
Abstract
Background
Pulpotomy is widely used in primary and immature permanent teeth, but its effectiveness in mature permanent teeth with irreversible pulpitis remains controversial.
Objective
To identify and evaluate the existing systematic reviews of randomized controlled trials (RCTs) assessing pulpotomy as a treatment for irreversible pulpitis in mature permanent teeth.
Methods
A protocol-guided search was conducted across PubMed, ProQuest, EMBASE, and Cochrane up to March 2024, targeting systematic reviews based on RCTs. Eligibility, selection, data extraction, and risk of bias assessment were performed independently by two reviewers. Quality was assessed using the AMSTAR 2 tool.
Results
Of the 52 articles retrieved, only one systematic review met inclusion criteria. The review included four RCTs involving 874 patients. Reported clinical success rates ranged from 81.2% to 98.19%, and radiographic success ranged from 38.4% to 95%, with the highest outcomes observed for calcium-enriched mixture and mineral trioxide aggregate. The AMSTAR 2 assessment rated the systematic review as critically low quality.
Conclusion
Current evidence from systematic reviews is insufficient to definitively recommend pulpotomy for irreversible pulpitis in mature permanent teeth. However, favorable clinical outcomes and the minimally invasive, cost-effective nature of the procedure suggest that pulpotomy may serve as a practical alternative to root canal treatment in select cases. High-quality RCTs and systematic reviews are urgently needed to strengthen the evidence base.
Keywords
Introduction
Rationale: Pulpotomy is a well-established vital pulp therapy procedure traditionally indicated for primary teeth and immature permanent teeth with pulp exposures due to caries or trauma. Foundational studies by Cvek and others in the 1970s and 1980s demonstrated that the removal of inflamed coronal pulp tissue, followed by placement of a biocompatible material, could preserve pulp vitality and support continued root development. 1 Early success was attributed to materials like calcium hydroxide, which promoted reparative dentin formation. 2 Over time, advancements in pulp biology and the introduction of more predictable materials led to renewed interest in applying pulpotomy to mature permanent teeth as well. 3
The treatment of irreversible pulpitis has evolved significantly. Guidelines from prominent endodontic associations, such as the American Association of Endodontists and the European Society of Endodontology, suggest that pulpotomy can be a viable option even for teeth traditionally considered beyond repair, and that a diagnosis of irreversible pulpitis is no longer mandatory for performing a pulpectomy.4,5 This reflects a shift toward less invasive vital pulp therapies aimed at preserving the health and vitality of the pulp and periapical tissues, even in cases of irreversible pulpitis, carious exposures, or traumatic injuries. 6 Notably, a noninferiority randomized clinical trial has demonstrated that pulpotomy may yield better outcomes than traditional root canal treatment in fully developed molars affected by irreversible pulpitis. 7
Full pulpotomy has gained recognition as a viable alternative in the management of irreversible pulpitis, particularly due to advancements in materials and techniques. Traditional root canal therapy involves complete removal of the pulp, whereas full pulpotomy selectively removes only the inflamed coronal pulp while preserving the vitality of the radicular pulp. Recent studies, such as Tran et al. 8 report nearly 100% clinical success and 93.8% radiographic success for biodentine pulpotomy in mature teeth with irreversible pulpitis over a one-year follow-up. Additionally, a systematic review by Ather et al. 9 found that full pulpotomy often yields superior outcomes compared to partial pulpotomy, supporting its role as a definitive treatment option.
The introduction of biocompatible materials, particularly calcium silicate-based cements such as biodentine and mineral trioxide aggregate (MTA), has significantly improved the predictability of pulpotomy outcomes. For instance, Qudeimat et al. 10 reported MTA pulpotomy success rates ranging from 95% to 100% in cases of irreversible pulpitis. These materials promote healing by creating a bioactive environment favorable for pulp regeneration, as supported by various clinical trials.11,12 Furthermore, the conservative nature of pulpotomy aligns with the principles of minimally invasive dentistry, aiming to preserve both tooth structure and pulp vitality while achieving therapeutic success. 13
Although several case series, randomized controlled trials (RCTs), and systematic reviews have been published on this subject, an overview of systematic reviews based exclusively on RCTs (Oxford Level 1a evidence) 14 is lacking. Therefore, our study represents the first overview of systematic reviews based exclusively on RCTs for pulpotomy in teeth with irreversible pulpitis, providing a high-level synthesis to support evidence-based clinical decision-making.
Objectives
To identify and evaluate systematic reviews of RCTs investigating pulpotomy for irreversible pulpitis in fully developed permanent teeth and to assess the quality of the available evidence.
