
Abstract
Langerhans cell histiocytosis (LCH) is a neoplastic disease characterized by aberrant proliferation of the mononuclear phagocyte system, predominantly affecting children under the age of 3 years. Although LCH can affect almost all organs, sinus involvement is rare. This case report documents a 9-year-old boy presented with vision impairment and intermittent headache on the right side. The CT scan and MRI examination revealed the presence of a soft mass in the right atrium of sphenoid sinus, which impacted the right optic canal. Biopsy results confirmed the presence of LCH. Considering the involvement of optic canal and vision impairment, meticulous debridement was performed followed by a 12-month standard chemotherapy. After 2 years of follow-up, the patient showed significant improvement, despite the presence of an encapsulated cyst in the right sphenoid sinus. This case highlights the importance of considering LCH when encountering an isolated soft mass accompanied by decreased vision in the sphenoid sinus. A thorough physical examination, laboratory tests, and imaging methods should be performed, with a biopsy being necessary to confirm the type of lesion and guide the appropriate treatment.
Introduction
Langerhans cell histiocytosis (LCH) is a rare disease characterized by mononuclear phagocyte system aberrant proliferation accompanied by infiltration of various types of inflammatory cells. 1 This disease typically manifests in pediatric population and can affect nearly all organs, with common presentations including lytic bone lesions and rashes. 2 The skull is commonly affected, with the orbit and mastoid being frequently involved. 3 Solitary sphenoid sinus LCH is an exceptionally unusual presentations with only a few isolated cases previously documented in the literature. It is important to note that other conditions, such as adenocarcinomas, squamous cell carcinomas, epidermoid carcinomas, and lymphoma, can also present as isolated soft masses with bone erosion in the sphenoid sinus.4,5 The definitive diagnosis or differential diagnosis relies on the examination of pathological specimens. In this case, we presented a 9-year-old boy exhibiting a soft tissue mass predominantly located in the right sphenoid sinus, accompanied by invasion of the optic canal. The biopsy revealed the presence of CD207, CD1a, S100 positive cells, indicating the diagnosis of LCH. The purpose of this article is to increase awareness of LCH in young patients presenting with soft masses and bone destruction in the sphenoid sinus.
Case report
