
Abstract
Background
Portal hypertension (PH) is a clinically significant entity that could present with life-threatening gastrointestinal bleeding. Cirrhosis is the most common cause of PH, with well-documented histopathology and etiology. However, in idiopathic portal hypertension (IPH), no single histopathologic finding is associated with PH. Our systematic review aims to identify and summarize the prevalence of the common histological findings of IPH.
Methods
We systematically searched PubMed, Cochrane CENTRAL, Web of Science, and Scopus till 1ST March 2022 for studies describing the histopathological features of IPH. Data were extracted from eligible studies and pooled as events rate and 95% confidence interval (CI) using binary random-effects model by open meta-analyst software.
Results
We included 23 retrospective studies with a total sample size of 813 patients. The overall incidence of nodular regenerative hyperplasia was 38.6%, 59.8% for portal fibrosis, 51.3% for periportal fibrosis, 39.3% for perisinusoidal fibrosis, 89.8% for portal vein sclerosis, 42.2% for portal inflammation, 53.3% for mega-sinusoids, 39.5% for thickening of portal vein branches, 93.8% for narrowing of portal veins, 53.3% for hepatic veins/venous outflow obstruction, 51.4% for aberrant portal/periportal vessels, 42.4% for shunt vessel, 50.9% for ductular proliferation, and 16.3% for steatosis.
Conclusion
Due to the relatively non-pathognomonic and non-specific nature of IPH, a combination of different histological features such as the portal and periportal fibrosis, portal vein sclerosis, mega-sinusoids, narrowing of portal veins, hepatic venous outflow obstruction, aberrant portal or periportal vessels, and ductular proliferation may be of value in diagnosing IPH as the incidence rate of these features was at approximately 50%.
Introduction
Idiopathic non-cirrhotic portal hypertension (INCPH) is a clinical disorder of uncertain etiology. It is intrahepatic portal hypertension (PH) in the absence of cirrhosis. 1 In 1965, Mikkelsen et al. introduced the term hepatoportal sclerosis (HPS) after identifying concentric sclerosis in the portal vein of patients with noncirrhotic PH. 2 Historically, other terms have been used to describe the histopathological changes in INCPH, including noncirrhotic portal fibrosis, 3 obliterative portal venopathy (OPV), 4 Porto-sinusoidal vascular disease, 5 and nodular regenerative hyperplasia (NRH). 6
Although the etiology of this condition is still unknown, several pathophysiological causes were mentioned in the literature, involving recurrent infections, hypercoagulability states, altered immune response, and genetic liability.1,7
INCPH has also been reported progressively in patients with HIV infection who can present with typical PH complications, such as variceal bleeding and ascites. In this case, the most common proposed mechanism playing an etiological role in its INCPH pathogenesis is sustained exposure to antiretroviral treatment, especially didanosine (ddI).8–11
The most common clinically significant presentation of idiopathic portal hypertension (IPH) is upper gastrointestinal bleeding due to esophageal varices. Hepatic venous pressure gradient (HVPG) is the predominantly used parameter to indicate the risk of bleeding from esophageal varices. It represents the pressure difference between the portal vein and the intra-abdominal portion of the inferior vena cava. 12 Other common conditions associated with IPH include thrombocytopenia and splenomegaly, usually with an intact liver synthetic function.13,14
A liver biopsy is usually performed to exclude cirrhosis and other causes of PH in patients with IPH.3,15 The interpretation of liver biopsy in IPH patients remains controversial because of the reported heterogeneity in histological features. 16
Histopathology of IPH has a broad spectrum ranging from insignificant non-definite changes, OPV, portal fibrosis, dilated sinusoids, HPS, NRH to a mixture of the last two histopathological features.17,18 However, no consensus diagnostic histological criteria for IPH have been demonstrated. Distortion of the portal vein branches (including obliteration, different degrees of sclerosis, increase in the number of branches, dilation, and luminal narrowing)19–21 was reported as the most common associated features in many studies, but the relative frequency of the histopathological changes in IPH differs among studies.15,19
In addition to diversity among studies for identifying the applicable histologic diagnostic criteria in patients with INCPH, no systematic reviews and meta-analyses were performed to identify the particular criteria. Hence, we performed the first systematic review and meta-analysis that assembled all available studies to recognize which histologic feature(s) are the fundamental predictor(s) for this condition and establish the histological diagnostic criteria.
Methods
Search strategy and data collection
We searched four electronic databases: PubMed, Cochrane CENTRAL, Web of Science, and Scopus for all published articles till the 1st of March 2022, using the following search strategy: (NCPF OR INCPH OR non-cirrhotic OR non-cirrhotic OR noncirrhotic) AND “Hypertension, Portal” [Mesh]). We also used the trials registry of the US National Institutes of Health (http://www.clinicaltrials.gov) to identify any other studies with the published results.