Methods
This overview of systematic reviews was conducted and reported in accordance with the Preferred Reporting Items for Overviews of Reviews guidelines. 15
Eligibility criteria
Inclusion criteria:
Systematic reviews based solely on RCTs; Studies evaluating pulpotomy in fully developed permanent teeth with a diagnosis of irreversible pulpitis; Studies published in the English language.
Exclusion criteria:
Systematic reviews not based exclusively on RCTs; Studies involving partial pulpotomy or direct/indirect pulp capping; Studies involving immature teeth; Studies published in languages other than English.
Definition of systematic review as used in the inclusion criteria
For the purpose of this overview, a systematic review was defined as a secondary study that used a clearly formulated research question and employed a predefined, transparent, and reproducible methodology—including a comprehensive search across multiple databases, explicit inclusion and exclusion criteria, and a formal risk of bias or quality assessment of the included RCTs. Only systematic reviews that exclusively included RCTs and synthesized their results were considered eligible for inclusion.
Information sources
Electronic searches were conducted in the following databases: PubMed, EMBASE, ProQuest, and the Cochrane Library, covering literature up to March 2024.
Search strategy
The search used the keywords: “pulpotomy” AND “mature permanent teeth” AND “irreversible pulpitis,” with filters applied for systematic reviews and English language.
Selection process
Two authors independently screened the titles, abstracts, and full texts of all retrieved articles. Discrepancies were resolved through discussion and consensus. As only one eligible systematic review was included, the issue of population or data overlap was not applicable.
Data collection process
Data were independently extracted by two reviewers using a structured format. Extracted elements included:
Author and publication year Country of origin of the systematic review Search period and number of databases searched Number of included studies and total patients (with dropouts) Follow-up duration and age range of participants Materials evaluated Interventions/comparisons included in the SR Clinical and radiographic success rates per material Bias assessment of included RCTs Outcome conclusions reported in the review Tool used for SR quality assessment (if any) Overall AMSTAR 2 rating.
No significant discrepancies in data extraction were noted.
Risk of bias assessment
The risk of bias in the included systematic review was independently assessed by two trained reviewers using the AMSTAR 2 tool. According to AMSTAR 2, systematic reviews are classified as:
High quality (no or one noncritical weakness) Moderate quality (more than one noncritical weakness) Low quality (one critical flaw, regardless of other weaknesses) Critically low quality (more than one critical flaw).
The included SR was rated as critically low quality. No reassessment of individual RCTs was performed. No supplemental primary studies were included.
Synthesis methods
Due to the inclusion of only one systematic review with heterogeneous interventions and outcome measures, a narrative synthesis was conducted. No meta-analysis or sensitivity analysis was applicable.
Results
Systematic review selection
A total of 52 articles were identified, of which eight were duplicates. After screening 44 titles and abstracts, 37 were excluded. The remaining seven full-text articles were reviewed, and six were excluded for not meeting eligibility criteria. Ultimately, one systematic review 16 was included. Figure 1 illustrates the flow diagram, and Table 1 lists excluded studies with reasons.

Flow diagram outlining the search and selection process for systematic reviews included in the overview of reviews.
Excluded studies and reasons for exclusion.

Characteristics of the included systematic review
The included review evaluated four RCTs involving 874 patients (148 lost to follow-up), published between 2000 and April 2021. Interventions assessed included calcium-enriched mixture (CEM), MTA, platelet-rich fibrin (PRF), calcium hydroxide (CH), and RCT as a comparison. Follow-up ranged from one to two years, with patient age spanning nine to 65 years. No tool for quality assessment of primary studies was reported. Table 2 lists the detailed characteristics of the included systematic review.
Systematic review characteristics.
