
Abstract
Due to the insidious nature of pediatric cardiac Behçet's disease (BD), misdiagnosis or missed diagnosis occurred frequently. We described a female pediatric patient with BD with cardiac valvular involvement diagnosed at the age of 4 years with clinical symptoms, including aphthous ulcers, fever, perianal ulcers, and erythema nodosum, as well as significantly elevated inflammatory markers. Echocardiography revealed that previously absent aortic valve lesions developed later and gradually worsened. After being diagnosed with BD with cardiovascular involvement, the patient was treated with glucocorticoids, immunosuppressants, biologics, diuretics, and aortic valvuloplasty. At the time of the follow up, the patient was stable. A review of 13 publications was conducted, including 14 cases of cardiac involvement in pediatric BD.
Background
Behçet's disease (BD) is a type of primary systemic vasculitis that causes oral ulcers, genital ulcers, uveitis, skin lesions, and multisystem involvement. More rheumatologists consider it a syndrome in recent years. 1 The disease prevalence varies (1–370/100,000 people) according to geographical factors as well: the highest value is observed in Turkey and, more broadly, in countries crossed by the so-called Silk Road, including the Middle East and far-east Asia. 2 Pediatric BD accounts for approximately 1.6% to 7.7% of all BD cases.3,4 The highly heterogeneous clinical manifestations of pediatric BD and the lack of specific biomarkers make early diagnosis more difficult. Furthermore, cardiac involvement in BD, including pericarditis, myocarditis, endocarditis, and cardiac valvulopathy, is a major cause of poor outcome in patients with BD, with a mortality rate of up to 20%. 5 This study now presents a case of pediatric BD in our center, with cardiac valve lesions as the main symptom. We also reviewed relevant literature to better understand the clinical characteristics of cardiac lesions and to improve diagnosis and treatment in pediatric BD.
Case presentation
On December 1, 2020, a 4-year-old girl was admitted to our center. She had a 1-year history of oral ulcers and a 10-month history of fever, erythema nodosum, perianal ulcer, and fatigue. In her medical history, she was admitted to another hospital 10 months prior (February 2020), laboratory tests showed white blood cell (WBC): 15.5 × 103/µL, hemoglobin 97 g/L, platelets 532 × 103/µL, C-reactive protein (CRP): 124 mg/L, erythrocyte sedimentation rate (ESR): 83 mm/H, antistreptolysin O was normal. Both influenza A and B virus antigens yielded positive results. Doppler echocardiography was used to detect minor tricuspid regurgitation signals. At that hospital, she was given antibiotics for more than 20 days, but her symptoms did not improve. She was then given oral ibuprofen for 1 month (5 mg/kg/each time, twice a day), and her body temperature returned to normal, but her oral ulcers and fatigue persisted.
