
Abstract
Objective
This study sought to develop a prediction model for double-J pipe scab following radical total cystectomy.
Methods
This retrospective study included clinical data on 175 patients who underwent routine double-J pipe replacement after radical total cystectomy. A double-J pipe scab was the nomogram's outcome. Boruta feature selection and the least absolute shrinkage selection operator (LASSO) approach were employed to predictions as efficiently as possible. Using multiple logistic regression, predictive models were created and displayed as nomograms. Nomogram performance was assessed using decision curve analysis, calibration plots, and receiver operating characteristic (ROC) curves. By computing the validation cohort's performance, the model was internally validated.
Results
This study covered 175 patients in total. In twenty-nine individuals (16.57%), a double-J pipe scab formed. Every participant was randomly split into two groups: training (n = 122) and validation (n = 53). As predictors, this nomogram included urine leukocytes, urinary PH, daily water intake, BMI, and double-J pipe brand. Excellent identification performance is indicated by the training and verification groups’ ROC curves, while the calibration curves demonstrate both groups’ excellent correction outcomes.
Conclusion
This study establishes a foundation for preventing and treating double-J pipe stones. It has a substantial predictive value for the occurrence of double-J pipe stones in the double-J pipe following radical total cystectomy.
Introduction
Bladder cancer is the most common malignancy of the urinary tract and ranks ninth overall. 1 Because of population ageing and environmental degradation, bladder cancer is becoming more common. 2 Urinary tract drainage and reconstruction surgery are frequently necessary for postoperative patients, and total cystectomy is the preferred treatment for bladder cancer that invades the muscular layer. Double-J pipe are a vital drainage material for the urinary tract. They are employed extensively in treating various urinary system illnesses, including ureteral strictures, tumours and calculi.3–5 However, there is a chance that bacteria will grow biofilms on the stent surface if the stent is left in the ureter for an extended period. Failure to remove the stent within 3 months may result in serious consequences, including infection, haematuria and scaling. 6 Even though double-J pipe encrustation problems are frequent, they are frequently overlooked in clinical settings, and there needs to be more research on the subject.7,8 In severe circumstances, this encrustation phenomenon can cause intimal dissection and ureter damage, making it difficult to remove the catheter.9–11 According to several studies, concomitant infection, long stent indwelling times and poor patient compliance are risk factors for stent encrustation.12–14
The issue of double-J pipe encrustation has yet to be a comprehensive remedy. Previous research has concentrated on retrospective analysis and empirical pooling, and no successful clinical solutions exist. No early risk assessment techniques are available for double-J pipe encrustation, and clinical care of symptoms is the norm. As artificial intelligence has grown in recent years, machine learning algorithms have been used increasingly to create predictive models. 15 Non-variable screening models are inappropriate for clinical practice and have significant computing costs during operation and subsequent maintenance. They could be more reproducible in a variety of healthcare settings. After least absolute shrinkage selection operator (LASSO) regression was used to eliminate risk factors, we further screened variables using the Boruta feature screening method. We then used iterative processing to identify significant predictors for double-J pipe scabs to handle random fluctuations in random forest importance scores and factor interactions. This approach is used extensively in Diabetes Mellitus research for feature selection.16,17
A simple and effective risk assessment instrument is essential for identifying high-risk patients and implementing preventive measures. In addition, this will provide us with a theoretical and decision-making framework for preventing the incidence of double-J pipe scaling following total bladder surgery.
Patients and methods
Study design and participants
This study was retrospective. We selected 175 patients who regularly replaced the double-J pipe at the Department of Urology, the First People ‘s Hospital of Nantong between January 2020 and October 2024 as the study subjects, resulting in scab formation of the double-J pipe (Figure 1). The results showed that the patients had double-J pipe scabs (according to a 7:3 ratio, they were split into two groups at random: the modelling group (n = 122) and the validation group (n = 53)). Criteria for inclusion include individuals at least 18 years old and those who frequently swap out their double-J pipe following a radical total cystectomy. Exclusion criteria include (1) incomplete medical records; (2) patients not treated in our hospital for double-J pipe extraction; and (3) patients with severe conditions affecting the urinary system, such as a ureteral stricture.