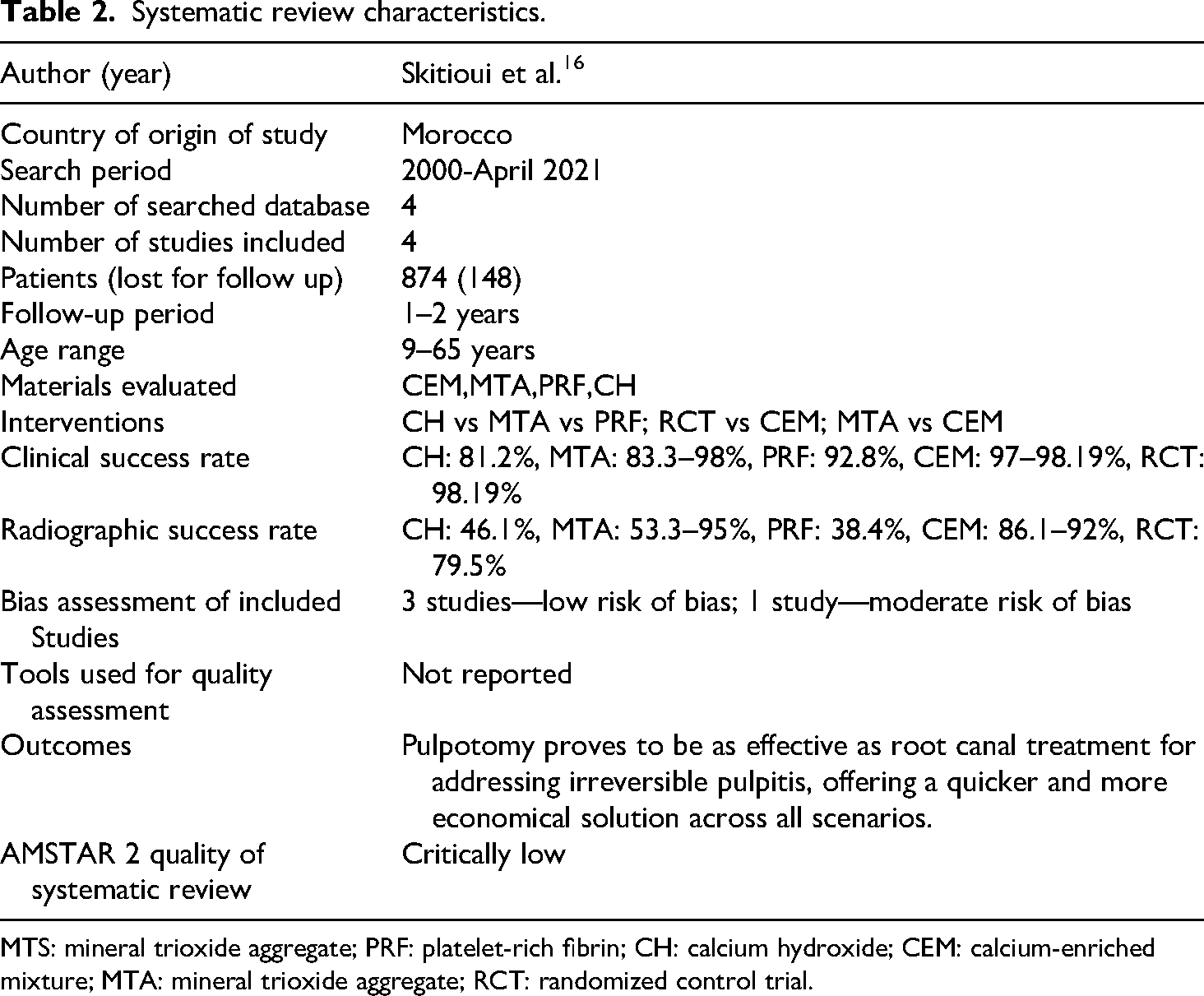
MTS: mineral trioxide aggregate; PRF: platelet-rich fibrin; CH: calcium hydroxide; CEM: calcium-enriched mixture; MTA: mineral trioxide aggregate; RCT: randomized control trial.
Risk of bias
The AMSTAR 2 rating of the included systematic review was critically low (The AMSTAR 2 checklist is included as a Supplemental File). Among the four RCTs included, three were assessed as having a low risk of bias, and one had a moderate risk of bias, though the specific assessment tools used were not reported.
Synthesis of results
Due to the heterogeneity in study designs, treatment protocols, outcome definitions, and materials used across the included RCTs, a meta-analysis could not be conducted. Instead, a narrative synthesis was performed. The clinical success rates reported for pulpotomy ranged from 81.2% to 98.19%, with CEM and MTA demonstrating the highest success rates across trials. In contrast, CH and PRF exhibited comparatively lower and more variable outcomes. Radiographic success rates showed wider variation, ranging from 38.4% to 95%, again favoring CEM and MTA. The studies differed not only in the biomaterials used but also in their follow-up durations (1–2 years) and outcome assessment criteria, which further limited direct comparisons. Despite these differences, the included RCTs consistently indicated that pulpotomy can achieve favorable results in mature permanent teeth with irreversible pulpitis. However, the variability in methodologies and the absence of long-term data across all trials call for cautious interpretation and underscore the need for standardized protocols in future studies.
Reporting bias and certainty of evidence
These aspects were not addressed in the included systematic review.
