
Abstract
Chronic obstructive pulmonary disease (COPD) increases the global disease burden due to its diverse adverse health effects on the respiratory and cardiovascular systems. This study aimed to elucidate the potential indicators of length of stay (LOS) and pharmacotherapy advice among COPD patients. Thereafter, hospitalized COPD patients with clinical records and respiratory and cardiovascular pharmacotherapy advice were retrospectively collected from a tertiary hospital between April 2017 and September 2020, and the determinants of LOS and cardiovascular pharmacotherapy advice were explored using regression analyses. Overall, 475 patients with COPD were recruited and stratified according to exacerbation and presence of Cor pulmonale (CP). The extended LOS, increased B-type natriuretic peptides (BNP), and a higher percentage of cardiovascular pharmacotherapy advice were observed in COPD with CP regardless of exacerbation, although the percentage of respiratory prescriptions was comparable. The presence of CP indicated a longer LOS (B = 1.850, p < 0.001) for COPD regardless of exacerbation. Meanwhile, elevated BNP levels indicated cardiovascular pharmacotherapy advise for both COPD in exacerbation (OR = 1.003, p = 0.012) and absence of exacerbation (OR = 1.006, p = 0.015). Moreover, advice for trimetazidine use for COPD in exacerbation (OR = 1.005, p = 0.002) has been suggested. Therefore, CP appears to be an important comorbidity resulting in extended LOS for COPD, which is likely to be advised with cardiovascular pharmacotherapy, which might be guided through BNP monitoring.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) raises clinical and public health concerns due to its rising incidence, prevalence, morbidity and mortality. 1 COPD is the third leading cause of mortality and increases the economic burden and compromises the quality of life in China. 2 Accordingly, further investigation is warranted to comprehensively characterize clinical features and therapy choices among COPD patients to improve health quality.
COPD not only has negative impacts on the respiratory system, but also raises health concerns regarding comorbidities. The death and disability-adjusted life-years of COPD appear to be ascribed to the two dominant environmental risk factors, smoking and ambient particulate matter. 3 Hospital admission and the length of stay (LOS) are extended for COPD patients in the presence of an increased number of comorbidities and exacerbation.4,5 Meanwhile, COPD exacerbation, hyperinflation, hypoxaemia, and systemic inflammation have been proposed as potential mediators of adverse cardiovascular events, which should be explored in both clinical and research settings so as to select reliable and accessible parameters to assist clinical outcome improvement through an integrated approach dealing with COPD and concomitant cardiovascular disorders.6,7
Reduced respiratory symptom burden, improved airway and lung function, mitigated airway inflammation, and treatment of comorbidities are beneficial for COPD.8,9 Nevertheless, the discrepancy between medication recommendations and COPD diagnosis is still evident,10–12 suggesting the necessity to demonstrate respiratory and cardiovascular pharmacotherapy for COPD in the real world. It should be noted that the exploration of factors in associated with the preferred medication choice could be helpful in updating effective COPD management.13,14
Taken together, this study aimed to elucidate the clinical characteristics and potential determinants relevant to LOS and pharmacotherapy advice among COPD patients, which might be valuable in optimizing COPD management.
Materials and methods
Study population
Hospitalized COPD patients between April 2017 and September 2020 were selected from a medical record system at the First People's Hospital of YongKang, Zhejiang, China. COPD inpatients were recruited in this observational retrospective study if a previous medical document ascertaining COPD diagnosis was available or a post-bronchodilator FEV1/FVC < 0.70 was identified during their hospital admission. 15 Thereafter, COPD exacerbation was recorded if an acute worsening of respiratory symptoms that resulted in additional medication was evident. 16 This study was approved by Ethics Committee of Medical Research of the First People's Hospital of YongKang, and the requirement for patient consent was waived due to the nature of the retrospective analysis of the already available data without disclosure of personal information. All procedures during this investigation were in accordance with the requirements of the Declaration of Helsinki.
Data collection
Particulate matter <2.5 μm (PM2.5) concentration at Yongkang between April 2017 and September 2020 was publicly available in the monthly environmental quality report as documented at Jinhua Municipal Bureau of Ecology and Environment (http://sthjj.jinhua.gov.cn/). The monthly mean PM2.5 concentration was retrieved and used to calculate quarterly mean PM2.5 concentration in each year.
