
Abstract
Objective
This study aimed to investigate the clinical characteristics of elderly chronic kidney disease (CKD) patients; and the correlation among their biochemical indicators, physical activity, and functional parameters. The findings of this study will hopefully a scientific basis for better understanding the causes and developing the best management methods for CKD in this population.
Methods
In total, 280 elderly patients with CKD participated in this cross-sectional study. All patients underwent a multidimensional assessment of clinical data, physical activity, and functional performance. Patients were stratified by disease severity into two groups: CKD stages 1–3 and stages 4–5. Additionally, they were categorized as sedentary or nonsedentary based on metabolic equivalent of task (MET) levels. Inter-group differences and correlations among the variables were subsequently analyzed.
Results
Research findings indicated that although male patients predominated in the overall cohort, female patients were more prevalent among those with advanced CKD (stages 4–5) and those reporting a sedentary lifestyle, and these subgroups also demonstrated a higher likelihood of hypertension and anemia. Compared to patients with CKD stages 1–3, those in stages 4–5 had significantly lower estimated glomerular filtration rate (eGFR), hemoglobin, albumin, and MET values (P < .05), along with higher serum creatinine and Barthel Index of Activities of Daily Living (BADL) values (P < .05). Similarly, when compared to nonsedentary patients, those with a sedentary lifestyle exhibited lower eGFR, hemoglobin, and MET levels (P < .05), alongside elevated procalcitonin (PCT) and BADL values (P < .05). Correlation analyses further revealed that renal function was significantly associated with both BADL and MET values in the studied CKD population (P < .05). Our correlation analysis also revealed that renal function in elderly advanced CKD patients is closely associated with levels of PCT and Hb (P < .05). Moreover, among sedentary elderly CKD patients, renal function was correlated not only with PCT and Hb (P < .05), but also with albumin and physical activity levels MET (P < .05).
Conclusions
Our study identified a predominance of female patients in advanced CKD stages and among those leading sedentary lifestyles. Furthermore, our findings suggest that renal function may be associated with physical activity and functional performance, with this relationship appearing most pronounced in sedentary individuals. The results also point to a potential interrelationship between renal function, inflammation, and nutritional status in advanced CKD.
Introduction
Chronic kidney disease (CKD) is caused by various primary or secondary factors, which can lead to the serious destruction of nephrons, the retention of metabolic waste, and body water, electrolyte and acid‒base balance disorders, resulting in various clinical manifestations. The morbidity and mortality of CKD are high, and it has become a major public health problem worldwide.1,2 During the early stages of CKD, patients with CKD may be overlooked due to unclear symptoms, which leads to a delay in receiving interventions that could slow down or prevent disease progression. 3 With the progression of CKD, the quality of life and life expectancy of patients gradually decrease.4,5 Moreover, late-stage CKD is associated with increased health care costs and resource use.6,7
The prevalence of CKD in China is approximately 8.2%, 8 and a recent study predicted an upward trend for the incidence of CKD in China in the next 15 years. 9 In China, a substantial increase in associated health care system costs of CKD (excluding kidney replacement) is projected, from ¥1.14 trillion in 2022 to¥1.66 trillion in 2032. 10 Moreover, a recent pragmatic review research showed that the average annual costs associated with CKD increased fourfold upon progression from stage G3a to G5. 3 Additionally, age is an important risk factor for CKD. 11 At present, China has entered an aging society, with over 200 million people aged 65 years or older. 12 With the continuous increase in the aging population, the number of elderly people with CKD will continue to increase. This will undoubtedly increase China's social burden. Hence, effectively managing and delaying the development of CKD in elderly patients is necessary to alleviate the social burden in China.
CKD is usually related to comorbidities, nutritional status, physical function, and lifestyle.13–16 Although these factors have been studied, their relationship has been largely overlooked, specifically in China. Moreover, the comorbidities, complications, and poor functional status of CKD can complicate the condition of elderly CKD patients, making the control of CKD in elderly individuals challenging. 17 The evidence generated from the adult population of CKD may not be fully applicable to elderly CKD patients. Therefore, this study focuses on: (a) the clinical characteristics of elderly CKD patients; and (b) the correlation among their biochemical indicators, physical activity, and functional parameters. The findings of this study will hopefully a scientific basis for better understanding the causes and developing the best management methods for CKD in this population.
