
Abstract
Objective
Polytrauma is a complex condition associated with poor outcomes and high mortality rates resulting from severe damage and complicated complications. This study sought to ascertain the incidence of chronic complications in polytrauma patients, as well as the early immune changes and risk factors.
Methods
A multicenter, prospective and observational cohort study was conducted at the emergency surgery or traumatic intensive care unit (TICU) of the Advanced Trauma Center from August 2020 to July 2023. A total of 2033 consecutive trauma patients were included in the study. In the first 1, 7, and 14 days after admission, flow cytometry and immunoassay kits were used to examine cytokine release and lymphocyte count.
Results
Trauma patients were reported 33.8% (687/2033) chronic complication rates, with monotrauma patients reported 8.1% (55/683) and polytrauma patients reported 59.4% (802/1350). And the four most frequent chronic complications in polytrauma patients were chronic musculoskeletal pain (30.4%), post-traumatic osteoarthritis (27.2%), chronic wound (21.6%), and chronic lung injury (14.1.%) .There were significant differences in lymphocyte ratios and cytokine levels, at 1, 7, and 14 day of admission between chronic complication groups (CCP) and not chronic complication groups (N-CCP) in polytrauma. Polytrauma patients with characteristics of higher ratio of Ts7d ratio (95% CI: 2.01–6.21), Treg14d (95% CI: 1.12–5.43) and level of IL-67d (95% CI: 1.22–4.43), TNF-α7d (95% CI: 1.05–3.83), IL-1014d (95% CI: 2.01–6.84) were found to have a higher likelihood of experiencing a chronic complication. Conversely, a higher ratio of Tc1d (95% CI: 0.53–0.86), Th1d (95% CI: 0.64–0.95) and Th/Ts14d (95% CI: 0.21–0.64) were identified as independent protective factors against a chronic complication event.
Conclusion
Polytrauma patients exhibit a notable prevalence of chronic complications. Some immune and inflammatory indicators can be observed early in combination after injury to predict the risk of chronic complications after polytrauma.
Introduction
Polytrauma encompasses injuries affecting multiple bodily systems, frequently resulting in critical conditions that predispose patients to acute complications such as acute kidney injury (AKI), acute respiratory distress syndrome (ARDS), and acute gastrointestinal dysfunction (AGI).1,2 These complications collectively contribute to the development of multiple organ dysfunction syndrome (MODS). 3 Advances in prehospital care, contemporary intensive care practices, the establishment of specialized trauma centers, and enhanced surgical interventions have significantly improved the early-stage survival rate of severely injured patients, increasing it from 60% to 85–88% in recent decades. The nature of MODS appears to be changing.4,5 With improved survival rates, the long-term functional outcomes of polytrauma patients have garnered increased attention. 6 It is widely recognized that trauma can induce a cascade of inflammatory responses and oxidative stress, contributing to the development of various diseases. 7 Chronic complications (CCP), including chronic musculoskeletal pain, chronic wounds, and chronic lung or kidney disease, often manifest during the later stages of hospitalization and persist post-discharge. These complications continue to significantly impact patient outcomes and pose ongoing challenges for trauma care systems.8–10 Unfortunately, the incidence and characteristics of chronic complications in polytrauma patients are not well understood.
Trauma induces a cascade of rapid immunological alterations in the initial phases, aimed at clearing damaged tissues. Afterwards, repair mechanisms are activated in order to restore cells and tissues to pre-injury state.
11
However, if the initial injury is of significant severity, the immune response may become dysregulated.
12
To mitigate the systemic inflammatory response syndrome (SIRS) that is rapidly initiated post-injury, a redeeming anti-inflammatory response syndrome (CARS) concurrently arises. A key feature of CARS is an increase in circulating anti-inflammatory cytokines, apoptosis of lymphocytes, and a reduced production of cytokines by endotoxin-challenged monocytes.13,14 Dysregulated and prolonged SIRS/CARS responses have been shown to delay physical recovery, cause organ dysfunction, and increase mortality and nosocomial infection risk over the past decade.13,15 These patients may develop chronic complications, continuing to exhibit cytokine profiles indicative of chronic inflammation and biomarker profiles characteristic of persistent immunosuppression.16,17 Additionally, a significant proportion of these individuals often require prolonged treatment in long-term acute care facilities. One year after being discharged from the hospital, about half of these patients have succumbed to their conditions, and another quarter remain bedridden.
