evidence exists for the benefits of nutrients and bio additives, such as probiotics, further study is required to inform the best nutritional guidelines for the elderly, especially as the global population continues to age.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.