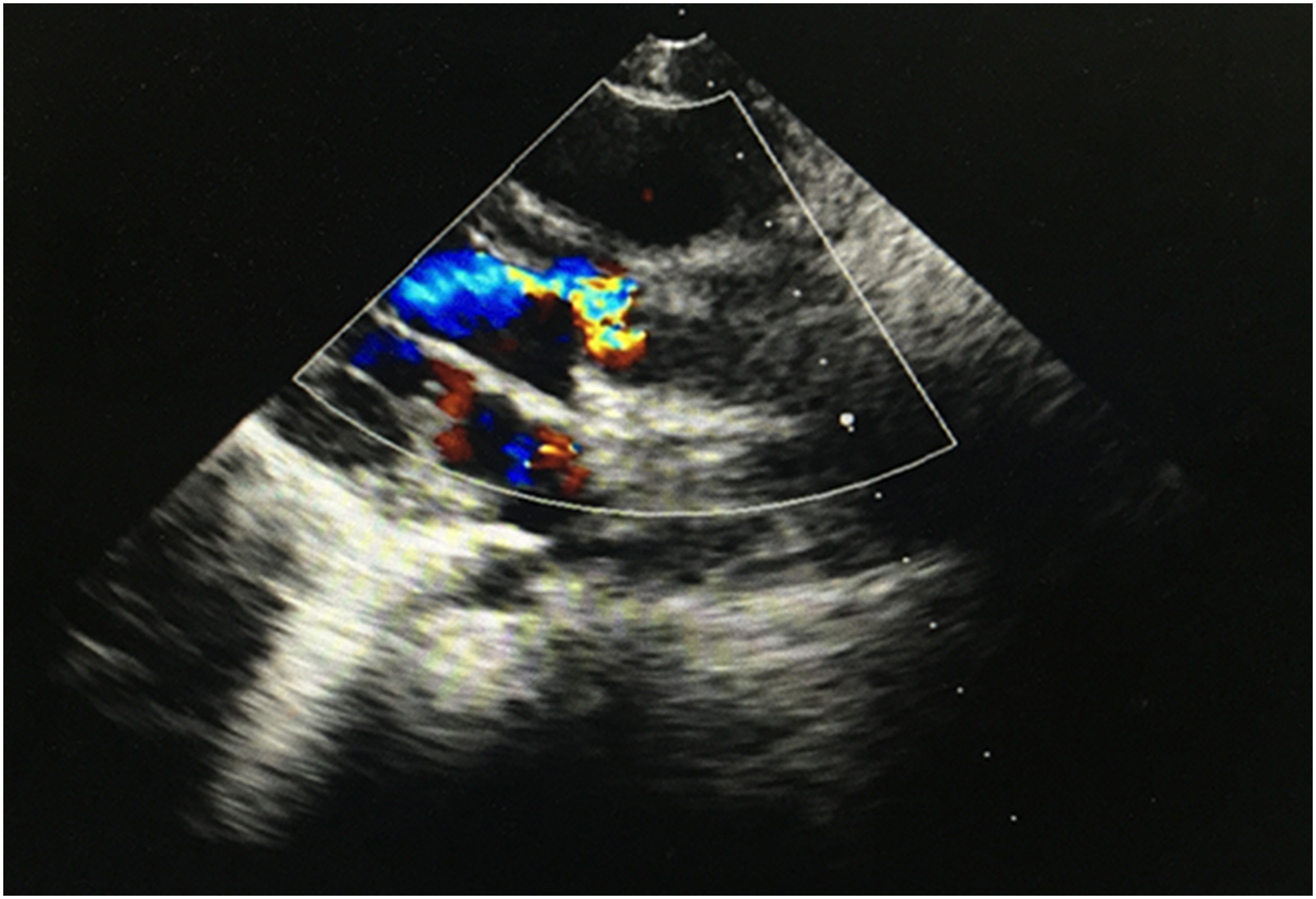
She had a cardiac murmur on auscultation 5 months earlier (in July 2020) during a visit to another clinic for diarrhea, but no further treatment was given. Two months ago (October 2020), she went to another hospital for echocardiography and found thickened leaflets and a mass that seemed to be vegetation on the aortic valve, accompanied by left ventricular enlargement. Coronary ultrasound revealed left coronary trunk expansion (3.2 mm, Z = + 2.72). An ambulatory electrocardiogram for 24 h revealed paroxysmal sinus tachycardia (heart rate, mean: 101 bpm, maximum: 173 bpm). She was evaluated at several hospitals, including ours (Figure 1). Echocardiography revealed that the leaflets in the aortic valve were enhanced and thickened, indicating aortic insufficiency with massive regurgitation.

Echocardiography of the patient in the present study before surgery. Three leaflets in the aortic valve are identified by echocardiography. Fusion of the noncoronary leaflet with the root of the anterior semilunar valve is also evident; the leaflets are enhanced and thickened. Redundancy of the noncoronary leaflet results in prolapse into the left ventricular outflow tract and poor valve closure. Aortic insufficiency accompanied by massive regurgitation.