The patient, a 9-year-old boy, was admitted to Wuhan Tongji Hospital in August 2021, presenting with a two-month history of intermittent right-sided headache accompanied by ipsilateral visual impairment. The initial onset of his headache occurred subsequent to intense physical exertion two months ago, and he experienced non-projectile emesis on three occasions during this time period, during which no interventions were made. There is no history of head trauma or rhinorrhea, postnasal drip, nasal congestion, hyposmia, epistaxis and other nasal symptoms. Apart from the impaired vision of the right eye (right 0.4, left 0.7), the pupillary light reflex was normal and he exhibited no oculomotor abnormalities, ocular discharge, or proptosis. There were no similar conditions among other family members.
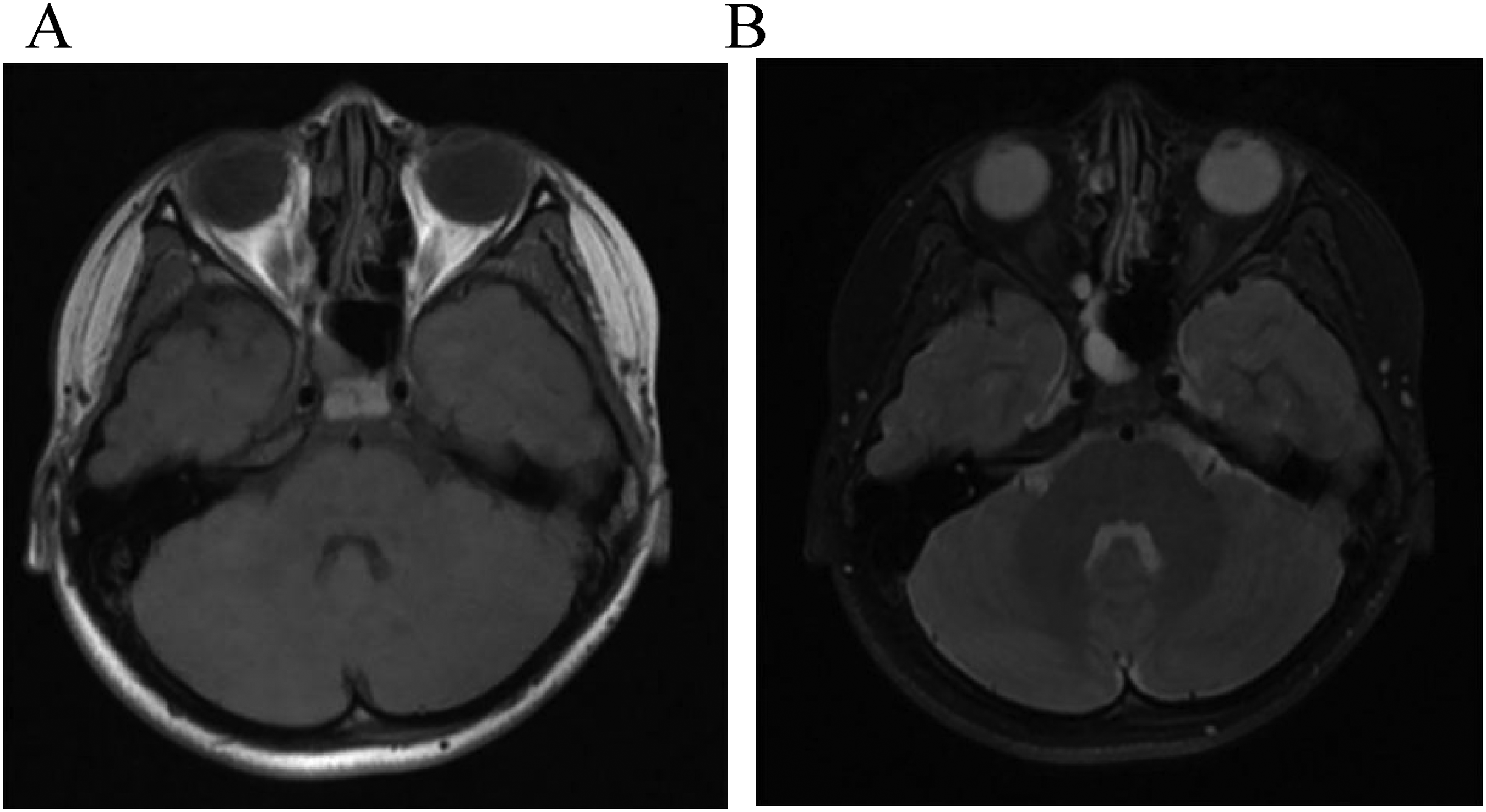
The patient's physical examination revealed no abnormalities except for right-sided vision loss, and he did not experience post-admission headaches. The laboratory tests, including a complete blood count, blood chemistry analysis, erythrocyte sedimentation rate (ESR) measurement, and coagulation function test, yielded results within the normal range. The CT scan showed a soft tissue mass with hyperdense foci in the right posterior ethmoid sinus and right sphenoid sinus atrium, accompanied by adjacent bone resorption (anterior sphenoid sinus wall, anterior skull base, orbital board), which may involve the right optic nerve canal (Figure 1). The subsequent MRI examination revealed that the presence of a nodular lesion with a short T2 signal shadow, occupying the right atrium of the sphenoid sinus and posterior ethmoid sinus, accompanied by bone resorption in the optic canal. The right optic nerve was slightly distorted as evidenced by the uneven signals within it. The brain parenchyma showed no obvious abnormal signals, and there was no central nervous system (CNS) involvement such as pituitary lesions or pituitary stalk thickening (Figure 1). To determine the presence of any additional sites involved, initial screening with chest radiography and abdominal ultrasonography was performed, yielding negative results. Subsequently, a more comprehensive examination, 18F-fluorodeoxyglucose (FDG) PET/CT, was performed to screen for the occult lesions. 6 No FDG accumulation was observed in either the right sphenoid sinus or other anatomical regions.

Ct axial (A) and coronal (B) scan showed a soft tissue mass (approximately 17 × 16 mm) with hyperdense foci in the right posterior ethmoid sinus and sphenoid sinus with the involvement of right optic nerve canal and erosion of adjacent bone. T1-weighted MRI (C) indicated an isointense mass and T2-weighted MRI (D) indicated a hypointense soft-tissue in the right posterior ethmoid sinus and sphenoid sinus with the involvement of right optic nerve canal and erosion of adjacent bone. An uneven signal in the right optic nerve suggested the mass had affected it.