Double J tube encrustation versus non-encrustation.
Data collection
The demographic characteristics included comorbidities, daily water intake, hydronephrosis, blood and urine regimen, number of double-J pipe adjustments, double-J pipe brand, and other measures. The patient information mentioned above was obtained from electronic medical records. A second auditor confirmed all chart review data before including it in the research. In addition, all patient identifiers were removed from all data. Reporting of this study complies with STROBE guidelines. 18
Ethics and informed consent
This retrospective study has been approved by the Ethics Committee of the First Hospital of Nantong (2023KT212). All subjects included in the study had signed an informed consent form authorising the use of the information for future scientific research. Retrospective data analysis followed the ethical guidelines applicable at the time of source data collection (Declaration of Helsinki 2013 revision).
Stone composition analysis
An infrared spectrometer (SUN-3G type) was utilised in this work to analyse the composition of the stones. Stone samples were dried in an oven for 5–10 min at 100 °C. After adding dried potassium bromide powder to small granular stone specimens in an agate mortar and grinding them evenly, the powder was put in a compression mould and compressed with a tablet press at 16 MPa for 5 s to create uniform, translucent tablets. These tablets were then placed in an interpretation analyser to gather spectra, and the spectra were examined using computer software to generate stone reports.
Statistical analysis
Statistics were done with SPSS 23.0 and R 4.1.2. For comparison across groups, an independent sample t-test was used for normally distributed continuous data with mean and standard deviation, and chi-square and Mann-Whitney U tests were used for discrete data with frequency, component ratio, or percentage. A logistic regression model was created with double-J pipe scaling as an independent outcome. Stepwise logistic regression was used for covariates with a univariate logistic regression P-value < 0.10 to identify risk factors for scaling with double-J pipe. Each validation library patient double-J pipe's scaling probability was calculated using logistic regression. Probabilities were predicted using receiver operating characteristic (ROC) curves and internally validated using Bootstrap. The Hosmer-Lemeshow test calibrated the logistic regression model based on the expected likelihood and actual occurrence of double-J pipe scaling.
Results
Patient characteristics