Methods
Study design and participants
This is a cross-sectional analysis of elderly patients from the physical evaluation and adverse outcomes for patients with CKD in the study in Chengdu, China.
This study employed consecutive recruitment, screening all elderly CKD patients discharged from Chengdu Eighth People's Hospital affiliated with Chengdu Medical College between January 2019 and September 2025. A total of 493 participants were initially considered potentially eligible for the study. The inclusion criteria were as follows: (a) diagnosed with CKD; (b) aged ≥ 65 years; and (c) accepted conservative treatment. The exclusion criteria were as follows: (a) incomplete medical records; (b) acute exacerbation of CKD; (c) CKD combined with cancer; (d) CKD combined with hemorrhagic anemia; and (e) physically disability to perform physical activities. After applying the inclusion and exclusion criteria, 280 participants were ultimately enrolled in the study (Figure 1).
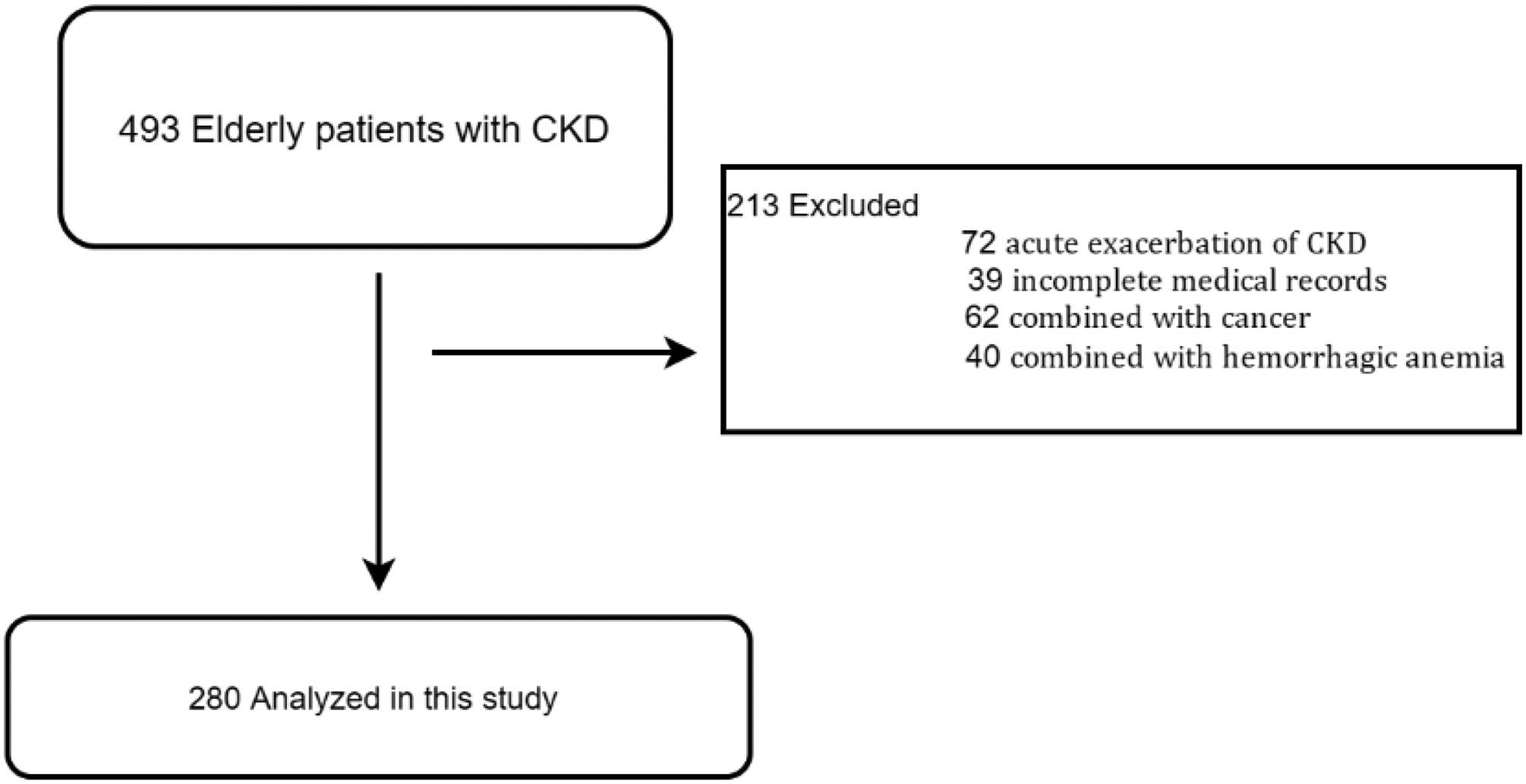
A flowchart of the subject inclusion.