The records of lung ventilation and diffusion tests using the JAEGER lung function instrument, bacterial flora analysis in the sputum with VITEK 2 COMPACT automatic bacterial culture system, partial pressure of carbon dioxide (PaCO2), partial pressure of oxygen (PaO2), and standardized base excess (BE) using an ABL800 FLEX blood gas analyzer were collected. Moreover, the measurements of routine blood examination with SYSMEX XN-1000/XE-2100 automatic haematology analyzer, B-type natriuretic peptides (BNP), cardiac troponin (cTnI) and myoglobin (Mb) using Pylon Immunochemistry system ET Healthcare.Inc, immunoglobulin, complement components, C-reaction protein (CRP) with SIEMENS BN™II System automatic protein analyzer, and pre-albumin using SIEMENS ADVIA 2400 automatic biochemistry analyzer were retrieved, respectively. All the data mentioned above referred to the results of the corresponding examinations at the time of hospital admission.
The cardiovascular abnormalities analyzed in this study were hypertension and Cor pulmonale (CP). Hypertension was determined in the presence of diastolic blood pressure > 140 mmHg and/or systolic blood pressure > 90 mmHg. CP was diagnosed based on its distinct characteristics, including cardiomegaly confined predominantly to the right ventricle with the form of dilatation, hypertrophy, or both, and pulmonary arterial hypertension, 17 which was evaluated with the aid of ultrasonic cardiogram and electrocardiogram.
The medication advice for COPD inpatients upon discharge from the hospital was analyzed in this study. Briefly, respiratory prescriptions were divided into three categories, namely expectorant and anti-asthma remedy, bronchodilator/corticosteroids, the combination of expectorant and anti-asthma remedy, and bronchodilator/corticosteroids, respectively. Cardiovascular pharmacotherapy includes trimetazidine, angiotensin-receptor blockers, statins, β1-blocker, angiotensin II receptor antagonists, and calcium antagonists, respectively.
Statistical analysis
Statistical analyses of the data were performed using IBM® SPSS® Statistics (version 26.0) and GraphPad Prism (Version 8.2.1). Quantitative and qualitative variables were expressed as median with interquarile25−75 and number with frequency, respectively. Comparisons between two variables were determined using Mann-Whitney U tests, while the distributions of the variables were analyzed using Chi-square tests or Fisher's exact tests. The determinants of LOS and pharmacotherapy advice were explored using multivariate linear and logistic regression models where applicable. A p-value <0.05 was considered as statistically significant.
Results
Study population and PM2.5 level stratified by each quarter per year
A total of 475 COPD patients were documented between 2017 and 2020, including 257 cases with exacerbation and 218 cases without exacerbation. The percentage of COPD exacerbation cases per year was 63.8% (37/58) in 2017, 37.4% (68/182) in 2018, 62.7% (111/177) in 2019, and 70.7% (41/58) in 2020. Meanwhile, the highest frequency of COPD exacerbation cases at each quarter per year was 40.5% (15/37) at 4th quarter in 2017, 30.9% (21/68) at 4th quarter in 2018, 29.7% (33/111) in the 3rd quarter in 2019, and 48.8% (20/41) at 4th quarter in 2020. Additionally, the highest and lowest mean PM2.5 level at each quarter per year were 39 μg/m3 at 4th quarter and 24 μg/m3 at 3rd quarter in 2017, 49 μg/m3 at 1st quarter and 23μg/m3 at 3rd quarter in 2018, and 49 μg/m3 at 4th quarter and 23 μg/m3 at 3rd quarter in 2019. Nonetheless, the mean PM2.5 level at each quarter was 26 μg/m3 in 2020 (Figure 1).

The number of COPD patients and mean PM2.5 levels stratified by each quarter per year. COPD, Chronic obstructive pulmonary disease; PM2.5, Particulate matter <2.5 μm.