One-hundred seventy-five patients had their data tracked. The incidence of double-J pipe stones was 16.57%, with 29 developing the condition. The demographic characteristics of the patients are detailed in Table 1. Among the 29 patients, simple stones were primarily composed of anhydrous uric acid (33.93%) (11/29) and calcium oxalate monohydrate (13.79%) (4/29); mixed stones were composed mainly of uric acid + sodium urate + calcium phosphate (17.24%) (5/29). Figure 2 is a flow chart of the case selection and study process. Table 2 illustrates particular outcomes.
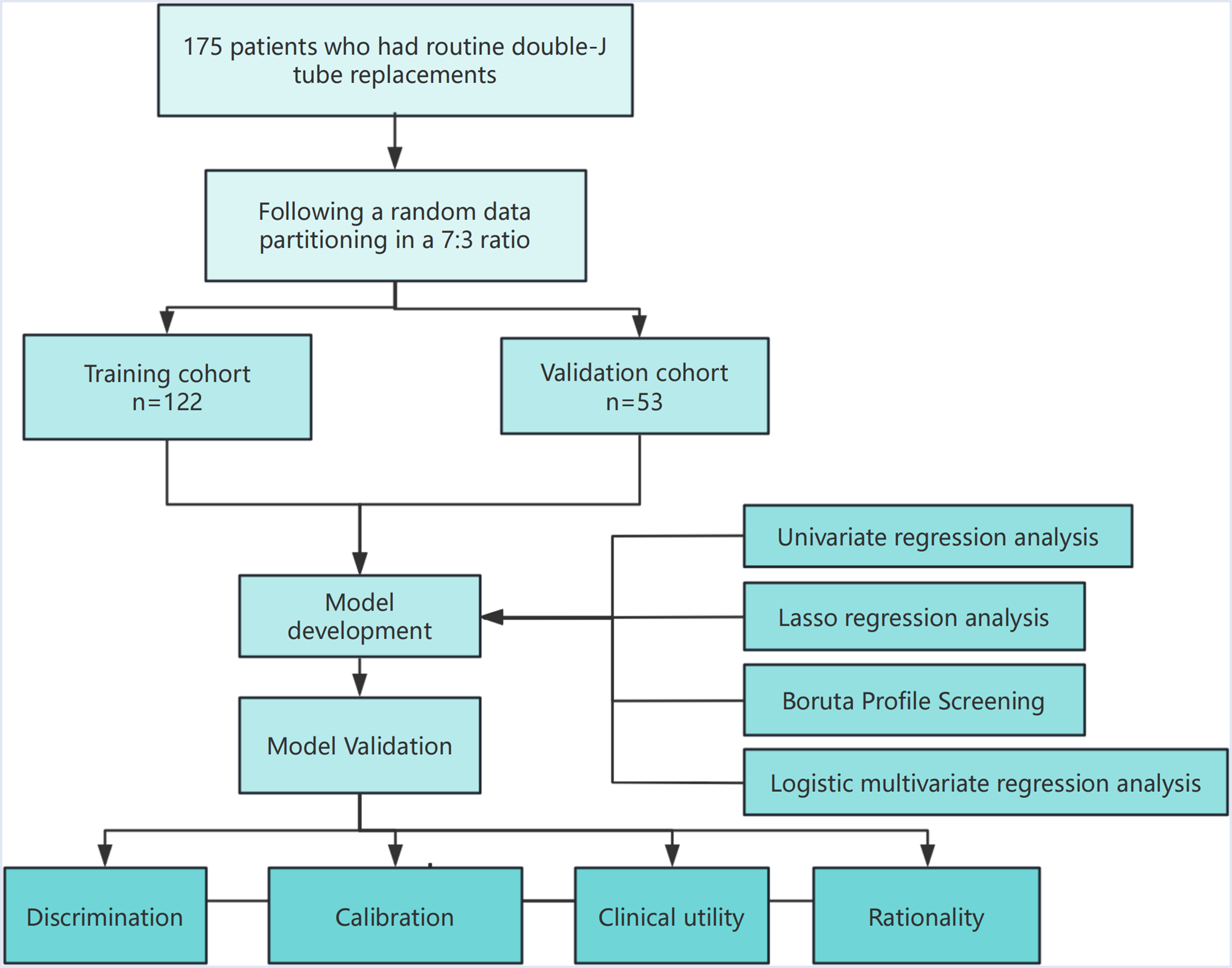
Research pathway diagram.
Analysis of double-J stent encrustation composition and composition ratio.

Baseline characteristics of patients.

BMI: body mass index.
Risk factors associated with double J stent scaling
The univariate analysis revealed that 25 variables were statistically significant (P < 1). The results of the univariate analysis are summarised in Table 3. We employed LASSO regression to simplify the model by selecting variables and a 10-fold cross-validation approach for internal validation, with a pi incidence as the dependent variable and Lambdat as the presence of numerous covariates. The λ filter variable was chosen to be Min. The Lasso method for screening numerical variables is illustrated in Figure 3(A), which employs 16 variable coefficients that vary with penalty coefficients. The coefficient of the initial integration factor is compressed and eliminated from the model when the coefficient is 0. A variable is associated with each row. The target covariates were identified by calculating the area under the ROC curve for 10-fold cross-validation, as illustrated in Figure 3(B). The confidence interval for the covariate of interest at the corresponding λ value is denoted by each red dot, while Lambda. Min and Lambda. Lse are indicated by two lines. We further implemented the Boruta feature selection algorithm on optimal parameters to facilitate the differentiation of scaling patients from non-scaling patients. Ultimately, we selected five variables: BMI, double-J pipe brand, daily water intake, urinary leukocytes and urinary pH (Figure 3(C)). The regression analysis was conducted using the complete inclusion method, and the regression model ultimately contained five factors (Figure 3(D)).

Boruta algorithm feature selection and significant variable selection based on LASSO. (A) Clinical feature LASSO coefficient profiles. (B) Through tenfold cross-validation, the optimal penalisation coefficient lambda was determined in LASSO. The figure illustrates the lambda value of the minimum mean square error. The least absolute shrinkage and selection operator (LASSO) is LASSO. (C) Boruta's feature selection. (D) Univariate logistic regression analysis-identified characteristics are depicted in forest plots.
