
Abstract
Due to the COVID-19 pandemic, the pressure on healthcare systems has been tremendous and it is having a huge economic impact. The objective of this paper is to carry out a systematic literature review of the publications that have analysed the costs derived from COVID-19 from the patient's perspective. Not only is this study aimed at measuring the impact of COVID-19 in economic terms, but also in qualitative terms, analysing, for instance, the types of costs (direct and indirect) and their variations depending on the geographical area under study. Searches were conducted in PubMed, Cochrane Library, Web of Science and Scopus. The time frame for the analysis was from the start of the pandemic until 9th December 2021. A total of 322 papers were found. The number of articles assessed for eligibility was 32, and after applying the exclusion criteria, 13 papers were included in the qualitative synthesis. Most of the studies analysed only direct costs (69.23%) and were focused on Asia (61.54%), where the larger indirect costs, as well as the greater total costs, were found. However, the higher costs per patient and year were shown for the United States. This investigation showed the importance of COVID-19 in national, regional and local budgets. More studies are to be developed in Europe due to both the existing differences in the health care systems and financing by country and the difference in the incidence of COVID-19 by country and wave.
Introduction
Current coronavirus disease, commonly known as COVID-19 (from SARS-CoV-2 pathogen) was initially identified in Wuhan (China) in December 2019.1,2 For the first weeks after its emergence, the virus spread fast and uncontrollably all over the world which led the World Health Organization (WHO) to declare an influenza global pandemic in March 2020. 3 From that moment on, national and regional Governments put in place different mechanisms in order to break the chain of virus transmission, including social distancing measures and general lockdowns,4,5 especially during the first months of the pandemic period.
According to WHO Coronavirus Dashboard, 6 nearly 400 million people in the world had been infected with COVID-19 by February 2022, and more than 5.7 million people have lost their lives; horrifying figures reminiscent of the human immunodeficiency virus (HIV) that remains one of the main global public health issues. Indeed, as stated by the latest WHO ‘Key facts of HIV and AIDS’ 7 in 2022, around 630,000 people died from HIV-related causes being nearly 1.3 million people who acquired HIV. It is, therefore, undoubtful that the impact on individual's health has been dramatic.
The COVID-19 pandemic has severely hit every healthcare organization as they are facing the most serious global pandemic crisis in a century. Healthcare systems have been stretched to the limit. 8 Not only have they focused on containing the spread of the virus, but they have also tried to provide an effective care service to any patient, COVID or non-COVID. As a result, the pressure on healthcare systems has been tremendous and different measures were activated in order to reduce it. 9 For instance, some institutions decided to cancel some elective surgical procedures and clinics, which has led to substantial strain on hospitals.1,10,11
The dramatic consequences of COVID-19 have not been limited solely to the clinical field, but have quickly spread to the social and economic spheres. 12 In fact, it might be said that the SARS-CoV-2 pandemic has had a huge economic impact on society. This is related to a larger economic burden, both due to direct (hospitalization, medical tests and/or drugs, among others) and indirect costs (sick leaves and the losses in productivity due to lockdown).
Almost two years after the pandemic started, different reports have tried to estimate the economic impact of COVID-19 from a macro perspective13–15; however, very few studies have analysed direct and indirect costs derived from this disease. 16
The aim of this study is to carry out a systematic literature review of the costs related to the coronavirus disease 2019 (COVID-19) pandemic. Specifically, the following research questions are stated:
What is the average cost generated as a consequence of COVID-19? What type of costs are included in the studies (direct, indirect or both)? Which regions (geographically speaking) are the studies based in? Are there differences between regions in terms of costs? If so, what kind of differences?
Materials and methodology
Study design and search strategy
From a methodological point of view, this paper is based on a systematic literature review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 17 The main aim is to analyse the literature that has been published about COVID costs. In this sense, we define direct costs as those which include inpatient care, outpatient care, drugs, diagnostics, nursing care, social services, and patients’ travel costs in order to get to health care. Meanwhile, indirect costs are losses of production due to short- or long-term sickness absence, disability pension, early old-age pension due to health problems, and permanent losses due to premature death. Thus, total costs represent the aggregate of direct and indirect costs. 18
All empirical studies where COVID-19 outcomes could be related to their economic burden or cost were included. One reviewer (LSR) removed irrelevant articles and assessed eligibility using the following criteria:
- Document type: Scientific journal article (full text). - Publication language: English. - Topic: COVID costs.