The sample size for this study was derived from the following formula:
The sample size calculation yielded a minimum requirement of 258 participants. However, the study recruited a total of 280 patients to ensure sufficient power.
This study followed the STROBE reporting guidelines, 19 and it was conducted in accordance with the ethical principles of the Helsinki Declaration of 1975 as revised in 2024 and approved by the institutional review board of Chengdu Eighth People's Hospital (No. 2023–CBYEC-057 on May 5, 2023). All data for this study were obtained from the patients’ medical records. Patient information was fully de-identified. Given the retrospective analysis of anonymized data from the hospital's dedicated data registry and electronic medical record system, the ethics committee granted a waiver of informed consent.
Physical activity and functional performance
The metabolic equivalent of task (MET) is a quantitative measure of physical activity intensity, and the average daily MET value can be considered as a measure of the average daily activity level. In elderly populations, activity levels are classified as follows: a daily mean of <1.5 METs is sedentary, 1.5–3 METs indicates light activity, and ≥3 METs represents moderate-to-vigorous activity.20,21
The Barthel Index of Activities of Daily Living (BADL) is a measure of functional performance, assessing six core activities: bathing, dressing, toileting, transferring, eating, and continence. Each item is scored dichotomously: 0 points indicate independence (no assistance required), and 1 point indicates dependence (partial or complete assistance required). The total score ranges from 0 to 6, with higher scores reflecting greater dependency. 22
Clinical data
All clinical data were obtained from the patients’ medical records. The demographic data included age, sex, and history of hypertension, diabetes, or hyperlipidemia. The biochemical data included blood creatinine, hemoglobin (Hb), serum prealbumin, albumin, globulin, and procalcitonin (PCT) levels. The estimated glomerular filtration rate (eGFR) was estimated by using the modified MDRD equation, 23 and the CKD stage was classified according to the Kidney Disease: Improving Global Outcomes (KDIGO) 2012 clinical practice guidelines. 24 According to the recommendation of the World Health Organization, anemia is defined as a Hb level of <130 g/L in males and <120 g/L in females.25,26
Statistical analysis
All the data were analyzed by SPSS statistical software version 21.0. Data were described as percentages (%) for categorical variables and mean and standard deviation (M ± SD) or median and interquartile range for continuous variables. The chi-square test was employed to compare the distribution of categorical variables (e.g. gender and comorbidity) across the groups. For comparisons of continuous variables (e.g. biochemical data, BADL, and MET) between groups, independent samples t-tests were used for normally distributed data; otherwise, nonparametric tests were applied. In addition, depending on the distribution of the data, correlations were analyzed using either Pearson's test (for normal distribution) or Spearman's test (for nonnormal distribution). P < .05 was considered to indicate statistical significance.