Univariate logistic regression analysis of risk factors for double-j tube encrustation.

Modal chart model for dual J stent scaling risk
The included patients were divided into training and evaluation groups in a 7:3 ratio using a randomised stratified grouping method (Supplemental data). The risk probability of double-J pipe scab in patients following radical total cystectomy was estimated using individualised nomogram estimation, which was determined by the risk factors selected by Lasso regression, Boruta feature selection algorithm and binary logistic regression (Figure 4). A modal plot is used to score each factor on a scale of 0 to 100, reflecting its regression coefficient concerning the necessity of scab formation in the double-J pipe. The cumulative score is determined by adding the scores associated with each factor to determine the probability of a double-J pipe lesion developing in an individual. This calculation entails the creation of a vertical line from each factor axis that intersects the point axis on the nomogram. The total score generated can be compared to the total score table for an explanation.

Clinical nomograms based on Boruta algorithm feature selection and multiple logistic regression analysis predict the risk of double-J pipe scar in patients with total bladder disease. BMI is the health index. PH is Pondus Hydrogenii.
Validation of nomogram models
The training cohort model (Figure 5(A)) had an AUC of 0.889 (95% CI: 0.8141–0.9641), while the testing cohort model (Figure 5(B)) had an AUC of 0.873 (0.8141–1). The model is accurately calibrated in both the training and testing cohorts. Based on the Hosmer-Lemeshow goodness-of-fit test for the training cohort (χ2 = 6.8641, P = 0.5514) and the validation cohort (χ2 = 7.0163, P = 0.5349), the model was adequately corrected. The calibration analysis indicated that the model was calibrated after 500 Bootstrap internal sampling. The Brier score for the training set was 0.087 with a P-value of 0.985 (> 0.05) (Figure 5(A)), while the scoring for the validation set was 0.086 with a P-value of 0.378 (> 0.05) (Figure 6(B)). The calibration curve demonstrated a robust correlation between the predicted and actual probabilities of occurrence.

The nomogram's evaluation and internal validation. (A) The AUC of the training group (AUC = 0.0.889) and (B) the validation group (AUC = 0.893) showed that the model had a high discrimination ability.

The concordance between the predicted and actual risk of double-J pipe crusting following total bladder surgery was evaluated using calibration curves. (A) The calibration curve of the training group, and (B) the calibration curve of the validation group.
Analysis of clinical practicability and rationality of prediction model
To evaluate the clinical utility of the nomogram, we employed the predicted probability of the calibration plot as a test variable and the incidence of double-J pipe crusting in patients following total bladder surgery as a state variable. As illustrated in Figure 7(A) and (B), we developed a clinical decision curve (decision curve analysis) for the nomogram model. The threshold probability is represented on the X-axis, while the net benefit is on the Y-axis. No patients experienced double-J pipe scab, as indicated by a slender solid black line, while all patients experienced double-J pipe scab, as indicated by a solid grey line. For this investigation, the predictive model's clinical benefits are illustrated by the red curve. The decision curve suggests that the model is advantageous over a relatively extensive threshold probability range. Furthermore, as demonstrated by the clinical impact curves (Figure 7(C) and (D)), the two curves closely overlapped when this predictive model was employed to risk stratify a population of 1000 individuals, suggesting it performed well in clinical applications.

Nomogram model clinical decision curve and clinical impact curve. The decision curve for the training set is denoted by (A), the decision curve for the validation set by (B), the clinical impact curve for the training set by (C), and the clinical impact curve for the validation set by (D).
To conduct a more thorough assessment, we compared the ROC curves of the predicted nomograms with those of models that employed a single predictor. The plausibility of this model is illustrated in Figure 8, which demonstrates that the nomogram area under the curve was greater than that of BMI alone, urinary leukocytes and urinary PH; this indicates that the individual predictors were consistently more minor than the predictive model, emphasising this model's robust performance.