Characteristics of COPD patients by exacerbation and CP
As shown in Table 1, there were no significant differences in sex, smoking rate, and self-reported duration of cough, sputum production, and shortness of breath between COPD patients with and without exacerbation. The frequency of impaired lung function and deterioration of lung diffusing capacity, positive bronchial dilation test, and abnormal bacterial flora in the sputum were also comparable between COPD patients with and without exacerbation. Nevertheless, younger age, lower CRP and BNP levels, higher pre-albumin levels and CP rate, and shorter LOS were evident in COPD patients with exacerbation than in those without exacerbation.
Characteristics of COPD patients with and without exacerbation.

Among COPD patients without exacerbation, there were longer self-reported duration of cough, sputum production and shortness of breath, lower pre-albumin; higher PaCO2, BE, and BNP; and longer LOS for cases with CP than for those without CP (Table 2). Meanwhile, among COPD patients with exacerbation, there were lower positive bronchial dilation test rates, higher white blood cell (WBC), neutrophil, eosinophils, N/L, P/L, PaCO2, BE, BNP, and hypertension rate, and longer LOS for patients with CP than for those without CP (Table 3).
Characteristics of COPD patients without exacerbation stratified by Cor pulmonale.

Characteristics of COPD patients with exacerbation stratified by Cor pulmonale .

Pharmacotherapy advice for COPD patients by exacerbation and CP
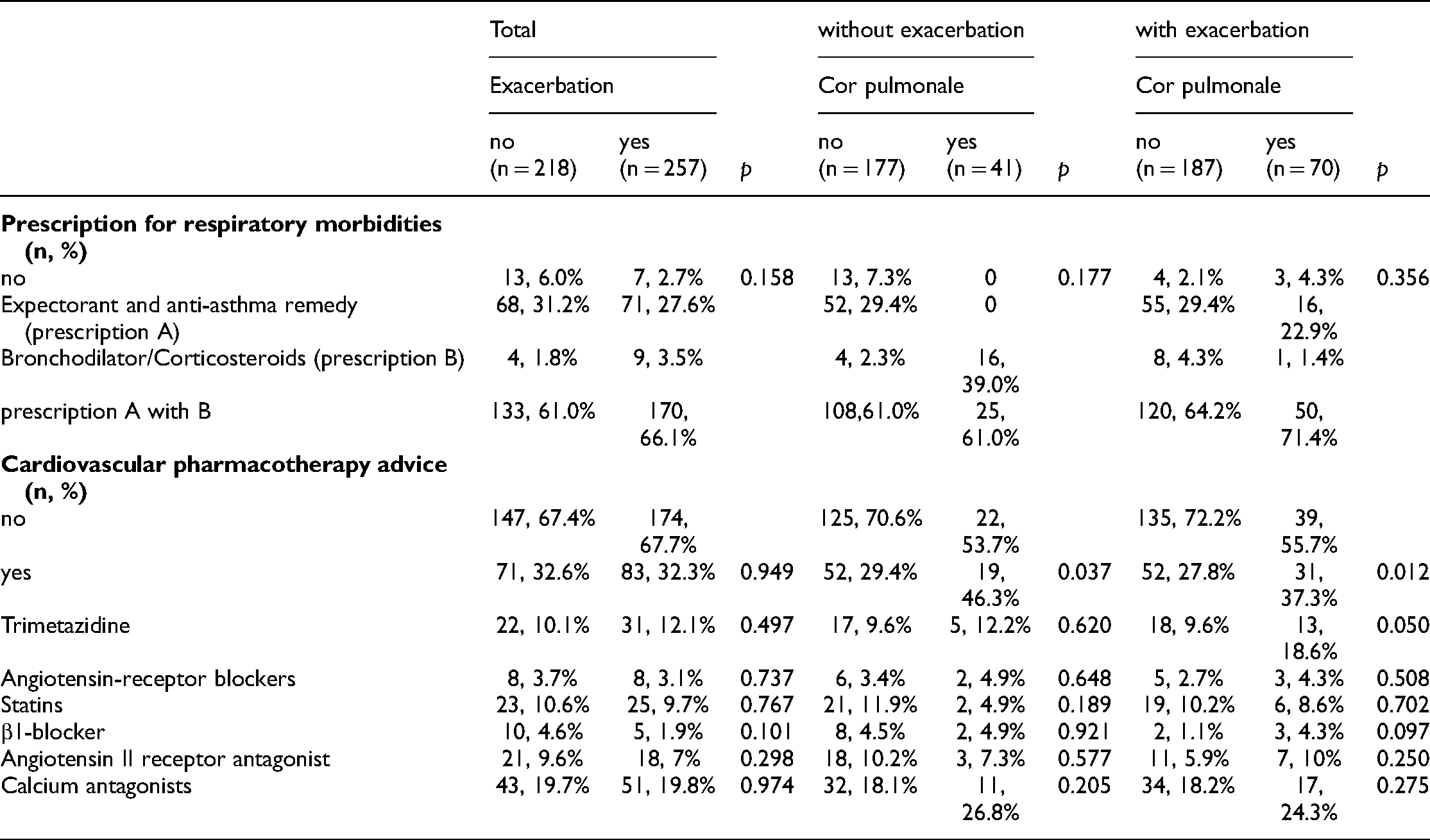