The duplicates were removed using Endnote software. All retrieved records were assessed for eligibility through titles and abstracts screening, then full-text screening. Those that matched our criteria were included in our study. For other related studies, we manually screened the references of the included studies.
Selection criteria
We included all studies that met the following criteria with no restrictions on age, sex, site, or publication date:
Inclusion criteria
Retrospective studies describing the histopathological features of idiopathic non-cirrhotic PH diagnosed according to the following criteria:
Evidence of portal hypertension as esophageal varices, hypersplenism, ascites, or increased hepatic venous pressure gradient. Doppler ultrasound showing patent portal and hepatic veins at the time of diagnosis.
Exclusion criteria
Hepatic cirrhosis on histology.
Conditions that cause cirrhosis according to conventional diagnostic criteria as chronic viral hepatitis, alcoholic liver disease, non-alcoholic steatohepatitis (NASH), obesity, hemochromatosis, autoimmune hepatitis, or Wilson's disease.
Conditions lead to portal hypertension: schistosomiasis, hepatic arterioportal fistula (HAPF), and veno-occlusive disease of the liver.
Chronic vitamin A intake, professional exposure to copper sulfate, vinyl chloride monomer, past angiography with thorium sulfate, exposure to Spanish toxic oil, or arsenic salts.
Malignancies.
Non-English studies, thesis, reviews, and if the abstract only is available.
Data extraction
Two independent reviewers with expertise in the field of IPH, initially extracted data from the included studies. Each reviewer used a standardized data extraction form to collect relevant information from the studies. In addition, a third reviewer, also an expert in IPH, verified the data extracted by the two initial reviewers. This reviewer compared the extracted data from both reviewers and identified any discrepancies or inconsistencies. Any discrepancies were settled by discussion.
The data extraction form primarily included: (a) a summary of the included studies such as country/site involved, inclusion criteria, exclusion criteria, specimen collection, type of stain, indications for liver biopsy, initial clinical diagnosis, co-morbidities, concomitant medications, and duration of symptom at presentation. (b) Baseline characteristics of the enrolled population, including the number of patients, number of provided specimens, males, age, body mass index (BMI), race, splenomegaly, hepatomegaly, spleen size (cm), liver size (cm), esophageal varices, esophageal varices grade (I:II:III: IV), gastrointestinal bleeding episode, portal hypertensive gastropathy, ascites, jaundice, encephalopathy, liver stiffness (kPa), Child-Pugh class (A:B: C), total proteins (g/dL), serum albumin (g/dL), total bilirubin (mg/dL), alanine aminotransferase (ALT) (IU/L), aspartate transaminase (AST) (IU/L), alkaline phosphatase (AP) (IU/L), Gamma-glutamyl transferase (GGT) (IU/L), protein C deficiency, protein S deficiency, WBC count (103/µL), platelet count (103/mm3), prothrombin time (INR/%/sec), RBCs count (106/mm3), hemoglobin (g/dL), and hypersplenism. (c) Histopathological features including NRH, portal fibrosis, periportal fibrosis, perisinusoidal fibrosis, portal vein sclerosis, portal inflammation, mega sinusoids, phlebosclerosis (thickening of portal vein branches), narrowing of portal veins, hepatic veins/venous outflow obstruction, aberrant portal or periportal vessels, shunt vessel, ductular proliferation, and steatosis.
Quality assessment
We assessed the quality of the included studies according to the quality assessment tools of the National Heart, Lung, and Blood Institute (NHLBI). 22 We used the tool of observational cohort studies and the tool of case-control studies. They composed of questions assessing the risk of bias and confounders. Each question was answered by “yes,” “no,” “not applicable,” “not reported,” and “cannot determine,” then each study was given a score to guide the overall quality, either “poor,” “fair,” or “good.”
Statistical analysis
We pooled the histopathological features as events rate and 95% confidence interval (CI) using a binary random-effect model by Open-Meta[Analyst] software. The I-squared test (I2) and the P-value of the Chi-squared test were used to assess inconsistency among pooled studies. 23 According to the Cochrane Handbook, values of I2 > 50% and P < 0.1 were indicators of significant heterogeneity. 24
Results
Literature search results
Our search retrieved 2150 records, only 17 records were duplicates and were excluded. Another 1963 records were excluded by title and abstract screening, and the remaining 170 were eligible for full-text screening. We finally included 23 studies in our review.7,8,13,17,25–43 The flow chart of the data collection and screening process is shown in Figure 1.