Results
Baseline characteristics of the patients with CKD
A total of 280 elderly patients with CKD were included in this study; 146 (52.14%) were men, and 134 (47.86%) were women. A total of 221 (78.93%) participants had a history of hypertension, 166 participants (59.29%) had a history of diabetes, and 64 (22.89%) participants had a history of hyperlipidemia, 161 (57.5%) participants had a history of anemia. The mean age was 77.78 ± 6.49 years. The mean biochemical data were as follows: serum prealbumin level, 194.69 ± 68.97 mg/L; albumin level, 35.16 ± 4.73 g/L; and globulin level, 31.07 ± 6.51 g/L. The median biochemical data were as follows: eGFR, 46.74 (43.72, 49.77) ml/min/1.73 m2, Hb level, 105.43 (102.88, 107.98) g/L, blood creatinine level, 157 (145.44, 168.57) μmoI/L; and PCT level, 0.35 (0.24, 0.46) ng/ml. The median physical activity and functional performance score were as follows: BADL, 3.15 (3.01, 3.29); MET, 1.79 (1.74, 1.85).
Clinical characteristics of the patients with CKD stages 1–3 and CKD stages 4–5
There were no significant differences in age between the two groups, but a significant difference was found in gender distribution. The incidence rates of diabetes and hyperlipidemia did not significantly differ between the two groups; however, there were significant differences in the incidence of hypertension and anemia between the groups (P < .05), and participants with CKD stages 4–5 had a greater prevalence of antianemic treatment (P < .05) (Table 1). According to Table 1, compared with patients with CKD stages 4–5, patients with CKD stages 1–3 had lower score of BADL score and higher score of MET (P < .05). There were no differences in the serum prealbumin or globulin levels between the two groups. Moreover, there were significant differences in the eGFR and blood creatinine, Hb, albumin, and PCT levels between the two groups (P < .05) (Table 1).
Clinical characteristics of patients with CKD stages 1–3 and CKD stages 4–5.
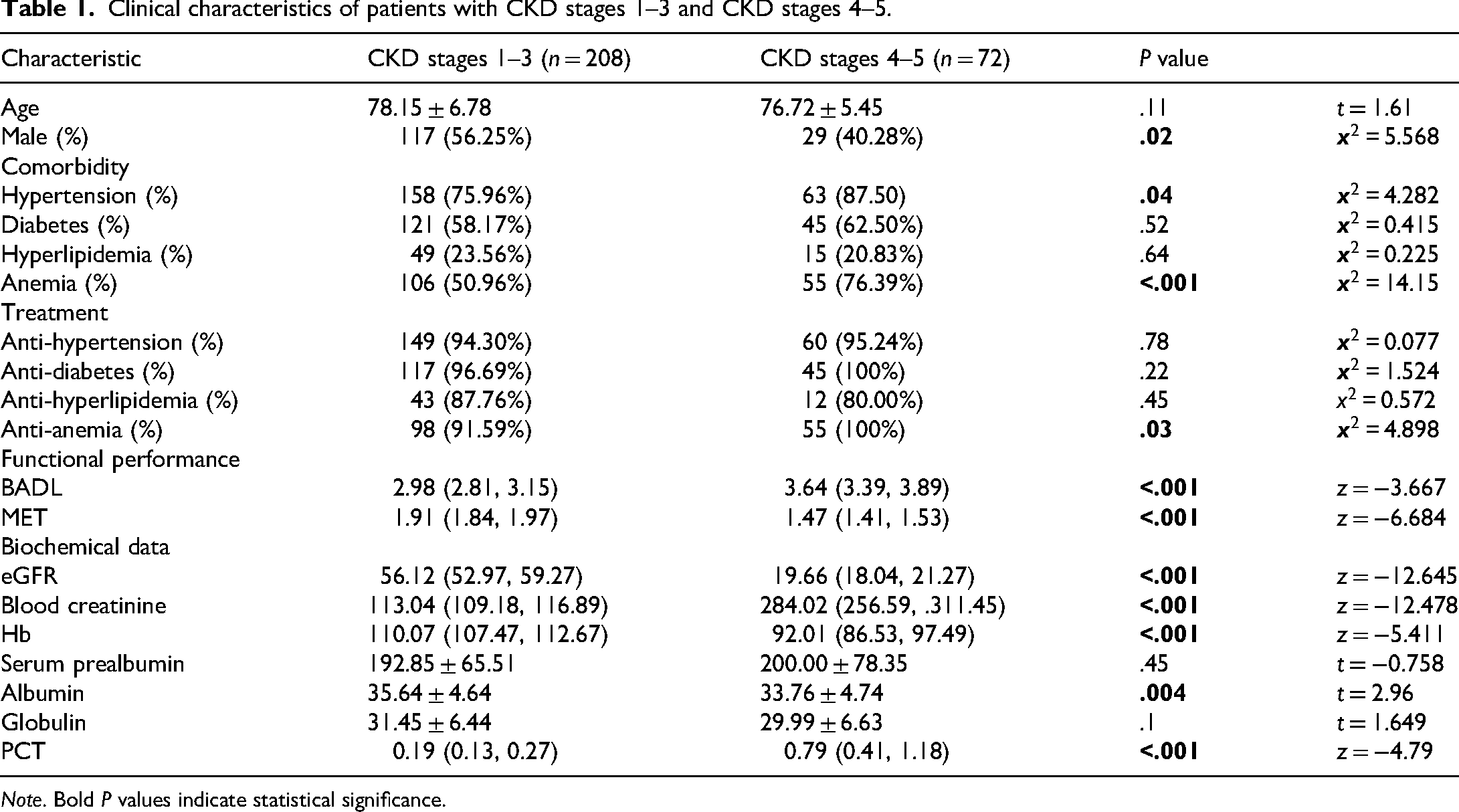
Note. Bold P values indicate statistical significance.
Clinical characteristics of the CKD patients based on their sedentary or not sedentary lifestyle