She had been experiencing daily hyperpyrexia for 2 weeks (mid-November 2020). The patient was transferred to our center for additional treatment (December 2020).
Her past and family history were unremarkable.
The physical examination on admission was unremarkable, with the exception of hyperpigmentation in the bilateral distal lower extremities and a grade 3/6 rumbling diastolic murmur at the cardiac apex. Laboratory investigation revealed WBC 12.9 × 103/µL, hemoglobin 112 g/L, platelets 614 × 103/µL, CRP 81.7 mg/L, ESR 58 mm/H, the levels of N-terminal pro-brain natriuretic peptide (NT-proBNP) were increased (1270 pg/mL), creatine kinase, cardiac troponin T, and myoglobin were normal. Serological tests for tuberculin, Epstein-Barr virus, fungus, and Brucella were negative, and no bacteria were found in blood cultures. Rheumatoid factor, antinuclear antibodies, antidouble-stranded DNA (dsDNA), anti-Ro Sjogren A (SSA), anti-La Sjogren B (SSB), anticardiolipin antibody, and antineutrophil cytoplasmic antibodies were negative. The chest and abdomen computer tomography angiograms and the carotid and limbs vascular ultrasound were unremarkable. Pathology, bone marrow cytology, ophthalmology, and genetic testing (whole-exome sequencing) were all normal. There was no testing for human leukocyte antigen-B51 (HLA-B51). The colonoscopy was not performed because the patient's parents objected.
Following an examination of the patient's medical history, Kawasaki disease and rheumatic fever were ruled out. The diagnosis of BD was made using the International Criteria for BD in 2013 6 and the Pediatric BD classification criteria in 2016. 7 The patient was first given methylprednisolone tablets (equivalent to 1 mg/kg/day prednisone), torasemide tablets, and pulse cyclophosphamide (800 mg/m 2 ). Given the severity of the aortic valve damage, aggressive treatment was required to create the conditions for surgery. So, infliximab (6 mg/kg) and thalidomide (0.75 mg/kg/day) were added 5 days later. Her temperature returned to normal the next day after taking oral glucocorticoids. WBC, ESR, and CRP retests returned to normal in the first week of treatment, while NT-proBNP retests returned to normal in the first month. However, echocardiography revealed significant left cardiac enlargement, posterior semilunar valve (noncoronary leaflet) prolapses, and damage to the anterior and right posterior semilunar valves (noncoronary leaflets) of the aortic valve, indicating progressive valvar impairment. The patient underwent aortic valvuloplasty 3 months after starting treatment. Following surgery, there was a significant reduction in aortic valve regurgitation (Figure 2). Aspirin (3 mg/kg/day) was given. During the follow up, cyclophosphamide (once a month, 6 times total) and infliximab (14 times total) were still administered on a regular basis, while orally methylprednisolone tablets (dosage gradually decreased), thalidomide, aspirin, and torasemide tablets, clinical symptoms disappeared, laboratory tests were normal, and the patient's condition was stable (Table 1).
Echocardiography of the patient in the present study after surgery. Echocardiography suggests significantly lower aortic valve regurgitation than before.
The longitudinal course of this patient.