PRISMA flow diagram.
Characteristics of the included studies
Most of the included studies were retrospective, with 813 patients and 623 provided specimens. Their mean age ranged from 15.3 to 60.7 years, with different disease durations varying from several months to years. The summary of the included studies and baseline characteristics of their enrolled subjects are shown in Supplemental Table 1.
Quality assessment
According to the NIH quality assessment tool for observational cohort studies, 3 studies7,39,40 were of poor quality, 17 studies7,10,17,26,28–30,32–35,38,41–43,46 were of fair quality, and only 1 study 31 was of good quality (Supplementary Table S1).
As for the NIH quality assessment of case-control studies, the two included case-control studies8,27 were of fair quality (Supplementary Table S2).
Histopathological features
Nodular regenerative hyperplasia
The overall incidence of NRH was 38.6% (95% CI [22.1%, 55.2%]). We found marked inconsistency among the included studies (I2 = 96.55%) (Figure 2).
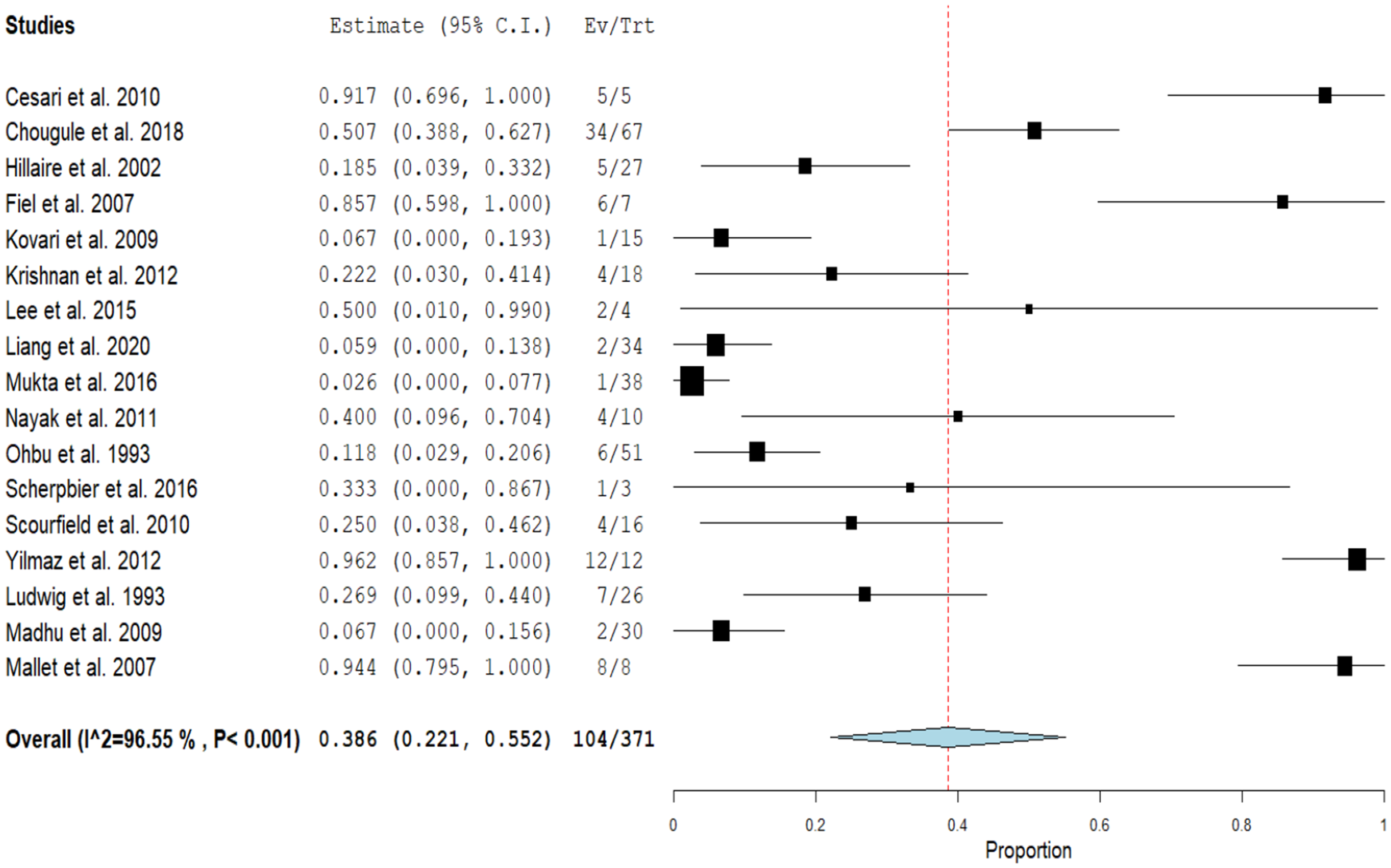
Forest plot of the event rate of NRH.