Web of Science, Scopus, PubMed and Cochrane were searched to carry out the systematic literature review. In order to delimit the topic, a combination of four Medical Subject Headings (MeSH) terms and keywords was applied: (‘economic burden’ or ‘cost analysis’) and ‘COVID’ and ‘patient’ (Table 1).
Search strategy.

Source: Authors’ elaboration.
Sample and data
Initially, 322 documents were identified (152 Web of Science; 124 Scopus; 6 Cochrane; 40 PubMed). LSR screened the titles and abstracts of all the papers and excluded those that did not meet the inclusion criteria. Maintaining a conservative position, if LSR was doubtful about any of the papers, it was classified as undecided, and the full text was analysed by CBF and PLL. Based on this, 271 were excluded. As a result, 51 articles were selected and 2 more were added by the authors (hand searching).
Afterward, duplicates were removed (19). The full text of the remaining 32 articles was screened by LSR, CBF and PLL. After full-text readings, 19 papers were excluded: 13 of them were out of scope, 4 were not applied and the full text of two of them was not available. That is, to minimize the bias problems, we employed adequate and rigorous search methods, examining mainly both a large search and data extraction by independent reviewers.
Data analysis procedure
Content analysis was done in the remaining 13 papers. Given the objective of the systematic review (to analyse the literature that has been published about COVID costs), the comparative analysis has been done using Purchasing Power Parities (PPP) and estimating costs in euros (€) of 2020. In doing so, we were able to compare direct cost, indirect cost and total costs between the different articles considered, which analyse various countries. Table 2 includes the coding. The authors developed and agreed on the coding in order to collect the information from all the studies.
Coding.

Source: Authors’ elaboration.
For the coding process, each author will independently code a set of articles. After that independent analysis, a common work session was held to put all the information together and draw the final conclusions of the study.
Results
This section describes the most relevant findings of the articles selected in our literature review. As we have previously mentioned, in this article we analyse the literature that studies costs related to COVID-19 infection with special attention to classify it according to types of costs. Overall, 13 studies were included in the study. The whole process is described in Figure 1.

Flow diagram of paper selection process. Source: Authors’ elaboration.
The costs finally included in this review are direct costs (direct health care costs and direct non-medical costs), indirect costs, and totals. Therefore, Table 3 summarizes the 13 articles found in the database search and hand-searching methods, including information about the country, objective, type of costs and main results.
Mapping of relevant studies considered (N = 13).

Source: Authors’ elaboration.
Then, we have compared the articles that only focus their analysis on direct costs versus those that consider other types of costs. It should be noted that around 70% of the sample (exactly, 69.23% of them) only focused on direct costs. Besides, regarding country information, it is obtained for America (United States), Asia (Saudi Arabi, Korea, China, Iran, and India) and Europe (Spain, Greece, and Germany) being their corresponding references for each area the following: America (Di Fusco et al.; 19 Tsai et al. 20 ), Asia (Khan et al.; 21 Lee et al.; 22 Li et al.; 23 Reddy et al.; 24 Ebrahimipour et al.; 25 Darab et al.; 26 Jin et al.; 27 Nakhaei et al. 28 ), and Europe (Romeyke and Stummer 16 ; Carrera-Hueso et al.; 29 Maltezou et al. 30 ).