16
Consequently, it is imperative to enhance our understanding of these pathophysiological processes, as they represent a growing concern for society
Early identification of patients at risk for chronic complications is crucial in the management of polytrauma patients, and remains a significant challenge. Physicians may predict the risk of chronic complications by closely monitoring immune status, which can then guide the implementation of appropriate measures. Prophylactic treatments aim to mitigate the subsequent risks of chronic complications. The aims of this study were (a) to underscore the substantial public health concern posed by polytrauma, as evidenced by the frequency of chronic complications; and (b) to determine the value of early immune changes in predicting the development of chronic complications.
Materials and methods
Study design and patients
A multicenter, prospective, and observational cohort study was performed at the emergency surgery or traumatic intensive care unit (TICU) of four Level I trauma centers (verified by China Trauma Rescue & Treatment Association (CTRTA)) from August 2020 to July 2023. This research received approval from the Institutional Review Board at Tongji Hospital Institutional Review Board at the Huazhong University of Science and Technology (IRB number: TJ-IRB20200720; approval date: 22 July 2020). Additionally, each participating study site obtained approval from their respective local review boards: Xiantao First People's Hospital Institutional Review Board (IRB number: 2023-01-001; approval date: 10 January 2023), Tianmen First People's Hospital Institutional Review Board (IRB number:2020010097; approval date: 8 January 2020), and Xiangyang Central Hospital Institutional Review Board (IRB number: none; approval date: 10 October 2021). This study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2013. Written informed consent for the study was obtained from each patient or their legally authorized representative, as some patients may lack the capacity to provide consent due to their medical conditions, such as being in a comatose or sedated state following trauma. All patient details have been de-identified to ensure that individuals cannot be identified in any way. The reporting of this study conforms to STROBE guidelines. 18
The inclusion criteria were as follows: (a) age ≥ 18 years; (b) patients with traumatic injury; (c) a first set of assessments within the first 24 hours after injury. Exclusion criteria: the patient or their family members state that the patient has a history of malignant tumors, metabolic or immune diseases, and uses hormones or immune preparations. Polytrauma patients meet the “new Berlin” definition as having AIS ≥ 3 in two or more body regions, along with at least one additional parameter such as hypotension, unconsciousness, acidosis, coagulopathy, or being over 70 years old. 19 Monotrauma, on the other hand, is defined as an AIS severity of ≥2 in a single body region with no injuries in other regions.20,21
A total of 2185 patients were consecutively enrolled across four trauma centers. Of these, 152 were excluded due to incomplete information or loss to follow-up (including deaths), leaving 2033 patients who met the inclusion criteria. After data query, trauma patients were separated into cohorts based on their site of injury: single trauma group versus polytrauma group, and based on events of chronic complications: chronic complications group (CCP) versus N-chronic complications group (N-CCP). In addition, 35 healthy volunteers were selected as the control group. The control group had no underlying diseases and had not previously used hormones or immune preparations.
Definition
Activity of daily living (ADL) or instrumental activity of daily living (IADL) disabilities were defined as impairments in basic self-care (e.g. bathing, dressing) and independent living tasks (e.g. managing finances, transportation), respectively, to assess functional dependence. 22 Application of vasoactive drugs entails the use of norepinephrine and dopamine throughout the patient's hospitalization. The specification of the drugs used was according to the existing research. 23 The Centers for Disease Control and Prevention (CDC) characterize chronic diseases as enduring conditions lasting at least 1 year that necessitate ongoing medical intervention or restrict activities of daily living, or both. 24 Supplemental Table S1 lists the chosen 6 chronic complications as well as their definitions (Supplementary appendix: Table S1).