Portal fibrosis
The overall incidence of portal fibrosis was 59.8% (95% CI [40.8%, 78.9%]), with marked inconsistency among the included studies (I2 = 96.3%) (Figure 3).

Forest plot of the event rate of portal fibrosis.
Periportal fibrosis
The overall incidence of periportal fibrosis was 51.3% (95% CI [28.5%, 74.1%]). We found marked inconsistency among the included studies (I2 = 93.22%) (Figure 4).

Forest plot of the event rate of periportal fibrosis.
Perisinusoidal fibrosis
The overall incidence of perisinusoidal fibrosis was 39.3% (95% CI [23.3%, 52.2%]). We found marked inconsistency among the included studies (I2 = 78.36%) (Figure 5).

Forest plot of the event rate of perisinusoidal fibrosis.
Mega sinusoids
The overall incidence of mega sinusoids was 53.3% (95% CI [27.5%, 79.1%]). We found marked inconsistency among the included studies (I2 = 96.01%) (Figure 6).

Forest plot of the event rate of megasinusoids.
Portal vein sclerosis
The overall incidence of portal vein sclerosis was 89.8% (95% CI [81.5%, 98.2%]), with marked inconsistency among the included studies (I2 = 69.85%) (Supplementary Figure S1).
Portal inflammation
The overall incidence of portal inflammation was 42.2% (95% CI [30.8%, 53.5%]). We found moderate inconsistency among the included studies (I2 = 53.04%) (Supplementary Figure S2).
Phlebosclerosis
The overall incidence of phlebosclerosis was 39.5% (95% CI [9.9%, 69.2%]). We found marked inconsistency among the included studies (I2 = 95.66%) (Supplementary Figure S3).
Narrowing of portal veins
The overall incidence of narrowing of portal veins was 93.8% (95% CI [82.1%, 105.4%]). Pooled results were homogenous (I2 = 0%) (Supplementary Figure S4).
Hepatic venous outflow obstruction
The overall incidence of hepatic venous outflow obstruction was 53.3% (95% CI [32.7%, 73.9%]). We found mild inconsistency among the included studies (I2 = 38.66%) (Supplementary Figure S5).
Aberrant portal or periportal vessels
The overall incidence of aberrant portal or periportal vessels was 51.4% (95% CI [7.2%, 95.6%]). We found marked inconsistency among the included studies (I2 = 98.22%) (Supplementary Figure S6).
Shunt vessel
The overall incidence of shunt vessels was 42.4% (95% CI [14.3%, 70.4%]). We found moderate inconsistency among the included studies (I2 = 67.62%) (Supplementary Figure S7).
Ductular proliferation
The overall incidence of ductular proliferation was 50.9% (95% CI [21.9%, 80%]). We found marked inconsistency among the included studies (I2 = 95.66%) (Supplementary Figure S8).
Steatosis
The overall incidence of steatosis was 16.3% (95% CI [11%, 21.6%]). Pooled results were homogenous (I2 = 0%) (Supplementary Figure S9).
Discussion
Our analysis reports that the incidence rates were higher than 50% for portal vein fibrosis, periportal fibrosis, portal vein sclerosis, mega-sinusoids, narrowing of portal veins, hepatic venous outflow obstruction, aberrant portal or periportal vessels, and ductular proliferation. In contast , the incidence of NRH, perisinusoidal fibrosis, portal inflammation, thickening of portal vein branches, shunt vessel, and steatosis were less than 50%.
The exact etiology/pathophysiology of INCPH is unknown, but it is believed that many factors may play a significant role in disease development. 41 Immunological disturbance, obstructive portal vasculopathy due to thrombophilia, infections, especially HIV, and increased fibrogenesis in portal tracts are considered the main factors.14,41 Immunologically, INCPH patients showed hypergammaglobulinemia and a high titer of antinuclear antibodies (ANA). Also, in the early stages, lymphoid cells were detected in liver biopsies. 14 Previous studies reported that prolonged exposure to highly active antiretroviral therapy (HAART) as didanosine might cause INCPH in HIV patients. 42 However, the exact mechanism of how didanosine causes PH is unknown. 42 The risk of fibrosis is increased when HIV is co-infected with hepatitis B and C. 44
Another theory of INCPH pathogenesis is progressive portal vein fibrosis. An in-vitro study 47 investigated the effect of connective tissue growth factor (CTGF) on liver cell biopsy. CTGF stimulated fibroblast proliferation causing extracellular matrix deposition and fibrosis. High levels of CTGF were found in IPH patients, supporting the theory of PH induced by the portal and peri-portal fibrosis. 47 Thrombophilia and occlusive thromboembolic complications may also be considered primary causes of INCPH.16,28 In Verheij et al., 16 clinicopathological features were described in 40 western IPH patients, and thrombophilia was the most common cause in 16 patients, followed by HIV infection in 8 patients. The partial or complete vessel occlusion leads to an interruption in hepatic hemodynamics and increases the risk of fibrosis. 48 All the previous factors describe the heterogeneous nature of the disease etiology and the difficulty in establishing definitive clinicopathological criteria.