In this context and focusing on Europe, Romeyke and Stummer 16 examine costs for the care of COVID-19 patients according to the G-DRG system. Carrera-Hueso et al. 29 evaluate the direct impact of the COVID-19 pandemic on Spain's health budget. According to America, Di Fusco et al. 19 determine health outcomes and the economic burden of hospitalized COVID-19 patients. Tsai et al. 20 analyse the characteristics of older adults with COVID-19 and their costs related to medical care. In the case of articles that examine Asia, Khan et al. 21 determine the survival of hospitalized COVID-19 patients. Lee et al. 22 assess the medical costs among children with COVID-19. Meanwhile, Li et al. 23 carry out a cost and affordability analysis to determine the medical costs of COVID-19 patients. Reddy et al. 24 conducted a cost analysis of COVID-19 patients requiring ICU admission. Similarly, Ebrahimipour et al. 25 evaluate both diagnostic and therapeutic costs of hospitalized patients with a diagnosis or suspected of COVID-19 disease.
However, the remaining four articles considered other types of costs (excluding only direct costs). Darab et al. 26 determine both direct medical and indirect costs of treating COVID-19 and the economic burden of the disease. Jin et al. 27 evaluate the health and societal costs of COVID-19. Similarly, Maltezou et al. 30 assess the costs associated with SARS-CoV-2 exposure and infection among healthcare professionals. Finally, Nakhaei et al. 28 estimate costs of COVID-19 patients.
Besides, Table 4 completes this information including the year of data, currency and the figures regarding each type of cost.
Summary of each of the 13 studies included in the analysis of comparing costs.

Source: Authors’ elaboration.
It should be noted that most of the articles are based, as expected, on the year 2020. In addition, it is found that the median cost per patient differs between studies. That is, there appear differences both by area and aim of the analysis.
All in all, to shed light on the above-mentioned results, in what follows, we provide homogeneous comparisons of our 13 eligible papers through the following three figures. Precisely, Figure 2 represents the information by geographic area, whereas Figure 3 shows the cost differences in these areas.
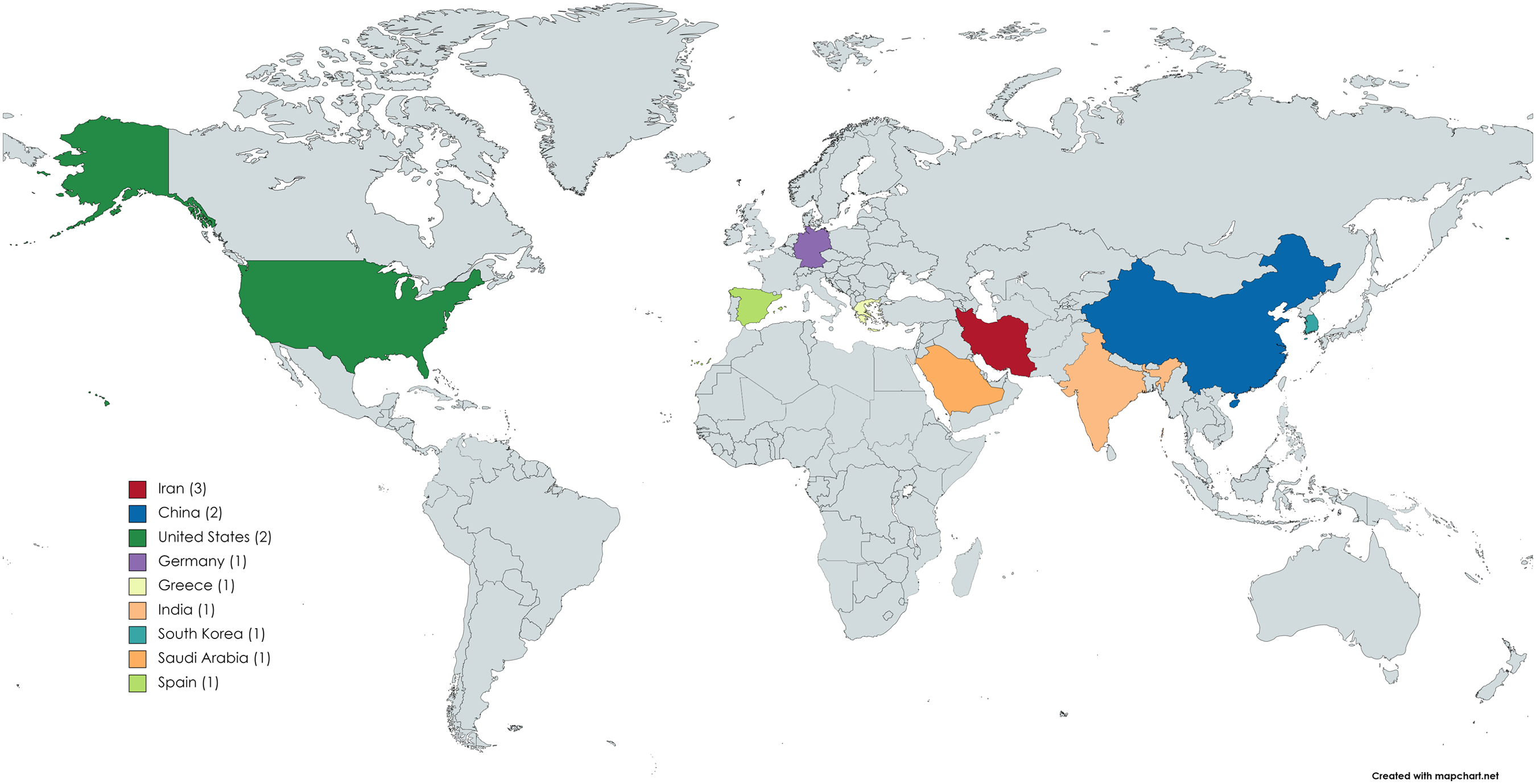
Distribution of the articles considered according to the area. Source: Authors’ elaboration.