Table 4 demonstrates that the most common respiratory pharmacotherapy was a combination of expectorant and anti-asthma remedy and bronchodilator/corticosteroids, followed by expectorant and anti-asthma remedy alone and bronchodilator/corticosteroids alone, regardless of exacerbation and CP. Meanwhile, cardiovascular pharmacotherapy for COPD without exacerbation was much more frequently advised for patients with CP than for those without CP (46.3% and 29.4%, p = 0.037). Similarly, among COPD patients with exacerbation, a higher percentage of cardiovascular pharmacotherapy was also evident in patients with CP than in those without CP (37.3% and 27.8%, p = 0.037). Nonetheless, the frequency of cardiovascular pharmacotherapy was comparable between COPD patients with and without exacerbation regardless of CP (p = 0.949). Further comparisons of specific cardiovascular pharmacotherapy demonstrated that among COPD patients with exacerbation, the frequency of trimetazidine advice was 18.6% and 9.6% for cases with and without CP, respectively (p = 0.050).
Prescription pattern among chronic obstructive pulmonary disease patients by exacerbation and Cor pulmonale.
Determinants associated with LOS and cardiovascular pharmacotherapy for COPD patients
The results of the multivariate linear regression showed that the increment in age, CRP, PM2.5, and the presence of CP were marginally but significantly correlated with the extended LOS for COPD regardless of exacerbation. Increased age and PM2.5 remained indicators of extended LOS for COPD without exacerbation, while age, neutrophil count, and PM2.5 positively correlated with LOS for COPD with exacerbation (Table 5).
Variables associated with length of stay at hospitals for chronic obstructive pulmonary disease patients by exacerbation and Cor pulmonale.
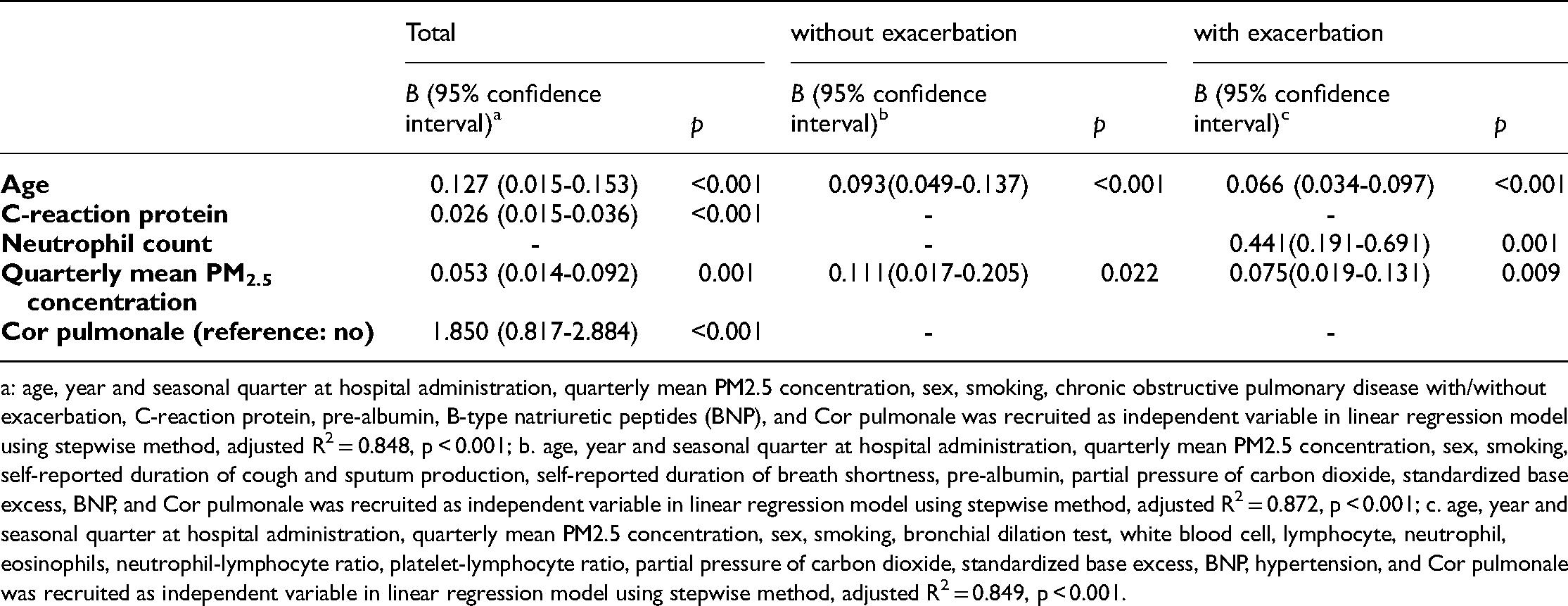