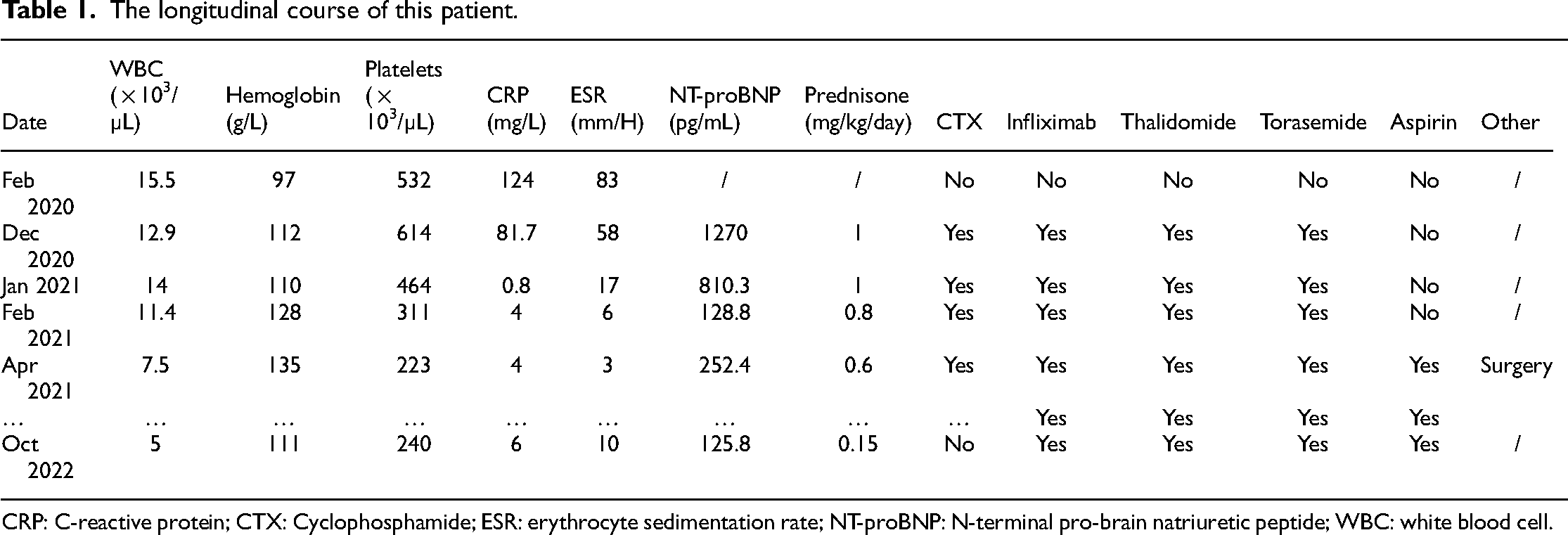
CRP: C-reactive protein; CTX: Cyclophosphamide; ESR: erythrocyte sedimentation rate; NT-proBNP: N-terminal pro-brain natriuretic peptide; WBC: white blood cell.
Discussion
In a large series, 8 cardiac involvement was reported to be between 2.4% and 12.1% in patients with BD. The prevalence of cardiac involvement in pediatric BD is unknown. Adults were found to have a 6% to 50% incidence of heart valve disorders. The aortic valve is the most commonly involved, with an incidence of up to 57.1% and 67.9%. It is frequently reflected on the echocardiogram as leaflet prolapse, though the mitral and tricuspid valves may also be involved. 9 Our patient had no obvious symptoms of cardiac involvement, and her progression from no valve lesions to irreversible valve damage was very gradual. This patient's aortic valve lesions were distinguished by thickened and prolapsed leaflets and poor valve closure. No cases of aortic valve leaflet damage in pediatric BD have been reported. To learn more about the cardiac involvement of pediatric BD, we used the search string “Behçet's, cardiac, pediatric” in PubMed (published between January 1990 and March 2021). There were 13 closely related publications,10–22 and 14 cases of cardiac involvement in pediatric BD were summarized. There were no large-scale case studies on pediatric BD cardiac valvular involvement. By summarizing these studies, we discovered that cardiac involvement in children was primarily manifested as intracardiac thrombus (10/14), coronary artery involvement (5/14), and valvular involvement (2/14) (Table 2), which differed from that of adult patients.8,23 Furthermore, we discovered that the current case had the youngest age of disease onset reported in the literature among pediatric BD with cardiac involvement and was the only case with aortic valve damage. The characteristics of pediatric disease onset, population sample size, and/or regional differences may all play a role in the possible cause of such variation between adults and children.
Manifestations of cardiac involvement in pediatric Behçet disease.