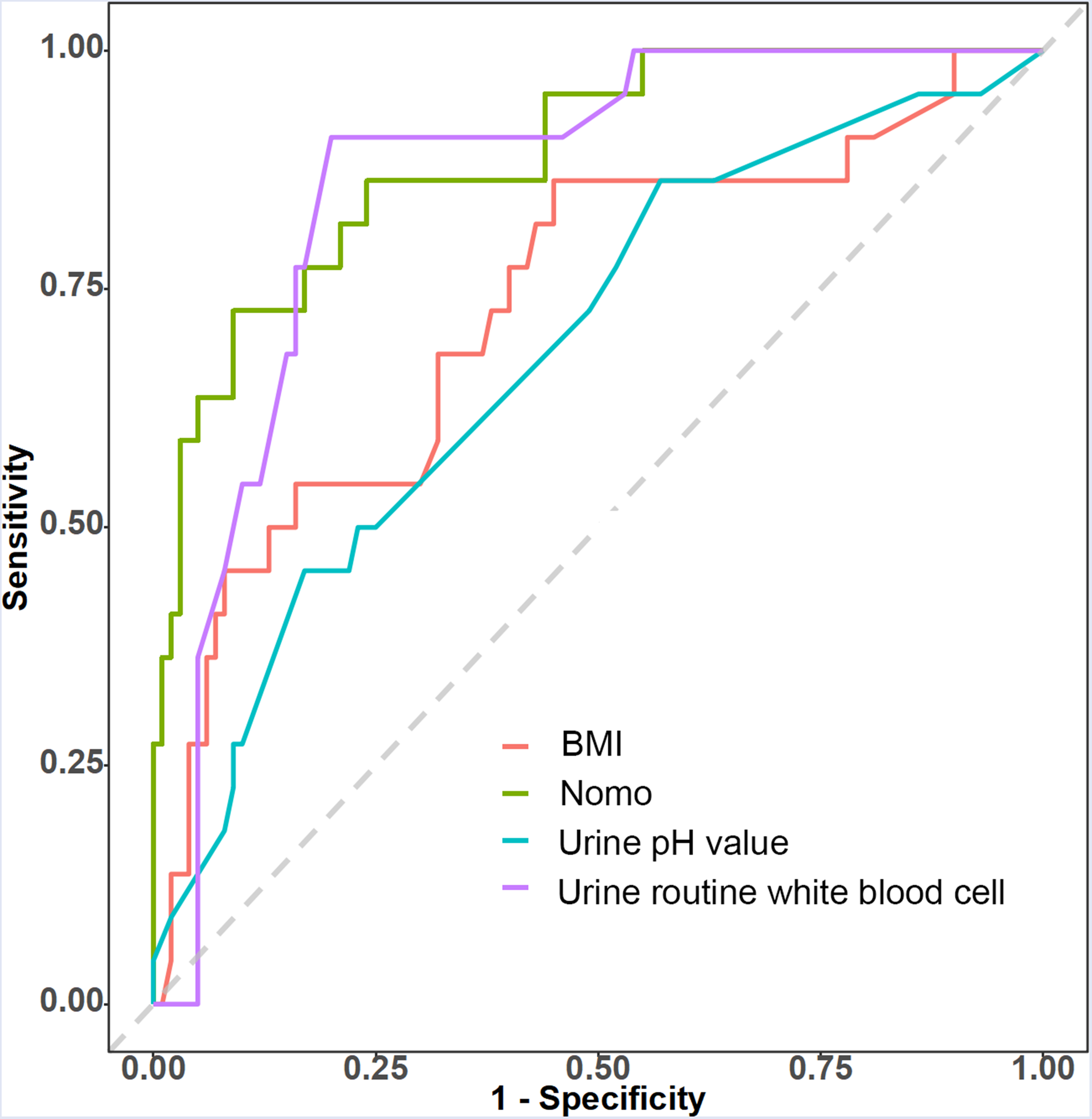
Rationality curve analysis of residual variable risk nomogram.