Average cost (€ 2020) per patient per type of cost according to the area. Source: Authors’ elaboration. Note 1-Studies by area: America (Di Fusco et al.; 19 Tsai et al. 20 ), Asia (Khan et al.; 21 Lee et al.; 22 Li et al.; 23 Reddy et al.; 24 Ebrahimipour et al.; 25 Darab et al.; 26 Jin et al.; 27 Nakhaei et al. 28 ), and Europe (Romeyke and Stummer 16 ; Carrera-Hueso et al.; 29 Maltezou et al. 30 ). Note 2-Countries by area: America (United States), Asia (Saudi Arabi, Korea, China, Iran, and India), and Europe (Spain, Greece, and Germany).
Hence, it has been analysed the countries studied in the selected articles. To simplify, in Figure 2, we have clustered them by country. A great part of the research is located in Asia (8 articles, which represent 61.54% of the total sample and include countries such as China, India, Iran, Korea and Saudi Arabi), followed by Europe (3 articles representing 23.08%, which analyse three countries such as Germany, Greece and Spain), and America (North America, n = 2, focusing only on the United States). The remaining continents entail 0%.
Secondly, Figure 3 shows the notable differences in average cost per patient and geographic area (in € 2020). The direct costs for the United States stand out and get € 18,872.85. Those direct costs are around 4,500–5,000 euros for Asia and Europe (€ 4,427.95 and € 4,824.31; respectively). Furthermore, regarding indirect costs there also appear important differences: € 7,478.86 for the Asian studies versus € 2,188.58 if we considered the European ones. Overall and broadly speaking, Europe seems not to be the most damaged region (at least at this time, with the published scientific evidence, which may differ from the accounting one of the different health care systems).
Summing up, most of the studies considered here (nine articles) only focus on the analysis of direct costs and take into consideration economic costs related to hospitalization, RT-PCR for SARS-CoV-2, ICU stay, or chest radiograph, among others. Only four articles examine other types of costs or several types of costs at the same time, such as indirect costs, including those associated with the cost of missed workdays (patients as well as families’ patients) and even the cost of premature death. On one hand, more than 60% of the selected articles focus their analysis on Asia, followed by Europe and America. On the other hand, we find the larger direct costs in the United States whereas the greater indirect and total costs are shown for Asia.
This research points out the great importance of COVID-19 in national, regional and local budgets. The authors of this systematic review consider that these differences may be due to differences in the healthcare systems and financing of the different countries, due to the incidence of COVID-19, or due to a combination of both. Therefore, further studies are needed.