Data collection
Sociodemographic characteristics of trauma were gathered from all patients in the trauma bay whenever feasible, or at the time of study enrollment, if applicable. Due to limitations, including the emergence of chronic complications in the later stages of hospitalization and post-discharge, not all patients were accessible for direct interaction at the trauma center. In instances where face-to-face communication was not possible, attempts were made to reach patients during outpatient follow-up appointments or through telephone communication. Clinical characteristics from the first 24 hours after admission were retrospectively collected from each patient's electronic medical and nursing records, including the Glasgow Coma Scale (GCS), Injury Severity Score (ISS), Shock Index (SI), and discharge-related documents. A record was kept of hospital events, including vasoactive drugs, mechanical ventilation, and length of stay in the intensive care unit.
On the day of admission (considered day 1), 15 mL of whole blood were collected. Additional samples were collected on days 7 and 14. For the control group, peripheral blood was collected once in the morning on an empty stomach. The blood samples were placed in heparinized vials (BD vacutainer sodium heparin 75 USP units, BD Frankline Lakes NJ, USA) and stored at -80 °C. The ratio of lymphocyte subsets in peripheral blood was detected by the FACScan flow cytometer (Beckman Coulter, Fullerton, CA, USA). According to the manufacturer's instructions, we measured levels of IL-1, IL-6, IL-8, IL-10, and TNF- in sera of patients using the LEGENDplex Human Th Cytokine Panel (Biolegend, San Diego, CA, USA).The specific test operation and data analysis methods refer to the author's previous research literature and related operation manuals.25,26
Study end points
The primary aim of this study was to evaluate the frequency of chronic complications in polytrauma patients, with additional objectives including the identification of risk factors linked to chronic complications and the elucidation of the correlation between immune disorders and such complications.
Statistical analysis
Before analyzing the data, we assessed normality and homogeneity of variance. Frequency counts and percentages were used to describe categorical variables, while continuous variables were presented as either median [IQR] or mean ± SD, depending on their distribution. For comparisons, we employed the Student's t-test, Mann–Whitney U test, or χ2 test, as appropriate. Using logistic regression, risk factors for chronic complications associated with polytrauma were identified. Propensity Score Matching (PSM) is employed as a statistical technique to mitigate confounding bias. In this research, the dependent variable was the CCP status (CCP or non-CCP), while age, gender, ISS scores, GCS scores, and SI level were considered as independent variables in a logistic regression model to derive the propensity score (PS). PSM was conducted utilizing the nearest neighbor matching method with a 1:1 matching ratio and a clamp value of 0.03, followed by an assessment of covariate balance between the CCP and non-CCP groups post-matching. Statistical analysis was performed with R software (version4.4.0) and GraphPad Prism software 9.3.1 (GraphPad Software Inc., San Diego, CA, USA).
Results
Case identification procedure
From August 2020 to July 2023, the trauma centers admitted a total of 2185 patients. Of these, 152 were excluded due to incomplete information or loss to follow-up (including deaths). The remaining 2033 consecutive patients met the inclusion criteria and were divided into the monotrauma group (n = 683) and the polytrauma group (n = 1350). Based on whether there is chronic complication or not, the monotrauma group is further divided into a chronic complication group (CCP, n = 55) and a N-chronic complication (N-CCP, n = 682), which for polytrauma group was a chronic complication group (CCP, n = 802) and a N-chronic complication (N-CCP, n = 548) (Figure 1).

Case identification procedure.
Distribution of chronic complication in trauma patients
As demonstrated in Table 1 and Figure 2, the incidence of chronic complications was highest among polytrauma patients (59.4%), compared with trauma patients (33.8%) and monotrauma patients (8.1%). And the four most frequent chronic complications in polytrauma patients were chronic musculoskeletal pain (30.4%), post-traumatic osteoarthritis (27.2%), chronic wound (21.6%), and chronic lung injury (14.1%) when compared with trauma patients and monotrauma patients.