Discussion
The double-J pipe is a fundamental and valuable instrument for preventing urinary tract obstruction and maintaining urinary tract patency following endourological and open urological procedures. 19 The DJ stent enables the direct drainage of upper urinary tract fluid into the bladder without external diversion. 20 Low back pain, irritating voiding symptoms, haematuria, dysuria, urinary frequency and suprapubic pain are among the complications of short-term stent placement (3–9 weeks). 21 In patients who fail to attend follow-up appointments, complications may also develop after the implantation of chronic stents. Scaling, occlusion, impaction, migration, knotting, stent fracture, spontaneous fragmentation, urine tract stenosis and hydronephrosis are among the delayed complications.22,23
This investigation identified BMI as a risk factor for double-J pipe stones (OR = 1.232). Hypertension and diabetes are prevalent complications of obesity, and they are bidirectionally related to calculi.24,25 Obesity is a factor that can be artificially controlled. Urinary calculi are not a standalone condition; they result from a combination of cardiovascular disease, obesity, diabetes and metabolic syndrome. A cross-sectional study of 605 cases followed for an average of 47 months revealed a direct correlation between BMI and stone disease. This relationship can be employed clinically as a predictor of the development of stone disease. 26 As a result, medical personnel should prioritise patient weight management in clinical practice. During the discharge education, obese patients should develop a personalised weight loss program that encompasses a reasonable diet, consistent exercise and regular monitoring and measurement. In addition, the discharge follow-up should be improved by conducting regular enquiries about implementing the weight loss program to increase patient awareness and attention, thereby facilitating effective weight management.
Abnormal preoperative urinary leukocyte quantification was identified as the risk factor for double-J pipe encrustation (OR = 1.009). As reported in the work of Cao et al., 7 patients with urinary tract infections exhibited a higher proportion of double-J pipe encrustation (92.9%) than those without infections (73.2%). This is an excellent reminder that we must remain vigilant in our clinical work when interacting with patients with abnormal preoperative urinary leukocyte quantification. Medical personnel should act promptly to conduct bacterial culture, identification, drug susceptibility testing, and the rational use of antibiotics for treatment by the examination results in the event of abnormalities. Medical personnel should rationally administer antimicrobial medications at the time of discharge. The entire health management process should be implemented, patient maintenance compliance should be improved, the prevalence of urinary tract infections should be decreased, and patients should be advised to exercise regularly, improve their nutrition and enhance their immunity.
In this study, we discovered that a higher urinary pH was a protective factor against double-J pipe scaling (OR = 0.25). Research has indicated that metabolic acidosis and decreased urine pH contribute to the formation of calcium oxalate stones. 27 Furthermore, our study revealed that the stone composition of double-J pipe scabs was primarily uric acid stones; this served as a reminder to us to monitor the patient's urine pH value in clinical settings and to titrate the pH test strip to record the urine pH value until a stable state was achieved, thereby preventing the formation of uric acid stones.
The development of surface stones was observed to be protected by a water intake of 2000 ml/d in this study (OR = 0.159). Tasian et al. observed that less than 50% of patients maintained an adequate daily fluid intake. 28 Hanrong Li et al. also showed that urine pH was also an independent risk factor for magnesium hexaphosphate stone formation. 29 A comprehensive meta-analysis 30 demonstrated that patients who consumed more than 2000 ml/day had a risk of urinary calculi that was approximately 50% lower than that of patients who drank less than 1000 ml/day (RR = 0.56, 95% CI 0.48 to 0.65, P < 0.001). However, there was still some debate regarding drinking fluids such as tap water, mineral water, juice, tea and coffee. To enhance patient compliance, medical staff should emphasise the importance of consuming a minimum of 2000 ml of water daily and suggest that patients carry graduated or volume-labelled drinking water bottles daily. Additionally, medical staff should enhance follow-up and communication by establishing WeChat groups and conducting live broadcasts on the network to ensure that patients understand the significance of consuming more water to prevent the scaling of double-J pipe.
In addition, this investigation determined that the brand of the double-J pipe was an independent risk factor for double-J pipe crusting (OR = 0.183). We discovered that the Zhongkangshun double-J pipe had a higher risk of scab formation than the fishtail ureteral stent. Consequently, our clinicians were advised to use the fishtail ureteral stent, which has a lower incidence of scab formation, to the greatest extent feasible to prevent the occurrence of the double-J pipe.