a: age, year and seasonal quarter at hospital administration, quarterly mean PM2.5 concentration, sex, smoking, chronic obstructive pulmonary disease with/without exacerbation, C-reaction protein, pre-albumin, B-type natriuretic peptides (BNP), and Cor pulmonale was recruited as independent variable in linear regression model using stepwise method, adjusted R2 = 0.848, p < 0.001; b. age, year and seasonal quarter at hospital administration, quarterly mean PM2.5 concentration, sex, smoking, self-reported duration of cough and sputum production, self-reported duration of breath shortness, pre-albumin, partial pressure of carbon dioxide, standardized base excess, BNP, and Cor pulmonale was recruited as independent variable in linear regression model using stepwise method, adjusted R2 = 0.872, p < 0.001; c. age, year and seasonal quarter at hospital administration, quarterly mean PM2.5 concentration, sex, smoking, bronchial dilation test, white blood cell, lymphocyte, neutrophil, eosinophils, neutrophil-lymphocyte ratio, platelet-lymphocyte ratio, partial pressure of carbon dioxide, standardized base excess, BNP, hypertension, and Cor pulmonale was recruited as independent variable in linear regression model using stepwise method, adjusted R2 = 0.849, p < 0.001.
Cardiovascular pharmacotherapy appeared to be advised for patients with high BNP levels and short duration of cough and sputum production among COPD patients without exacerbation. Meanwhile, female sex, high BNP levels, and the presence of hypertension were associated with cardiovascular pharmacotherapy advice for COPD exacerbation. High BNP levels remained a potential indicator of trimetazidine advice for COPD patients with exacerbation (Table 6).
Potential determinants of cardiovascular pharmacotherapy advice for chronic obstructive pulmonary disease patients.