Distribution of chronic complication in trauma patients. Bar Chart: Blue for trauma patients, orange for monotrauma, and gray for polytrauma, showing the incidence of chronic complications. Line Chart: Blue for trauma patients, orange for monotrauma, and gray for polytrauma, indicating the incidence of six complications.
Rate of chronic complication in trauma patients.

n/a = not.
Sociodemographic characteristics and hospital course between CCP and N-CCP groups in polytrauma patients
Table 2 presents the demographics and characteristics of polytrauma patients. The mean value of ISS was 22.8, while for GCS and SI were 10.9 and 0.9, respectively. Overall, 54.9% (741/1350) polytrauma patients suffered head injury, 64.1% (866/1350) polytrauma patients had a thorax injury, 19.1% (258/1350) suffered abdomen injury, 34.6% (467/1350) suffered spine injury, and 15.3% (207/1350) suffered pelvis injury, while lower-extremity and upper-extremity were recorded for 53.2% (718/1350) and 44.1% (596/1350) patients, respectively. The injury was mainly caused by car collision (37.9%, 511/1350), followed by electric bicycle collision (37.3%, 504/1350), and high-energy fall (20.9%, 283/1350) (Table 2).
Comparison of sociodemographic characteristics, hospital course and outcomes between CCP and n-CCP in polytrauma patients.
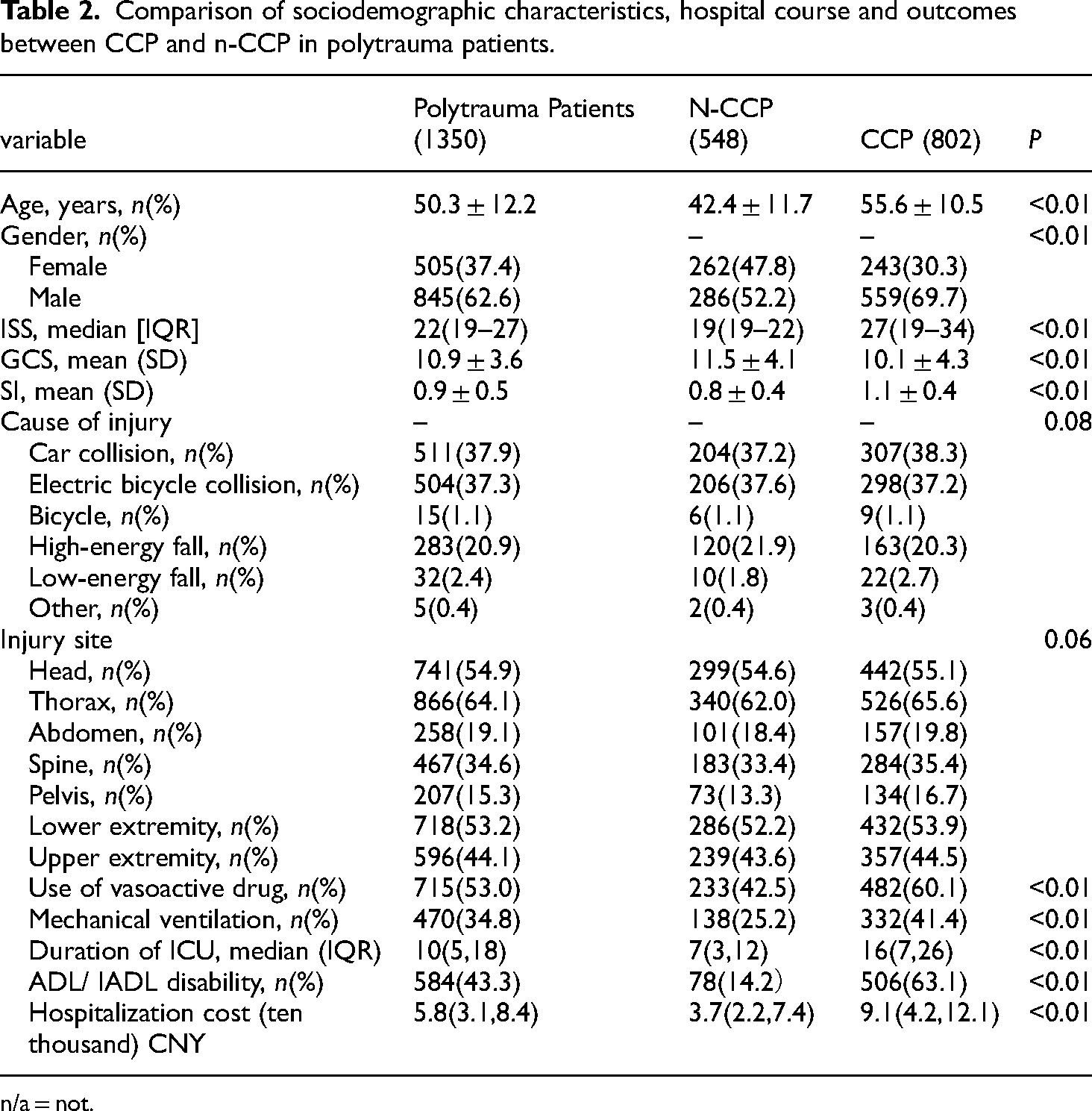
n/a = not.
Table 2 also depicts the comparison of sociodemographic characteristics and injury profile between the study groups. The CCP groups were predominantly male (69.7% vs. 52.2%; P < 0.01), and frequently with the mean age (55.6vs. 42.4; P < 0.01) when compared with n-CCP groups. The patients in the CCP groups were often more severe than that in n-CCP groups, as patients had higher ISS scores and lower GCS scores (P < 0.01). And those patients in CCP groups may have gone through a more severe shock as patients had higher SI scores (P < 0.01).In addition, the duration of ICU, the rate of mechanical ventilation and use of vasoactive