Discussion
This study provides insight into the costs related to COVID-19 infection. Most of the studies (69.23%) analyses only direct costs. The selected articles show that the more usual location for conducting the studies is Asia (61.54%), where we find the larger indirect costs as well as the greater total costs (€ 7,474.86 and € 10,505.41, respectively). Trends are observed in several studies of direct and healthcare costs measured by patient and year, where the higher costs were shown for the United States (€ 18,872.85).
To the best of the authors’ knowledge, at the time of the search, there are no other similar studies in this area. But we can see where the costs are in other reviews carried out for other diseases such as dementia 18 or multiple sclerosis. 31 Regarding dementia, it was found that the annual cost per patient with dementia in Europe was on average € 32,506.73, whereas for the United States, it was € 42,898.65. Besides, for multiple sclerosis, it was claimed that the total annual cost per patient in Europe was on average € 40,300. In both, the relevance of not only considering direct health care cost was highlighted.
That is, more information is needed to assess the impact of diseases on the sustainability of healthcare systems. This information is important in order to obtain an improvement in the management of health organizations. Precisely, to have individualized information on the costs per patient is fundamental. It would be very relevant to analyse the impact of COVID-19 vaccination according to the decrease of costs. What it is known is that the maximum level of COVID-19 vaccination without social impositions is about 70% between countries but could be increased. 32 That is, knowing the characteristics of patients, their consumption of resources and their health outcomes will allow predictions to be made about the economic impact of treating diseases, which will facilitate decision-making in health planning and/or in dealing with new waves of this pandemic (and future one).
Limitations of this study
First, we acknowledge that systematic reviews are subject to bias. Moreover, we have considered 4 of the main search engines internationally recognized by academics (PubMed, Cochrane Library, Web of Science and Scopus). Second, we have established several inclusion and exclusion criteria. Third, in spite of considering the full period between the beginning of the pandemic and the end of the literature search, here the period under analysis is only 2 years. That is, the results could be amplified in the near future when more articles would be available.
Conclusions
These days, there is a growing concern about the economic impact that COVID-19 is having on the economy in general, and in the health sector in particular. Focusing on the latest, the seriousness of the COVID-19 pandemic has highlighted the need for information regarding incidence, mortality, resource consumption and/or healthcare pressure. The objective of this review was to know the cost per patient with COVID-19.
The results obtained reinforce the initial idea that COVID-19 has had a strong economic impact on healthcare systems, both directly and indirectly. In turn, this fact reinforces the need to develop new cost-based studies so that decision-makers can make the most appropriate decisions about allocating resources and managing healthcare tight budgets. In addition, the results show great disparities between the different geographical areas. Therefore, it seems interesting to develop new studies analysing how COVID-19 costs are related, if they are, with the national and/or regional social measures established to control the spread of the virus 33 ; together with the preparedness of the countries to face similar crisis. 34 Conclusions in this sense will be very useful when designing new social and healthcare policies.
Footnotes
Abbreviations
Author contributions
All authors were involved in all stages of the systematic literature research and review of studies. All authors contributed to the writing of the manuscript and read and approved the final manuscript.
Availability of data and materials
The data are available on reasonable request from the corresponding author.
Consent for publication
All authors have approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received financial support from the Valdecilla Biomedical Research Institute (IDIVAL) through the project ‘Test de estrés o resistencia en el Sistema Cántabro de Salud, desarrollo de tecnologías innovadoras digitales para modelizar escenarios de mayor utilización sanitaria y soluciones de impacto socioeconómico y humano frente a la COVID-19’ with reference INNVAL20/03.
Registration protocol
The review was not registered because this review focus the analysis only on costs.