Owing to recent research showed that muscle loss and lifestyle are associated with CKD,27,28 and the difference in MET value between patients with CKD stages 1–3 and 4–5 in this study, we divided CKD patients into sedentary (MET value ≤ 1.5)and not sedentary (MET value > 1.5)lifestyle subgroups. According to Table 2, there were 95 CKD patients with sedentary lifestyle. They were older, had a higher BADL value, and MET value was significantly lower than that in nonsedentary participant (P < .05). The incidence rate of hypertension and anemia significantly differed between patients with sedentary and patients with nonsedentary (P < .05). Table 2 also shows that CKD patients with sedentary had lower eGFRs and Hb levels and higher blood creatinine and PCT levels than did CKD patients with nonsedentary (P < .05).
Clinical characteristics of the CKD patients based on their sedentary or not sedentary lifestyle.

Note. Bold P values indicate statistical significance.
Relationships among the biochemical, physical activity level, and functional parameters in elderly CKD patients
As shown in Figure 2A, the eGFR was positively correlated with the Hb level (r = .24, P < .001) and MET value (r = .35, P < .001), and was negatively correlated with BADL value (r = ‒.20, P < .001), and the PCT level was negatively correlated with the eGFR (r = ‒.31, P < .001), Hb level (r = ‒.43, P < .001) and albumin level (r = ‒.39, P < .001), and the Hb level was positively correlated with the albumin level (r = .54, P < .001) and MET value (r = .28, P = 0.002), and was negatively correlated with the BADL value (r = ‒.36, P = <.001), and the BADL value was negatively correlated with the MET value (r = ‒.92, P≤.001) in elderly patients with CKD. Figure 2B shows the correlation of relevant indicators in elderly patients with CKD stages 1–3. The Hb level was positively correlated with the albumin level (r = .50, P < .001) and MET value (r = .24, P < .001), and was negatively correlated with the BADL value (r = ‒.33, P < .001), and the PCT level was negatively correlated with the Hb level (r = -.30, P < .001) and albumin level (r = -.34, P < .001). In addition, the BADL value was negatively correlated with MET value (r = ‒.94, P < .001). As shown in Figure 2C, the eGFR was positively correlated with the Hb level (r = .48, P < .001) and albumin level (r = .26, P = 0.03), the Hb level was positively correlated with the albumin level (r = .63, P < .001), and the PCT level was negatively correlated with the eGFR (r = ‒.40, P < .001), Hb level (r = ‒.50, P < .001) and albumin level (r = ‒.52, P < .001), and the BADL value was negatively correlated with the Hb level (r = ‒.24, P = 0.04) and MET value (r = ‒.91, P < .001) in elderly patients with CKD stages 4–5.