drug were significantly different between the CCP groups and n-CCP groups in polytrauma (P < 0.01). The CCP groups had higher ratio of mechanical ventilation (41.4% vs. 25.2%, P < 0.01), use of vasoactive drug (60.1% vs. 42.5%, P < 0.01) and longer of ICU stays (16(days) vs.7(days), P < 0.01) (Table 2). As to disease burden, the CCP groups had higher rate of ADL/IADL disability (63.1% vs. 14.2%, P < 0.01) and hospitalization cost in polytrauma patients (9.1(ten thousand) vs.3.7(ten thousand), P < 0.01) when compared with N-CCP groups.
Early changes in lymphocyte and inflammatory cytokine levels between CCP and N-CCP in polytrauma patients
Before PSM, there were statistically significant differences in age, gender, ISS scores, GCS scores and SI level between the CCP and the N-CCP groups (P < 0.05). Using the PSM method to match the basic information of patients in a 1:1 ratio, a total of 362 study subjects was successfully matched, with a total of 724 cases. After PSM, there were no statistically significant differences in the baseline characteristics between the CCP and N-CCP groups (P > 0.05), as shown in Table 3.
PSM method to match the basic information of patients.

On the 1st day after polytrauma, a notable disparity in the ratio of total T lymphocytes (Tc) and helper T lymphocytes (Th) was observed between the CCP and N-CCP groups (P < 0.05). On the 7th days after polytrauma, there was a significant increase in the ratio of Treg cells in both the CCP and N-CCP groups, with a more pronounced elevation noted in the CCP group (P < 0.05). Additionally, an increase in the ratio of Ts cells and a decrease in the Th/Ts ratio in the CCP group were observed, which was statistically significant comparing with the N-CCP group (P < 0.05).On the 14th days after polytrauma, the ratio of Tc cells, Th cells and Th/Ts ratio in the CCP group were significantly lower, and the ratio of Ts cells and Treg cells were significantly higher than those in the N-CCP group (P < 0.05)(Table 4).