Author biographies
Carla Blázquez-Fernández, PhD in Economics (2015). She is Lecturer in the Department of Economics at Universidad de Cantabria (Spain). Her main lines of research are Public Economics and Health Economics, about which she has published many papers in national and international specialized journals. She belongs to the two Health Economics research groups that exist in Cantabria, University of Cantabria and IDIVAL. She has carried out short-stays at the City University of London (UK) and the Universidade de Coimbra (Portugal). She has been involved in several multidisciplinary teams for the development of different competitive research projects (including those funded by the European Commission through the Horizon 2020 Framework, etc.). She has acted as reviewer for several high-impact journals and has presented many works as oral presentation in international and national conferences and seminars. Moreover, she has been part of several organizing committees of conferences and meetings related to Applied Economics, Public Economics and Health Economics.
Paloma Lanza-León is PHD in Economics from the Universities of Cantabria, Oviedo and the Basque Country (Spain). She is a researcher at the Health Economics Research Group of the University of Cantabria and the Valdecilla Biomedical Research Institute (IDIVAL). Currently, she is hired as a postdoctoral researcher in the Department of Economics of the University of Cantabria, where she has developed her research career since it began in 2018. She was a visiting pre-doctoral student at City University of London (United Kingdom) in 2019 and a pos-doctoral one at University of Amsterdam (Netherlands). She has published several peer-reviewed articles, which have been published in different journal such as The European Journal of Health Economics, Health Policy or The International Journal of Health Planning and Management; and she has a H-index of 5 (Google Scholar). She is also a reviewer in indexed journals. Her main fields of research are focused on Public Economics, Health Economics and Public Policy Evaluation. Additionally to her research, she has taught in the Degree of Business Administration, the Degree of Economics and in the Master on Management of Healthcare Services of the University of Cantabria.
Lidia Sanchez-Ruiz is Associate Professor at the University of Cantabria. Her teaching is focused on the field of production and operations management, logistics and process management. Her main lines of research are focused on process management and continuous improvement, with a specific research line focused on sustainability (triple impact, B Corp. certification). She is the co-author of more than fifty scientific articles published in prestigious national and international publications. She has taken part in more than twenty projects. She is a researcher of the Santander Financial Institute (SANFI); member of the Yunus Center at the University of Cantabria and GEM (Global Entrepreneurship Monitor) senior researcher. Throughout her career, she has held several research stays (University of La Laguna- Spain, Polytechnic University of Catalonia – Spain, Cardiff University – Wales, Universidade do Algarve – Portugal, Universidad Politécnica de Valencia – Spain) and teaching stays (ISM University of Management and Economics, Lithuania; University of Katowice, Poland; Technical University of Sofia, Bulgary).
David Cantarero-Prieto is Full professor (Catedrático de Universidad). H index 26. Director of Master and Research (www.madgs.es) University&Health Departament Cantabria. Group of Health and Public Economics. IDIVAL Valdecilla Hospital. Associate editor Gaceta Sanitaria (![]() he is involved in EU Project TIMELY till September 2024 and Cost and Joint actions HEALTH4EUkids 2026. In addition to his teaching and research on Public Economics at the Faculty of Economics in the University of Cantabria, he also works doing consultancy, training and research projects on Public Policies Evaluation, mainly in: Tools for Impact Evaluation in practice.Monitoring and Evaluation of public programs and policies. Economic Analysis (Statistics and Econometrics) in Social Research. Fiscal Federalism and Taxation. Health Economics and Social Expenditure. Ageing and Silver Economy. He have developed this work in different countries including Spain, Belgium, Denmark, France, Germany, Ireland, Italy, Netherlands, Poland, Portugal, Sweden and England.
he is involved in EU Project TIMELY till September 2024 and Cost and Joint actions HEALTH4EUkids 2026. In addition to his teaching and research on Public Economics at the Faculty of Economics in the University of Cantabria, he also works doing consultancy, training and research projects on Public Policies Evaluation, mainly in: Tools for Impact Evaluation in practice.Monitoring and Evaluation of public programs and policies. Economic Analysis (Statistics and Econometrics) in Social Research. Fiscal Federalism and Taxation. Health Economics and Social Expenditure. Ageing and Silver Economy. He have developed this work in different countries including Spain, Belgium, Denmark, France, Germany, Ireland, Italy, Netherlands, Poland, Portugal, Sweden and England.