Discussion
This overview highlights the emerging role of pulpotomy as a biologically conservative treatment modality for mature permanent teeth diagnosed with irreversible pulpitis. While only one systematic review met the inclusion criteria, the findings from the four RCTs it synthesized consistently point toward high clinical success rates for pulpotomy when biocompatible materials such as CEM and MTA are used. Importantly, these success rates approached or even equaled those of conventional root canal treatment (RCT), traditionally considered the gold standard. A key finding is that material selection substantially influenced both clinical and radiographic outcomes, with CEM demonstrating not only excellent clinical performance but also favorable radiographic healing, suggesting it may offer superior biological compatibility or sealing ability. While MTA also performed well, variability in radiographic success across studies raises questions about handling, placement, or case selection. In contrast, CH and PRF, though historically explored, showed lower and more inconsistent outcomes.
Despite the promising results, the review's methodological limitations included lack of bias assessment, poor reporting, and the absence of certainty grading which mean that these findings should be interpreted with caution. Utilizing CEM cement for pulpotomy presents a noteworthy option compared to conventional root canal procedures for managing irreversible pulpitis. This method provides a gentler and more economical approach. This is particularly beneficial in regions with limited access to advanced dental equipment, where resources like radiography units, essential for RCT, may be unavailable. In such areas, patients often face a choice between extraction and living with untreated dental pain. Additionally, in countries where RCT is not covered by public health insurance, financial barriers can make pulpotomy an attractive option, as it preserves the tooth's functionality while being more affordable. 21
One significant biological advantage of pulpotomy is its ability to maintain the vascularization and nutritional supply of the dental pulp. This is crucial for the long-term health of the tooth, especially in younger patients, where preserving pulp vitality reduces procedural complexity and improves patient compliance by minimizing discomfort and appointment time. 22 However, the application of pulpotomy as a definitive treatment for irreversible pulpitis in mature teeth remains controversial. Traditionally, irreversible pulpitis has been treated with RCT or extraction, and pulpotomy has been seen as a deviation from conventional protocols. 23
The diagnosis and management of irreversible pulpitis are complicated by the variability in clinical symptoms, which do not always accurately reflect the extent of pulpal pathology. Common indicators like prolonged spontaneous pain and sensitivity to percussion are often poor predictors of the true state of pulp health. Studies have shown that the degree of inflammation at the exposure site may not correspond with the extent of tissue damage, leading to potential misjudgments in treatment planning. 24 For instance, Giuroiu et al. found that clinical symptoms often fail to accurately predict the histopathological condition of the pulp. 25
To improve diagnostic accuracy, recent research suggests using the time required to achieve hemostasis during pulpotomy as a more reliable indicator of pulp inflammation severity. 26 Hemostasis achieved within 1 to 10 min is often associated with inflammation confined to the coronal pulp, making pulpotomy a more suitable treatment option. 27 This approach provides a more objective measure compared to subjective clinical symptoms, offering greater precision in determining when pulpotomy is appropriate for irreversible pulpitis.
The traditional belief that irreversible pulpitis always requires RCT or extraction has been challenged by advances in pulp biology and therapy. Biologically based treatments that aim to preserve pulp vitality and function are now seen as potentially superior in certain cases. This trend toward minimally invasive, regenerative approaches reflects a broader shift in endodontics toward preserving natural tooth structures and utilizing the body's inherent healing capabilities rather than resorting to pulp removal.28,29 The success of pulpotomy in treating irreversible pulpitis, particularly in resource-limited settings, could have significant implications for patient care and dental treatment economics. 24
Although traditionally applied to primary and developing permanent teeth, the use of pulpotomy in fully mature teeth demands thorough evaluation. The evolving treatment guidelines reflect a shift toward more conservative management of irreversible pulpitis, but the current evidence is insufficient to fully endorse pulpotomy as a standard treatment for this condition. Strengthening the evidence base will be essential to improving clinical practice and patient outcomes in the management of irreversible pulpitis.
Interpretation in context
Recent endodontic literature and position statements from professional bodies, such as the American Association of Endodontists and the European Society of Endodontology, support a shift toward minimally invasive vital pulp therapies, including full pulpotomy, even in mature permanent teeth.4,5 Histological studies have shown that clinical symptoms do not always reflect irreversible pulpal damage, providing a rationale for preserving pulp vitality in select cases. 30 However, the strength of this overview's conclusions is limited by the methodological quality of the included SR and the lack of meta-analytical synthesis. The included RCTs were heterogeneous in terms of materials used, diagnostic criteria, outcome definitions, and follow-up durations, which challenges direct comparison and generalizability.
Limitations
This overview is subject to several limitations:
Only one systematic review met the inclusion criteria, limiting the comprehensiveness of the evidence base. The included SR was rated as critically low quality, affecting the reliability of its findings. The follow-up duration in the included trials was relatively short (1–2 years), which may not reflect long-term outcomes The SR did not report on risk of reporting bias or certainty of evidence, which are crucial for interpreting clinical validity.