Lymphocyte and inflammatory cytokine levels between CCP and n-CCP in polytrauma patients.

Note: Compared with the N-CCP group, Pa < 0.05; Tc is total T lymphocytes, Th is helper T lymphocytes, Ts is inhibitory T lymphocytes, CTL is cytotoxic T lymphocytes, Th/Ts is helper T lymphocytes/inhibitory T lymphocytes, Treg is regulatory T lymphocytes, IL is interleukin, TNF- α for tumor necrosis factor-α.
On the 1st day following polytrauma, IL-6, IL-8, IL-10, and TNF- levels increased in both CCP and N-CCP groups. On 7th days after polytrauma, IL-6 and TNF-α levels in the N-CCP group had largely returned to baseline, whereas these cytokines remained significantly elevated in the CCP group compared with the N-CCP group (P < 0.05). Furthermore, IL-8 and IL-10- levels continued to rise in both groups at 7th days after polytrauma. Notably, IL-8 and IL-10- levels in the CCP group were significantly higher than those observed in the N-CCP group at 7th and 14th days after trauma (P < 0.05) (Table 4).
Risk factors for CCP in polytrauma
Risk factors for chronic complications in polytrauma patients have been thoroughly analyzed (Table 4). The results of the multivariate regression analysis revealed factors independently associated with chronic complications in polytrauma, as displayed in Table 5. Higher levels of Ts7d and IL-1014d were 3.04 (95% CI: 2.01–6.21) and 3.97 (2.01–6.84) times more likely to suffer from chronic complications, respectively. Moreover, patients with higher levels of Treg14d were 2.78 (1.12–5.43) times more likely to experience chronic complications, which for patients with higher levels of IL-67d and TNF-α7d were 2.18 (1.22–4.43) and 1.35 (1.05–3.83), respectively. A higher levels of Tc1d (OR = 0.73; 95%CI: 0.53–0.86), Th1d (OR = 0.82; 95%CI: 0.64–0.95) and Th/Ts14d (OR = 0.41; 95%CI: 0.21–0.64), conversely, were demonstrated to be independent protective factors from chronic complications event (Table 5).
Univariate and multivariate regression analyses of lymphocyte and inflammatory cytokine levels associated with CCP in polytrauma.

Discussion
Polytrauma is a multifaceted clinical condition associated with unfavorable outcomes and increased mortality rates as a result of severe injuries and various complications, thus posing a persistent health issue.1,27 The incidence of in-hospital complications has been reported to be as high as 60%,which are known to contribute to prolonged hospital stays, elevated healthcare costs, and increased mortality.28,29 Advances in the treatment and prevention of polytrauma, propelled by societal development and scientific and technological progress, have significantly improved the survival rates of severely injured patients. However, with increased survival rates, certain chronic complications tend to manifest during the later stages of hospitalization and even post-discharge. Chronic complications are defined variably but typically encompass the notions of enduring duration, significant impact on daily life, and the necessity for continuous management. 30 Recent research has identified extended manifestations of chronic complications linked to immunosuppression and infection.8,31,32 The prevalence of chronic complications in post-polytrauma patients remains undetermined. It is crucial to characterize these diverse chronic complications to advance our understanding of their underlying immune status and to develop novel diagnostic and therapeutic strategies.