Portal vein sclerosis is the thickening of the portal vein intima or its branches due to the deposition of fibrous tissue. 45 Fibrosis of the portal vein and its small branches, especially with abnormal intrahepatic vessels, is the leading characteristic of the disease. 45 Mukta et al. 33 reported an incidence of 76.3% of portal venous sclerosis among 68 patients diagnosed with the disease. On a larger scale, our pooled data of 813 patients showed a higher incidence rate of portal sclerosis at 89.8% and portal fibrosis at 59.8%. This thickening may lead to the narrowing of vessels and cause PH without cirrhosis. Dhiman et al. demonstrated that the sudden narrowing of veins, especially the major intrahepatic branches, is one of the classic findings of INCPH detected by ultrasonography. 46 A similar finding is reported in our paper; the narrowing of portal veins was at the highest value (93.8%), which increases the vessel resistance and may illustrate how the portal pressure increases.
PH participates in the formation of abnormally dilated channels in the area surrounding the portal vein. 44 The marked dilatation of these periportal sinusoids causes mega sinusoids. Although it was infrequent to be seen, as reported by Nayak et al. 18 (4 among 10 patients), this histological finding was found at higher rates in other studies.31,43,44 Ludwig et al. 43 reported that mega sinusoids were found in 65% of patients (17 patients), while our analysis showed mega sinusoids in 53.3%. Another cause of INCPH in HIV patients is NRH. 25 This finding is characterized by the regeneration of hepatic cells in the form of diffuse non-neoplastic nodules with no connecting fibrous septa. 49 These nodules may be due to hepatocellular atrophy and the hepatotropic factors caused by portal vein obstruction. 45 Mallet et al. 25 reported NRH in 7 patients among 8 HIV patients, while we report a 38.6% incidence of NRH, which is relatively similar to results reported in Ludwig (25%). 49 Herniation of portal vessels and their leakage of surrounding hepatic parenchyma is called shunt vessels. A previous study described shunt vessels in 3 patients among 13 with INCPH. 29 A higher incidence was found in our study; 42.4% but even the higher incidence ofshunt vessels may be present without the occurrence of PH. 29
In terms of our study's strengths, we attempted to conduct a comprehensive search to obtain considerable evidence. The included studies’ quality reaches a trusted standard of proof. We analyzed all of the histopathological features identified in the included studies with a relatively large number of patients. However, there are some limitations, such as the marked heterogeneity which could not be resolved. Some histopathological features were reported by only a small number of studies. All of the included studies were retrospective and observational in nature. Furthermore, they were primarily conducted at tertiary referral centers where patients may have more severe or atypical presentations of IPH compared to those cases managed in primary or secondary care settings. This could have influenced the observed histopathological features in our study and may limit the generalizability of our findings to the broader IPH population. Furthermore, HIV-positive patients in the study population may have skewed the overall results, particularly for certain histopathological findings.
Conclusion
We concluded that, due to the relatively non-pathognomonic and non-specific nature of IPH, a combination of different histological features such as the portal and periportal fibrosis, portal vein sclerosis, mega-sinusoids, narrowing of portal veins, hepatic venous outflow obstruction, aberrant portal or periportal vessels, and ductular proliferation might be of value in diagnosing IPH as the incidence rate of these features was at least 50%.
Supplemental Material
sj-docx-1-sci-10.1177_00368504241264996 - Supplemental material for Histopathological features of idiopathic portal hypertension: A systematic review and meta-analysis
Supplemental material, sj-docx-1-sci-10.1177_00368504241264996 for Histopathological features of idiopathic portal hypertension: A systematic review and meta-analysis by Adnan Malik, Sohira Malik, Ahsan Farooq, Muhammad Imran Malik and Sadia Javaid in Science Progress
Footnotes
Data availability statement
Data will be available to any researcher who contacts the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.