AV, aortic valve; ECG: electrocardiogram; LA, left atrial; LV, left ventricular; RA, right atrial; RV, right ventricular; Y, yes.
HLA-B51 is the most common and dominant genetic marker associated with BD. HLA-B15, B27, B40, B44, B52, B57, and A26, on the other hand, have been identified as minor but independent risk alleles of BD in various populations. 24 However, when we asked her about her family history, we discovered that not only did she have no relevant family history, but no family members had similar symptoms.
Treatment is determined by the severity of the disease and the organs affected. Glucocorticoid therapy combined with immunosuppressive therapy 8 is the mainstay of BD management. Because of the patient's young age and the presence of both aortic and coronary artery involvement, aggressive treatment was administered in light of these risk factors. In recent years, infliximab and adalimumab have been increasingly used to treat refractory BDs such as BD uveitis, central nervous system involvement, intestinal BD, and cardiac BD. It has been reported that infiximab and adalimumab have comparable efficacy in patients with severe and refractory BD, and patients who received adalimumab as antitumor necrosis factor (TNF therapy. The clinical response was rapid, impressive, and complete. 25 Thalidomide has immunomodulatory, anti-TNF-α, and antiangiogenic properties, making it useful for various inflammatory disorders. 26 The patient in the study experienced long-term remission of symptoms after receiving adequate doses of glucocorticoids along with cyclophosphamide and infliximab. However, the progressive worsening of irreversible valvular damage necessitates additional surgical intervention. Is she a candidate for the surgery? How can the opportunity for operation be grasped? The literature has revealed an extremely high prevalence of paravalvular leak following aortic valve replacement in patients with comorbid BD valvular lesions who underwent surgical treatment during the disease's active period. 27 Therefore, to avoid re-operation and minimize postoperative complications, it is critical to control the primary disease pre-operatively and apply appropriate postoperative maintenance therapy with immunosuppressants. 28 The patient in this study received aggressive medical treatment, and all primary symptoms and inflammatory markers improved. Furthermore, the combination of biologics and immunosuppressants was successful in lowering the patient's glucocorticoid dosage to a safe range for surgery. These conditions and opportunities made the surgery possible. After a thorough evaluation by rheumatology and cardiac surgery specialists, the patient's aortic valvuloplasty was successfully performed. Echocardiography revealed a significant reduction in aortic valve regurgitation, indicating that the aortic valve had been repaired. She was treated by sequential rheumatology after surgery. The patient has been stable for more than a year following surgery.
In conclusion, the symptoms of cardiac involvement in pediatric BD may be subtle, and the progression from no valve lesions to irreversible valve damage was insidious. Therefore, early detection of pediatric cardiac BD is difficult. Active treatment and close monitoring of echocardiography may improve these patients’ outcomes. To improve the prognosis, personalized treatment regimens should be developed through multidisciplinary consultation.
Footnotes
Acknowledgements
Thanks to all the participants for their involvement in the study.
Contributors’ statement
XY and X-NW collected data, carried out the initial analyses, drafted the initial manuscript, and reviewed and revised the manuscript. X-NW critically reviewed the manuscript. J-ML conceptualized and designed the study, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Data availability statement
All data generated or analyzed during this study are included in this article.
Ethics approval
Written informed consent was obtained from the patients for their anonymized information to be published in this article. This study was approved by the ethics committee of the Capital Institute of Pediatrics.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Xin Yao is an attending pediatric physician, studying for a PhD in pediatrics. Her area of research is Rheumatic diseases in children focusing on immune pathogenesis.
Xing-Ning Wang is an associate chief physician of pediatric, holds a PhD in Pediatrics. Her area of research is Rheumatic diseases and Immune disease in children.
Jian-Ming Lai, professor of pediatrics, committee member of Beijing Rheumatology Society, has rich experience in the diagnosis and treatment of systemic lupus erythematosus, juvenile idiopathic arthritis, Kawasaki disease and other pediatrics diseases.