This study introduces a clinical nomogram incorporating biomarkers and clinical features to offer a personalised evaluation of the necessity of implementing supplementary measures in patients following total bladder surgery to prevent the formation of double-J pipe scabs. Patients with a large BMI base should be given dietary guidance in conjunction with nutrition departments, with less high purine and high sugar intake and lower urine uric acid levels. Patients should have urine routine reexamination every week after operation, drink more water to colonise less bacteria and preferentially select stents with low scale materials such as fish tail, especially for patients with expected indwelling time of more than 3 months. Patients should drink no less than 2000 ml of water daily. Further drugs should be used to lower uric acid levels in patients with uric acid stones.
Five predictors were evaluated and incorporated into the nomogram. The nomogram's risk prediction capability was 0.889 and 0.873 for the validation set. The primary benefits of this study are threefold: first, the use of straightforward and objective clinical data to develop prediction models; second, the variables used to construct prediction models are easily accessible, which significantly enhances the model's universality and simplifies its implementation in clinical settings. Finally, our nomograms demonstrated significant calibration, consistency and differentiation.
The current study has some limitations. This is a single-centre cross-sectional study with a sample size of only 175 and is retrospective and may have selection bias (e.g. sicker patients are more likely to be included), resulting in caution when extrapolating results to other centres or populations. In addition, we lacked long-term data (more than 1 year) to assess the predictive value of the model for long-term scaling risk. Finally, we performed internal validation exclusively on nomogram models, and subsequent investigations necessitated external validation. In the future, we will further unite 3–5 tertiary hospitals in this region to carry out a large-sample (n ≥ 500) prospective study to verify the universality of the model in different regions and different surgical teams, and supplement the external validation cohort data. To find more risk factors for double-J pipe scab complications in patients after total bladder surgery, in order to take early relevant measures to avoid double-J and further hospitalisation and improve patient discomfort.
Conclusion
In this study, we constructed a prediction model for double-J pipe stones after total bladder surgery. We found five independent factors affecting the occurrence of double-J pipe stones: BMI, preoperative urine routine white blood cell quantification, double-J pipe brand, postoperative water intake and urine PH value, with good predictive ability. Clinical staff were recommended to use this risk prediction model to implement targeted intervention to reduce the probability of double-J pipe stones.
Supplemental Material
sj-pdf-1-sci-10.1177_00368504251363901 - Supplemental material for Predictive model of double-J pipe scab size after radical total cystectomy based on Boruta feature selection and LASSO technique: A retrospective cross-sectional study
Supplemental material, sj-pdf-1-sci-10.1177_00368504251363901 for Predictive model of double-J pipe scab size after radical total cystectomy based on Boruta feature selection and LASSO technique: A retrospective cross-sectional study by Cheng Shen, Haishun Ni, Zhan Chen, Junjie You and Bing Zheng in Science Progress
Supplemental Material
sj-docx-2-sci-10.1177_00368504251363901 - Supplemental material for Predictive model of double-J pipe scab size after radical total cystectomy based on Boruta feature selection and LASSO technique: A retrospective cross-sectional study
Supplemental material, sj-docx-2-sci-10.1177_00368504251363901 for Predictive model of double-J pipe scab size after radical total cystectomy based on Boruta feature selection and LASSO technique: A retrospective cross-sectional study by Cheng Shen, Haishun Ni, Zhan Chen, Junjie You and Bing Zheng in Science Progress
Footnotes
Ethics approval and consent to participate
The research involving human subjects was reviewed and approved by the Medical Ethics Review Committee of the First People’s Hospital of Nantong (2023KT212), in strict adherence to the principles of the Declaration of Helsinki, and informed consent was obtained from all subjects.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Author contributions
CS wrote the first draft of the manuscript. HSL, ZC and JJY collected and analysed the data. JJY and BZ supervised the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was supported by Medical Research Project of Nantong Health Commission (MS2022017), Jiangsu Health Commission (Z2022014), Youth Project of Health Commission of Nantong City (QN2022017), Yaodong Shenzhou - Pharmaceutical Research Capacity Building Fund Project (2024-KY002-01), Nantong University Clinical Medicine Special Scientific Research Fund Project (2024LQ019), and Basic Research and Social Minsheng Plan Project (MS22022085).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data is provided within the manuscript or supplementary information files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.