To the best of our knowledge, this study represents the inaugural multicenter trial aimed at examining the incidence of chronic complications in polytrauma patients. Our findings suggest that polytrauma patients demonstrate a higher prevalence of chronic disease characteristics compared with monotrauma patients (59.4% vs. 33.8%). The most frequently observed chronic comorbidities in polytrauma patients include chronic musculoskeletal pain (30.4%), post-traumatic osteoarthritis (27.2%), chronic wounds (21.6%), and chronic lung injury (14.1%). Inflammation is recognized as a critical mechanism underlying various chronic musculoskeletal pain conditions, with sustained local or systemic inflammation and nervous system disorders subsequent to polytrauma serving as primary contributors to such pain.33,34 Prior studies have shown changes in the levels of specific cytokines in individuals with fibromyalgia, such as IFN-γ, IL-5, IL-6, IL-8, and the anti-inflammatory cytokine IL-10, subsequent to the stimulation of peripheral blood mononuclear cells (PBMCs). 35 Sepsis- and ARDS-induced lung inflammation frequently culminate in the development of pulmonary fibrosis, which is initially characterized by an inflammatory phase followed by extensive lung tissue necrosis. 36 The cytokines and chemokines released by type-1 and type-2 helper T-cells (Th1 and Th2) in response to lung injury, along with the recruitment of inflammatory cells, may contribute to the progression from injury to fibroproliferation. 37 Post-traumatic osteoarthritis is a chronic osteoarthropathy characterized by the progressive degeneration of articular cartilage and inflammation of the synovial joint. The activation of inflammatory mechanisms during the acute phase is believed to play a pivotal role in the onset of the chronic disease. 38 A substantial number of cytokines are produced immediately following injury, exerting long-lasting effects that may disrupt joint homeostasis and contribute to joint degeneration through various metabolic pathways. 39 Excessive neutrophil infiltration is a pivotal factor in the cycle of chronic inflammation and serves as a biological marker for chronic wounds. 8 Repetitive trauma, local tissue hypoxia, and substantial bacterial burden, in conjunction with increased infiltration of specific immune cell subsets, perpetuate a deleterious cycle that hinders progression into the proliferative phase of healing. 40 These phenomena represent adverse clinical outcomes resulting from persistent, imbalanced local or systemic inflammation following polytrauma.32,41–43
A traumatic injury causes a disturbance in the homeostasis of the immune system, affecting both innate and adaptive immune responses. This disturbance triggers an immediate activation of the innate immune response, prompting a swift cellular immune reaction aimed at addressing the threat posed by the traumatic injury. 44 Nonetheless, this response may lead to serious complications and potentially fatal consequences.45,46 The majority of patients who experience polytrauma and survive the initial 24–48 hours post-injury generally have a relatively favorable prognosis. 47 Notably, mortality following the initial phase is less frequently attributable directly to the trauma itself and more commonly results from infections and complications that arise, particularly under conditions of prolonged immunosuppression.48,49 These complications primarily involve diminished cytokine production, impaired monocyte-macrophage function, a sustained increase in myeloid-derived suppressor cells (MDSCs), and a reduction in both the number and functionality of effector T cells. 50 Cytotoxic T cells (Tc) and helper T cells (Th1) play essential roles in pathogen elimination and immune activation, yet trauma often dampens Tc function and dysregulates Th1 activity, increasing the risk of tissue damage. Suppressor T cells (Ts) and regulatory T cells (Treg) modulate this response, though their elevated presence post-trauma can shift the immune system toward a suppressive state, as indicated by a lower Th/Ts ratio and greater susceptibility to infection. 51 Key cytokines like IL-6 and TNF-α drive the inflammation necessary for healing, but if persistently elevated, they may lead to systemic inflammation and organ dysfunction. Conversely, IL-10 reduces inflammation but may contribute to immunosuppression when chronically high. 52 In this study, we describe the temporal changes in the ratio of T cells and cytokine levels in the peripheral blood of polytrauma patients with or not with chronic complication. We propose that in cases of polytrauma, the initial injury precipitates the development of chronic complications. Clinical evidence from our study supports this hypothesis, demonstrating that in polytrauma patients with chronic complications key mechanisms of immune imbalance are evident at an early stage. Specifically, within 24 hours, there is a significant down-regulation in the ratio of T cells and within 7 to 14 days, there is a notable up-regulation of serum levels of IL-6, IL-8, IL-10, and TNF-α, along with a relative increase in Tregs and Ts. These findings are consistent with previous research.53–55
In the context of identifying predictors of chronic complications following polytrauma, multivariate logistic regression analysis revealed that Tc 1 day, Th 1 day, Ts 7 days, Treg 14 days, Th/Ts 14 days, IL-6 7 days, TNF-α 7 days, and IL-10 14 days are significant risk factors. These findings suggest that early monitoring of these immune and inflammatory markers post-injury could facilitate the prediction of chronic complications. Consequently, early implementation of targeted therapeutic interventions may enhance the prognosis for patients experiencing polytrauma.