a. age, year and seasonal quarter at hospital administration, quarterly mean PM2.5 concentration, sex, smoking, self-reported duration of cough and sputum production, self-reported duration of breath shortness, pre-albumin, partial pressure of carbon dioxide, standardized base excess, B-type natriuretic peptides (BNP), Cor pulmonale, length of stay at hospitals, and prescription for respiratory morbidities was recruited as covariable in multivariate logistic regression model using forward stepwise method, R2 = 0.429, p < 0.001; b. age, year and seasonal quarter at hospital administration, quarterly mean PM2.5 concentration, gender, smoking, bronchial dilation test, white blood cell, lymphocyte, neutrophil, eosinophils, neutrophil-lymphocyte ratio, platelet-lymphocyte ratio, partial pressure of carbon dioxide, standardized base excess, BNP, hypertension, Cor pulmonale, and length of stay at hospitals, and prescription for respiratory morbidities was recruited as covariable in multivariate logistic regression model using forward stepwise method, R2 = 0.574, p < 0.001; c. age, year and seasonal quarter at hospital administration, quarterly mean PM2.5 concentration, gender, smoking, bronchial dilation test, white blood cell, lymphocyte, neutrophil, eosinophils, neutrophil-lymphocyte ratio, platelet-lymphocyte ratio, partial pressure of carbon dioxide, standardized base excess, BNP, hypertension, Cor pulmonale, and length of stay at hospitals, and prescription for respiratory morbidities was recruited as covariable in multivariate logistic regression model using forward stepwise method, R2 = 0.789, p < 0.001.
Discussion
This study found that COPD patients with concurrent CP have extended LOS independent of exacerbation and are likely to be advised with cardiovascular pharmacotherapy in the presence of BNP elevation during hospital admission.
The presence of CP is much more frequently detected in COPD patients with exacerbation than in those without exacerbation (27.2% vs. 18.8%) as reported here, and the prevalence of CP was 48.1% for advanced COPD as documented elsewhere, 18 which is consistent with the conception that CP is typically the result of chronic lung disorder exacerbation. 17 The sensitivity and specificity of CRP in discriminating COPD exacerbation could reach >70% and 82%, respectively, when the cut-off value was defined as approximately 11 mg/L.19,20 However, CRP cut-off value is above the median CRP level of COPD patients with exacerbation (3.49 mg/L) and without exacerbation (7.37 mg/L), as observed in this study. Meanwhile, higher CRP levels may not be suggestive of COPD severity and exacerbation history. 21 Moreover, the distinctive endotype of COPD and the aetiology of exacerbation may also influence CRP levels. There are eosinophilic and bacterial exacerbations displaying clinical differences, and high CRP has been considered as an airway bacterial exacerbation marker in COPD patients. 22 However, elevation of CRP in COPD patients without exacerbation in this study could not be ascribed to the conception of airway bacterial exacerbation, because the abnormal bacterial flora rate in sputum of COPD patients with and without exacerbation was around 16% without significant difference in this study. Alternatively, CRP values increased with declining eosinophil count, which might be common in COPD patients, especially for smokers.23,24 This might not be a possible explanation for the intriguing changes in CRP levels between COPD patients with and without exacerbation, as these two groups of patients had comparable smoking rates and eosinophil counts. It should be noted that high CRP/low pre-albumin and low CRP/high pre-albumin levels were documented in exacerbated COPD and stable COPD, respectively, 25 while an inverse observation was evident in COPD with and without exacerbation as presented here, raising a possible interference of pre-albumin on CRP values in COPD.
The characteristics of the circulating inflammation index and peripheral blood cell counts appear to be complicated by the presence of CP in COPD. The absence of influence of CP on the WBC count was reported in COPD regardless of exacerbation. 26 Despite the possible null effect of CP on WBC and other investigated inflammatory cell counts in the peripheral blood of COPD patients without exacerbation, CP likely increased some inflammatory parameters (e.g. WBC, neutrophil, N/L, P/L), but reduced lymphocyte count without changes in CRP levels among COPD patients with exacerbation in this investigation. This may be partially explained by the notion that an increase in N/L has been suggested to be a valuable indicator of COPD-specific inflammatory status, which plays a role in COPD-associated pulmonary hypertension and the resulting cardiovascular disorders.27,28
Cardiovascular comorbidity (e.g. congestive heart failure), older age, and high CRP concentration (e.g. >100 mg/L) have been demonstrated to be indicators of longer LOS among COPD patients especially during exacerbation.22,29 COPD exacerbation events may be increased due to atmospheric particulate matter pollution. 30 The quarterly mean PM2.5 concentration data collected in this study are within the moderate range of PM2.5 concentrations (16–50 μg/m3), exhibiting minimal health impact on patients. 30 Without consideration of exacerbation status, COPD patients with coexisting CP had longer LOS in this study, suggesting the importance of monitoring CP in COPD management.