The definitive diagnosis was obtained by performing a biopsy through endoscopic sinus surgery. Intraoperatively, the right posterior ethmoid sinus pyocyst was identified, and the sphenoid sinus cavity was filled with smooth and pale neoplasm. The pathological results showed the histiocytic cell was stained positively for langerin (CD207), CD1a, CD68, CD163, S100 and Ki67. BRAF V600E mutation was identified in cell-free DNA from the blood of the patient. Consequently, the patient received a diagnosis of LCH exclusively localized in the sphenoid sinus. Considering the involvement of the right optic nerve canal and impaired vision, the surgical procedure of debridement was conducted to decompress the optic nerve canal and excise the neoplasm. During the surgical procedure, a soft, smooth and pale mass was identified in the right sphenoid sinus, accompanied by partial destruction of the optic nerve canal (Figure 2). Sequentially, the technique of blunt dissection was employed to carefully remove the mass from the upper, medial, and posterior walls of the right sphenoid sinus as well as the right optic canal. The other parts of the wall of sphenoid sinus were relatively contact.

During the endoscopic endonasal surgery, a soft, smooth and pale mass was found in the right sphenoid sinus (A) and optic nerve canal was partially destroyed when the mass was carefully removed (B). Arrow indicates the mass and arrowhead indicates the bone lesion of the optic nerve canal.
The patient exhibited a satisfactory postoperative recovery, devoid of any ocular motility disorders, visual impairment, or headaches. The vision in the patient's right eye improved after the surgical intervention (right 0.5, left 0.7), suggesting that the tumor's pressure on the optic nerve was relieved. Considering the involvement of the optic nerve, a standard first-line therapy involving vinblastine and prednisone was administered to this patient for a duration of 12 months following surgery.
After a two-year follow-up, no evidence of recurrence was found through MRI examination, although there was an encapsulated effusion in the right sphenoid sinus (Figure 3).
Two years after the surgery, axial T1-weighted MRI scan (A)showed there was not abnormal soft tissue in the sella turcica; axial fat-suppressed T2-weighted MRI scan (B) showed there was an encapsulated effusion in right sphenoid sinus.
Discussion
LCH was previously referred to as histiocytosis X, the incidence of LCH was reported to be 4.6 per million in children under the age of 15. 7 There are several classification methods for categorizing LCH based on its clinical presentation. The most widely accepted one was based on whether single system (SS-LCH) or multisystem (MS-LCH) was involved and this classification provides a basis for the treatment of LCH (as shown later in the corresponding part). 8 Sphenoid sinus disease primarily arises from the spread of nearby lesions. It is termed isolated sphenoid sinus disease (ISSD) when exclusively the sphenoid sinus is affected, while other sinuses remain uninvolved. In cases of ISSD, inflammation and tumors are the most frequent causative factors, with inflammation accounting for 75% of instances and tumors for 18.9%. 9 The incidence of ISSD in children is only 0.4% of all paranasal sinuses. 10 LCH in the sphenoid sinus is exceedingly rare in the child population.
The etiology of LCH remains incompletely understood, and there has been ongoing debate regarding whether LCH should be classified as an immune disorder or a neoplasm. 11 Some scholars have reported that genetic, cytokine mediation, immunologic derangement and virus infection played important roles in the pathogenesis of LCH. 12 A groundbreaking study conducted in 2010 found that over half of patients diagnosed with LCH exhibited BRAF (V600E) mutations, which have been associated with the development of malignant proliferation. 13 The mutation of MAP2K1 is also frequently observed in patients with LCH, with reported frequencies reaching up to 33%. However, this mutation is exclusively found in individuals harboring wild-type BRAF. 14 These mutations can lead to the abnormal activation of the MAPK (mitogen-activated protein kinase) pathway, which provides strong evidence for characterizing LCH as a clonally expanding myeloid neoplasm. 15
The clinical manifestation of LCH depends on the affected organs. The bone is the most commonly involved organ (80%), while involvement of the central nervous system excluding the pituitary is rare(2–4%). 16 Pain and swelling are the most typical symptoms when the bone was involved, whereas cutaneous involvement typically presents as seborrheic dermatitis-like eruption, pinpoint erythematous or papules or pustules. 17 ISSD presents with symptoms that are non-specific. In pediatric cases, the predominant clinical symptom is a persistent headache. Should the lesion encroach upon the optic nerve, the patient may suffer from vision loss, experience double vision, or encounter visual fatigue. 9 Depending on the underlying etiology, inflammatory ISSD may present with symptoms such as nasal congestion, nasal discharge, postnasal drip and fever. 18 In case of severe acute bacterial or invasive fungal infections, the condition may lead to cranial nerves palsy, epidural abscesses, and may extend into to the cavernous sinus, resulting in cavernous sinus infection, cavernous sinus thrombosis, and other severe complications. 19 LCH is a primary tumor of the sphenoid sinus. When the mass extends to invade the pituitary gland, the clinical manifestations of thirst and urolithiasis may occur. 20 Vomiting, spreading nerve palsy, hypoesthesia of the trigeminal nerve, hyperreflexia of the limbs, and increased plantar reflexes may occur if the lesion extends to the parasellar and petrous areas. 21 Solitary occurrences of LCH in the sphenoid sinus have been reported in only a few cases.20–25 We summarized these cases in Table 1 in terms of published year, gender, age, chief complaint, extent of the lesion, therapy and follow-up period.