Limitation
This study is constrained by various limitations. Specifically, disparities in patient across individual studies may be influenced by diverse immunologic responses, such as gene polymorphisms, as well as potential confounding variables like the quantity and potency of therapeutic medications administered and the occurrence of subsequent surgical procedures. These factors can affect individual inflammatory responses and result in a tenuous association between immune status and particular complications. The majority of the included studies did not provide comprehensive details on these aspects. Moreover, despite chronic complications being categorized linking to international guidelines, the lack of unified diagnostic criteria for various chronic complication due to their complex nature. Therefore, the individual immune response in patients with chronic complications after polytrauma requires further study.
Conclusions
Our study characterized the incidence of chronic complications in polytrauma patients and further emphasized that polytrauma represents a substantial public health concern, as evidenced by its frequency of chronic complications. An imbalance of the immune system occurs after severely injured trauma at early stage and this phenomenon is more pronounced in polytrauma with chronic complication. Physicians may gain insight into the individual risk for chronic complications by monitoring lymphocyte and inflammatory cytokine secretion patterns closely.
Supplemental Material
sj-docx-1-sci-10.1177_00368504241305901 - Supplemental material for From trauma to chronicity: Understanding the incidence and early immune changes of chronic complications in polytrauma patients
Supplemental material, sj-docx-1-sci-10.1177_00368504241305901 for From trauma to chronicity: Understanding the incidence and early immune changes of chronic complications in polytrauma patients by Cong Zhang, Deng Chen, Qian Wan, Gang Yin, Yang Liu, Jialiu Luo, Shunyao Chen, Zhiqiang Lin, Shuaipeng Gu, Hui Li, Teding Chang, Liming Dong, Peidong Zhang and Zhaohui Tang in Science Progress
Supplemental Material
sj-pdf-2-sci-10.1177_00368504241305901 - Supplemental material for From trauma to chronicity: Understanding the incidence and early immune changes of chronic complications in polytrauma patients
Supplemental material, sj-pdf-2-sci-10.1177_00368504241305901 for From trauma to chronicity: Understanding the incidence and early immune changes of chronic complications in polytrauma patients by Cong Zhang, Deng Chen, Qian Wan, Gang Yin, Yang Liu, Jialiu Luo, Shunyao Chen, Zhiqiang Lin, Shuaipeng Gu, Hui Li, Teding Chang, Liming Dong, Peidong Zhang and Zhaohui Tang in Science Progress
Footnotes
Acknowledgments
The authors thank the staff at the Department of Clinical Statistics for their assistance in statistical analysis.
Authors contributions
Z.T. and P.Z. participated in the designing of the experiment, collection, analysis, and interpretation of data, and drafting the manuscript. D.C., Q.W., G.Y., Y.L., J.L., S.C., Z.L., S.G., H.L. L.D. and T.C. collected and analyzed data. C.Z. contributed to the collection and analysis of data and drafted the manuscript. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical, legal, and privacy issues.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Grants 81873870 (Z.T.) from the National Natural Science Foundation of China.
Institutional review board statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the ethics committee at Tongji Hospital (IRB number: TJ-IRB20200720; approval date: 22 July 2020), Xiantao first people's Hospital (approval date: 10 January 2023), Tianmen First People's Hospital Institutional Review Board (approval date: 8 January 2020), and Xiangyang Central Hospital Institutional Review Board (approval date: 10 October 2021).
Informed consent statement
Informed consent was obtained from each patient or the patient's legally authorized representative involved in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.