Correlations among the relevant indicators. (A) Relationships among the eGFR, Hb level, albumin level, PCT level, BADL value and MET value in elderly patients with CKD. (B) Relationships among the eGFR, Hb level, albumin level, PCT level, BADL value and MET value in elderly patients with CKD stages 1–3. (C) Relationships among the eGFR, Hb level, albumin level, PCT level, BADL value and MET value in elderly patients with CKD stages 4–5. The numbers in the boxes represent the correlation coefficient (r value).
Relationships among the biochemical, physical activity level, and functional parameters in elderly CKD patients with sedentary or not sedentary lifestyle
Figure 3A shows that the correlation of relevant indicators in elderly CKD patients with sedentary. The results revealed a positive correlation between the eGFR and the Hb level (r = .53, P < .001), albumin level (r = .24, P = 0.02) and MET value (r = .24, P = 0.017). Additionally, the PCT level was negatively correlated with the eGFR (r = ‒.41, P < .001), Hb level (r =‒.55, P < .001) and albumin level (r = ‒.53, P < .001), and the Hb level was positively correlated with the albumin level (r = .53, P < .001), and the BADL value was negatively correlated with the MET value (r = -.80, P < .001). As shown in Figure 3B, the PCT level was negatively correlated with the eGFR (r =‒.21, P = 0.005), Hb level (r = ‒.34, P < .001), and albumin level (r = ‒.31, P < .001). The Hb level was positively correlated with the albumin level (r = .53, P < .001), MET value (r = .24, P = 0.001). In addition, the BADL value was negatively correlated with the Hb level (r = ‒.36, P < .001), albumin level (r = ‒.26, P < .001) and MET value (r = ‒.85, P < .001).

Correlations of the relevant indicators in elderly CKD patients with sedentary or not sedentary lifestyle. (A) Relationships among the eGFR, Hb level, albumin level, PCT level, BADL value and MET value in elderly CKD patients with sedentary lifestyle. (B) Relationships among the eGFR, Hb level, albumin level, PCT level, BADL value and MET value in elderly CKD patients with not sedentary lifestyle. The numbers in the boxes represent the correlation coefficient (r value).
Discussion
In this study, we investigated clinical feature, physical activity, and functional parameters in elderly patients with CKD. The study participants had a higher prevalence of hypertension, diabetes, and anemia. Additionally, the cohort comprised a higher proportion of males. Our findings suggest that the severity of elderly patients with CKD is correlated with BADL and MET value.
Subgroup analysis by disease stage demonstrated that patients with CKD stages 4–5 were mainly female, and had a higher prevalence of hypertension and anemia. Unsurprisingly, CKD4–5 patients had lower eGFR levels and poor nutritional status. Additionally, CKD4–5 patients had higher BADL value and lower MET value. Other subgroup analysis further demonstrated that sedentary elderly CKD patients (i.e. those with MET value ≤ 1.5) were associated with older age, a higher proportion of females, and a greater likelihood of hypertension and anemia. Compared with nonsedentary patients, those with sedentary had more advanced CKD and higher BADL scores. These findings confirm that aging, hypertension, and anemia are established factors associated with CKD in the elderly, aligning with previous research.11,29,30 Besides, gender is also associated with elderly CKD. Existing literature reports a female preponderance in early CKD. 31 Nevertheless, our findings reveal a sustained higher prevalence of women in an elderly cohort marked by progressive functional decline. This may be related to estrogen levels. Estrogen is known to exert a protective effect on renal function in women. 32 The age-related decline in estrogen levels may therefore compromise this protection. A recent study showed that lower endogenous estrogen levels in later years are associated with a higher incidence of CKD. 33 Therefore, it is best to regularly monitor estrogen levels for elderly women with CKD.