Implications for practice and research
Despite limited high-quality evidence, pulpotomy appears to offer a promising alternative to RCT in mature permanent teeth, particularly in settings where cost, time, or access to specialist care is a constraint. Its use could reduce treatment burden while preserving tooth vitality, especially when materials like CEM and MTA are used. However, clinicians must exercise caution and rely on strict case selection until more robust evidence becomes available. Therefore, we emphasize the need for well-designed, long-term RCTs that incorporate standardized diagnostic criteria, clearly defined outcome measures, and consistent treatment protocols. Additionally, high-quality systematic reviews are essential—those that follow transparent methodology, include rigorous risk of bias assessment, and apply formal certainty grading frameworks such as GRADE. These steps are critical to strengthening the current evidence base for pulpotomy in mature permanent teeth and to facilitating the development of reliable, evidence-based clinical guidelines.
Conclusion
This overview of systematic reviews highlights that pulpotomy, particularly with materials like CEM and MTA, may serve as a viable and cost-effective alternative to root canal treatment in mature permanent teeth with irreversible pulpitis. While clinical success rates are promising, the quality of existing systematic reviews is limited. Therefore, pulpotomy should currently be considered only in carefully selected cases. Future research should focus on conducting well-designed RCTs and higher-quality systematic reviews to provide more definitive evidence for clinical guidelines.
Supplemental Material
sj-pdf-2-sci-10.1177_00368504251346677 - Supplemental material for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials
Supplemental material, sj-pdf-2-sci-10.1177_00368504251346677 for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials by Ajay Chhabra, B Saravana Prathap, Ramya KP, Priyanka Yadav, Himani, Sona J Parvathy and Vandana Chhabra in Science Progress
Supplemental Material
sj-pdf-3-sci-10.1177_00368504251346677 - Supplemental material for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials
Supplemental material, sj-pdf-3-sci-10.1177_00368504251346677 for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials by Ajay Chhabra, B Saravana Prathap, Ramya KP, Priyanka Yadav, Himani, Sona J Parvathy and Vandana Chhabra in Science Progress
Supplemental Material
sj-xls-4-sci-10.1177_00368504251346677 - Supplemental material for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials
Supplemental material, sj-xls-4-sci-10.1177_00368504251346677 for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials by Ajay Chhabra, B Saravana Prathap, Ramya KP, Priyanka Yadav, Himani, Sona J Parvathy and Vandana Chhabra in Science Progress
Supplemental Material
sj-csv-5-sci-10.1177_00368504251346677 - Supplemental material for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials
Supplemental material, sj-csv-5-sci-10.1177_00368504251346677 for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials by Ajay Chhabra, B Saravana Prathap, Ramya KP, Priyanka Yadav, Himani, Sona J Parvathy and Vandana Chhabra in Science Progress
Supplemental Material
sj-xlsx-6-sci-10.1177_00368504251346677 - Supplemental material for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials
Supplemental material, sj-xlsx-6-sci-10.1177_00368504251346677 for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials by Ajay Chhabra, B Saravana Prathap, Ramya KP, Priyanka Yadav, Himani, Sona J Parvathy and Vandana Chhabra in Science Progress
Supplemental Material
sj-xlsx-7-sci-10.1177_00368504251346677 - Supplemental material for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials
Supplemental material, sj-xlsx-7-sci-10.1177_00368504251346677 for Pulpotomy for irreversible pulpitis in mature permanent teeth: An overview of systematic reviews of randomized controlled trials by Ajay Chhabra, B Saravana Prathap, Ramya KP, Priyanka Yadav, Himani, Sona J Parvathy and Vandana Chhabra in Science Progress
Footnotes
Acknowledgements
The authors used Grammarly (Grammarly Inc.) to assist in grammar correction and language refinement during manuscript preparation.
Author contributions
Saravana Prathap B.: conceptualization, methodology, investigation, data curation, writing—original draft, writing—review and editing, supervision, and project administration; Ramya K.P.: conceptualization, methodology, formal analysis, investigation, data curation, and writing—original draft; Ajay Chhabra: supervision, formal analysis, validation, and project administration; Priyanka Yadav: investigation, supervision, formal analysis, and resources; Sona J Parvathy: methodology, formal analysis, visualization, and resources; Himani: formal analysis, resources, validation, and visualization; Vandana chhabra: formal analysis, validation, visualization, and resources.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All extracted data and forms used during the overview are available upon request from the corresponding author.
Registration and protocol
This overview was not registered; no protocol prepared.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.