One critical COPD pharmacotherapy is bronchodilators and corticosteroids, which are prescribed through the evaluation of exacerbation and respiratory symptom burden. 8 The percentage of mono-prescriptions of bronchodilators and corticosteroids was comparable between COPD patients with and without exacerbation (3.5% and 1.8%, respectively), while a high percentage of bronchodilators and corticosteroid prescriptions was 39.0% for COPD without exacerbation but with CP, rather than COPD with both exacerbation and CP (1.4%). Because of the role of expectorants in mucus expectoration and the mitigation of cough by anti-asthma medications, the prescription of expectorants could reach 20% for COPD patients.31,32 The persistent cough, sputum production and shortness of breath in our COPD patients with and without exacerbation or CP suggested the potential benefit of expectorants and anti-asthma medications with a prescription rate ranging from 22.9% to 31.2%. Nonetheless, it is worth mentioning that at least 61% of our COPD patients were simultaneously prescribed expectorant and anti-asthma medications, bronchodilators, and corticosteroid, which is in line with the combination of pharmacological strategies for obstructive lung diseases. 32
Cardiovascular pharmacotherapy is also desirable for COPD. 6 Our study demonstrated that COPD exacerbation itself does not influence cardiovascular prescription advice. However, patients with CP were likely to be advised with cardiovascular pharmacotherapy, independent of exacerbation. We noticed that BNP, rather than other cardiac markers (e.g. cTnI, Mb), increased in COPD with CP, indicating a possible role of BNP in reflecting the presence of CP in COPD.18,33 Further logistic regression revealed that BNP is a potential indicator of cardiovascular pharmacotherapy advice for all COPD patients, although hypertension is another factor correlating with cardiovascular prescription for COPD patients with exacerbation. Indeed, BNP is a natriuretic peptide, which is an emerging marker in the field of cardiovascular pharmacotherapy. 34 Elevated BNP levels appeared to be suggestive of trimetazidine prescription for COPD patients as reported here, which might be tentatively explained by the benefit of trimetazidine in BNP downregulation in CP patients. 35 Delineating the benefit of BNP monitoring for COPD patients with cardiovascular pharmacotherapy advice in further prospective investigations remains.
There are some limitations to be addressed. This was a retrospective cross-sectional investigation to characterize key clinical parameters and pharmacotherapy advice among 475 COPD patients from a single tertiary hospital between 2017 and 2020. The accessible and achievable parameters as demonstrated in our regression analyses might not definitively provide a causal effect on cardiovascular prescription, which remains to be the scope of the prospective study. Additionally, the absence of daily PM2.5 concentrations and other air pollutants precluded us from comprehensively interpreting the potential effect of atmospheric pollution on pathophysiological features of COPD patients. Nonetheless, these issues might be partially resolved when the variation of the year and season and the calculated quarterly mean PM2.5 concentration was considered as a covariate in our regression analyses, because the recruited COPD patients were local citizens. Further studies with sophisticated air pollutant monitoring data are warranted, which might be helpful in mitigating the incidence of adverse pathophysiological events in local COPD patients from an environmental perspective. Moreover, the significant but marginal role of BNP in suggesting cardiovascular pharmacotherapy advice (especially for trimetazidine) needs to be examined in a larger-scale COPD population, which might guide personalized medication for these kinds of COPD patients.
Conclusion
CP should be carefully examined among COPD patients regardless of exacerbation, which appears to be a critical comorbidity resulting in extended LOS. In addition to prescription targeting respiratory symptoms, patients with COPD are also likely to be advised with cardiovascular pharmacotherapy, which could be guided through BNP monitoring.
Footnotes
Author contributions
Data curation, Formal analysis, Methodology, Writing-review & editing, HF; Data curation, Methodology, Writing - review & editing, MZ, HZW, CSZ, XY; Data curation, Writing - review & editing, HLX; Conceptualization, Formal analysis, Methodology, Writing -original draft, Writing-review & editing, Supervision, MY. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the special scientific research fund of institutes in Zhejiang (grant number YS2021004).