While exercise is recognized to have beneficial effects on CKD, the precise association between physical function and CKD remains controversial.34,35 A meta-analysis suggested that a higher level of physical activity was associated with a lower odds of CKD. 36 Furthermore, other studies have linked both physical activity and sedentary behavior to renal function and damage. 37 In contrast, other researchers believed that physical activity is not related to CKD.38–40 Our findings showed that higher eGFR levels are associated with greater physical activity (MET) and lower dependency (BADL) in elderly CKD patients. This correlation between eGFR and MET was most pronounced among sedentary patients, demonstrating that renal function is more tightly coupled to physical activity in this subgroup. In CKD patients, complications like malnutrition, inflammation, and anemia lead to sarcopenia and frailty. 41 A sedentary lifestyle compounds this by accelerating muscle loss, reducing functional capacity, and elevating insulin resistance and inflammation,42,43 which in turn accelerates renal function decline. Altogether, our data still tend to suggest a correlation between physical activity and elderly CKD, but further research is needed on the underlying mechanisms.
Furthermore, extensive research has established that nutritional and inflammatory status are critical determinants of eGFR in patients with advanced CKD.44,45 Our correlation analysis revealed that renal function in elderly advanced CKD patients is closely associated with levels of PCT and Hb. Moreover, among sedentary elderly CKD patients, renal function was correlated not only with PCT and Hb, but also with albumin and physical activity levels MET. The PCT, Hb, and albumin levels can reflect inflammation and nutritional status of patients with CKD.46–48 Therefore, our research results provide a basis to some extent for the importance of timely exercise, nutritional support, and anti-inflammatory treatment in the early stage of CKD.
Our research has several limitations. First, this was an observational study, not a double-blind randomized controlled trial, so the results of this study should be interpreted as associations rather than causal relationships. Second, the data are limited to a single center and cannot fully represent the entire elderly CKD population. Third, our indicators are relatively single in evaluating relevant content. Finally, this was a cross-sectional analysis that could not evaluate the changes in various indicators over time. Future studies should employ prospective longitudinal designs with larger, more diverse samples to further elucidate the interrelationships between renal function, physical activity, and nutritional status in elderly CKD patients.
Conclusion
Our study identified a predominance of female patients in advanced CKD stages and among those leading sedentary lifestyles. Furthermore, our findings suggest that renal function may be associated with physical activity and functional performance, with this relationship appearing most pronounced in sedentary individuals. The results also point to a potential interrelationship between renal function, inflammation, and nutritional status in advanced CKD. Collectively, these findings highlight the critical importance of implementing early interventions—including tailored exercise regimens, nutritional support, and anti-inflammatory strategies—especially for elderly female patients.
Abbreviations
Chronic kidney disease
Estimated glomerular filtration rate
Hemoglobin
Procalcitonin
Kidney Disease: Improving Global Outcomes
metabolic equivalent of task
Barthel Index of Activities of Daily Living
Footnotes
Acknowledgments
We wish to thank Chengdu Eighth People's Hospital for their great support of this project.
Ethical approval and consent to participate
This study was conducted in accordance with the ethical principles of the Helsinki Declaration and approved by the institutional review board of Chengdu Eighth People's Hospital (No. 2023-CBYEC-057 on 05.05.2023). All data for this study were obtained from the patients’ medical records. Given the retrospective analysis of anonymized data from the hospital's dedicated data registry and electronic medical record system, the ethics committee granted a waiver of informed consent.
Author contribution
YD conceptualized the study, designed the plan, and revised the manuscript. YS and QY collected the data. HM, JY and SY stored and managed the data. XL and YT analyzed the data. QW wrote the original draft of the manuscript. All the authors read and approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Medical Research Projects of Chengdu (2022240; 202317013476; 2024587) and the General Projects of Sichuan Provincial Administration of Traditional Chinese Medicine (MS2023465).
Declaration of Conflicting Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflicts of interest.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.