Summary of reported cases of solitary LCH in sphenoid sinus.

The diagnosis of LCH relies on pathological examination, which reveals the presence of CD1a, S100 and Langerin (CD207) positive histiocytes with an inflammatory background. 26 Therefore, whenever possible, biopsy should be performed. Given that LCH can result in bony destruction, primary malignant tumors or metastatic tumors are the most important conditions that needs to be differentiated from LCH. Therefore, in this case, a PET-CT was conducted. The results indicated that a low-density shadow in the right sphenoid sinus with adjacent bone absorption, however, no increase in glycolytic metabolism was observed within it. Furthermore, no abnormal uptake of FDG was observed in any other anatomical regions. Due to the erosion of adjacent bone of the mass, malignant tumors, such as adenocarcinomas, squamous cell carcinomas, epidermoid carcinomas, lymphoma and giant cell tumor should be taken into consideration.4–6 Although invasive fungal disease would lead to bone erosion, it usually occurs in patients with immunodeficiency and there is no sufficient evidence to support it in this case. 27
Observation (without functional impairment) or local treatment (with functional impairment) is sufficient in SS-LCH with single site affected; systematic treatments are required in SS-LCH with multiple sites affected or MS-LCH. 16 The standard systematic therapy is vinblastine and prednisone for 12 months. 28 As more and more evidence showed that LCH is driven by the abnormal activation of MAPK pathway, several targeted agents, such as, vemurafenib have shown preliminary efficacy and safety, however, further clinical trials are still needed before these targeted agents used clinically. 29 Although radiotherapy was applied in certain cases (Table 1), a retrospective study showed that out of 12 patients with MS-LCH who received primary radiotherapy, five succumbed to the disease. 30 Accordingly, radiotherapy is not recommended as a standard treatment. 3 In this case, despite maximal surgical removal of the neoplasm, residual remnants remained due to the inherent risks associated with performing an extended resection in the sphenoid sinus. Consequently, a standard treatment was applied to this patient. 28 Due to LCH has a relatively high reactivation rate, it is recommended to conduct a minimum follow-up period of 5 years for all patients with LCH. 16 In this case, there was not any sign of recurrence after 2 years of follow-up, although an encapsulated effusion was found in right sphenoid sinus. The presence of encapsulated effusion might be due to incomplete development of the sphenoid sinus in children, a small sphenoid sinus opening during surgery, postoperative scarring leading to a narrowed sphenoid sinus opening, and subsequently impeded drainage.
Conclusion
This case highlights the possibility of LCH when the lesion presents as a solitary soft tissue mass with circumambient bone destruction in sphenoid sinus. Given that the clinical manifestation of several other conditions described above are similar to LCH in sphenoid sinus, obtaining pathological findings through biopsy is crucial for establishing a definitive diagnosis. Our experience suggests that surgical excision followed by a standard systematic treatment may an effective approach to managing LCH involving the optic nerve canal in the sphenoid sinus.
Footnotes
Abbreviations
Acknowledgements
I would particularly like to acknowledge my teammate, Yu-Ting Wang, for her wonderful collaboration and patient support.
Author contributions
Min-Shan Li. searched literature for this case and wrote the manuscript, Xing-Liang Wu and Ao Hang participate in revising the manuscript. H.W. designed the clinical case and prepared the manuscript. All authors have read and agreed to the published version of the manuscript.
Author's note
The authors obtained informed consent for publication of the case report and associated images from the legally authorised representatives, who signed a written informed consent form.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from * Committee of Tongji Hospital, Huazhong University of Science and Technology (TJ-IRB20231238)*.
Funding
This study was supported by the National Nature Science Foundation of China (NSFC) grant 81873694 (H.W.), the key Research and Development Program of Hubei Province 2022BCA005(H.W.), Knowledge Innovation Program of Wuhan-Basic Research 2022020801010446(H.W.).
Informed consent
Written informed consent was obtained from the patient's legal representative for the anonymised information published in this article.