
Abstract
Background:
The atresia rate of sphenoid ostium after endoscopic sphenoidotomy for isolated sphenoid disease is 9.4%–10.2%.
Aims:
To reduce sphenoid sinus ostium atresia rate after sphenoidotomy surgery.
Materials and Methods:
The data of patients with isolated sphenoid sinus disease at our hospital between 2015 and 2022 were retrospectively analyzed. The age, gender, disease course, pathology, postoperative follow-up time, anatomy data of sphenoid sinus and postoperative sinus ostium atresia rate were compared between the two groups of patients with traditional sphenoidotomy and modified sphenoidotomy.
Results:
A total of 117 patients with isolated sphenoid sinus disease underwent endoscopic sphenoidotomy. There were 76 cases in the traditional sphenoidotomy group, fungus ball in 59.2% of patients, the postoperative sinus ostium atresia rate was 14.5%. There were 41 cases in the modified sphenoidotomy group, fungus ball in 53.6% of patients, and 0 case of sinus ostium atresia. Statistical analysis showed significant differences in postoperative sinus ostium atresia rate. There was no significant difference in age, pathology, postoperative follow-up time, anatomy data of sphenoid, and other data.
Conclusions and Significance:
The modified endoscopic sphenoidotomy may reduce the rate of postoperative sinus ostium atresia.
Keywords
Introduction
Isolated sphenoid sinus disease is a rare disease, often manifesting as varying degrees of pain in different parts of the head. Some patients are asymptomatic and are only diagnosed by sphenoid sinus mass seen during CT or MRI examinations. 1 Because of the deep location of the sphenoid sinus and nonspecific symptoms, the diagnosis and treatment of isolated sphenoid sinus disease is often delayed, and severe cases can lead to vision loss.2,3 Moss et al. retrospectively analyzed 1133 patients with isolated sphenoid sinus disease reported in the literature. The pathology was chronic rhinosinusitis without nasal polyps (CRSsNP) (28.3%), mucocele (20.3%), fungal sinusitis (12.5%), intracranial lesions (7.0%), benign tumors (5.7%), and malignant tumors (7.7%). 4 There are many benign lesions in isolated sphenoid sinus disease, but a considerable part of them are malignant tumors, which require early surgical treatment. 5
The most common surgical method for isolated sphenoid sinus disease is endoscopic sphenoidotomy. The key step is to find the natural sphenoid sinus ostium through the ethmoid sinus or olfactory cleft, expand the sphenoid sinus ostium and clear the lesion. The size of the expanded sinus ostium is determined according to the pathology and volume of the lesion. 17.2% of the septal branch of the sphenopalatine artery was injured during endoscopic sphenoidotomy, electrocoagulation is required to stop bleeding.6–8 After sphenoid sinus surgery, 9.4%–10.2% of patients develop sphenoid ostium atresia, resulting in sphenoid sinus mucocele.9,10
The main cause of sinus stenosis and atresia after sphenoidotomy is surgical wound scar hyperplasia, and the secondary cause is inflammatory bone hyperplasia. According to statistical analysis, the diameter of the ostium will be reduced by 43% in one month after sphenoid sinus opening, and the ostium will be stable after 6 months, the ostium area needs to be expanded to more than 61.3 mm2 in order to avoid ostium stenosis and atresia. 11 However, in our clinical experience, some patients had sinus ostium atresia after surgery even after we opened the sphenoid sinus to more than 100 mm2 . We believe that simply expanding the ostium diameter is insufficient to avoid sinus ostium atresia, and new methods are needed.
To reduce sphenoid sinus ostium atresia rate after sphenoidotomy for isolated sphenoid sinus disease, we reviewed the data of patients with isolated sphenoid sinus disease at our department in the past 7 years. Before 2020, the traditional sphenoidotomy was used to expand the natural ostium inward and downward under the nasal endoscope. After 2020, the modified sphenoidotomy was recommended by Harvey et al. to expand the sphenoid sinus ostium upward and outward under the nasal endoscope. 12 We compared the clinical characters and sinus ostium stenosis rate of two groups in this study.
Materials and methods
Study design and patients
Between January 2015 and April 2022, the data of patients with isolated sphenoid sinus lesions admitted to the Department of Otolaryngology, the Second Affiliated Hospital of Zhejiang University School of Medicine were retrospectively analyzed, and the CT images of all patients were reviewed to confirm that the lesions were confined to the sphenoid sinus. Patients with lesions beyond the sphenoid sinus, non-nasal headaches such as migraine and tension headaches, or those who did not undergo surgery were excluded. This study was approved by the hospital ethics committee, and all patients gave informed consent.
Before 2020, the patients underwent traditional endoscopic sphenoidotomy (exposing the natural sphenoid sinus ostium through the olfactory cleft or ethmoid sinus, enlarging the sphenoid sinus ostium inward and downward, and coagulating the septal branch of the sphenopalatine artery), and the diameter of the opening window was greater than 10 mm. After January 2020, the patients underwent modified endoscopic sphenoid sinus surgery (enlarging the sphenoid sinus ostium upward and outward, reaching the base of the skull and the lamina papyracea. If the window was insufficient to clear the lesion, a small amount of tissue below the sphenoid sinus natural ostium was removed, leaving the septal branch of the sphenopalatine artery and the inner mucosa of the sphenoid sinus ostium intact). Nasopore or high-expansion sponge was used to fill the surgical cavity in both methods, and the high-expansion sponge was pumped on the second day after the surgery. The patients were re-examined at 2, 6 weeks, and 12 weeks after surgery with endoscopy. If the sphenoid sinus ostium was susceptible to stenosis, follow-up was continued until the size of the sinus ostium was stable. All patients were telephonically followed-up 1 year after surgery. If the patient has symptoms such as headache, we advise the patient to revisit the hospital for nasal endoscopy. All surgeries were performed by three rhinologists with more than 10 years of surgical experience. The clinical data of patients were collected, including age, gender, chief complaint, disease course, CT and/or MRI images, surgical methods, complications, and whether or not underwent re-operation.
The anatomical data of the anterior wall of sphenoid sinus in two groups were measured. The axial CT bone window was used to measure the distance from the natural ostium of the sphenoid sinus to the sphenoid sinus septum, the distance from the natural ostium of the sphenoid sinus to the ethmoid bone lamina papyracea, and the thickness of the sphenoid sinus wall. The sagittal CT bone window was used to measure the distance from the natural ostium of the sphenoid sinus to the skull base, the distance from the natural ostium of the sphenoid sinus to the bottom wall, and the thickness of the sphenoid sinus wall (Figure 1). The anatomical data of the anterior wall of the sphenoid sinus was compared between the traditional surgery group and the modified surgery group.
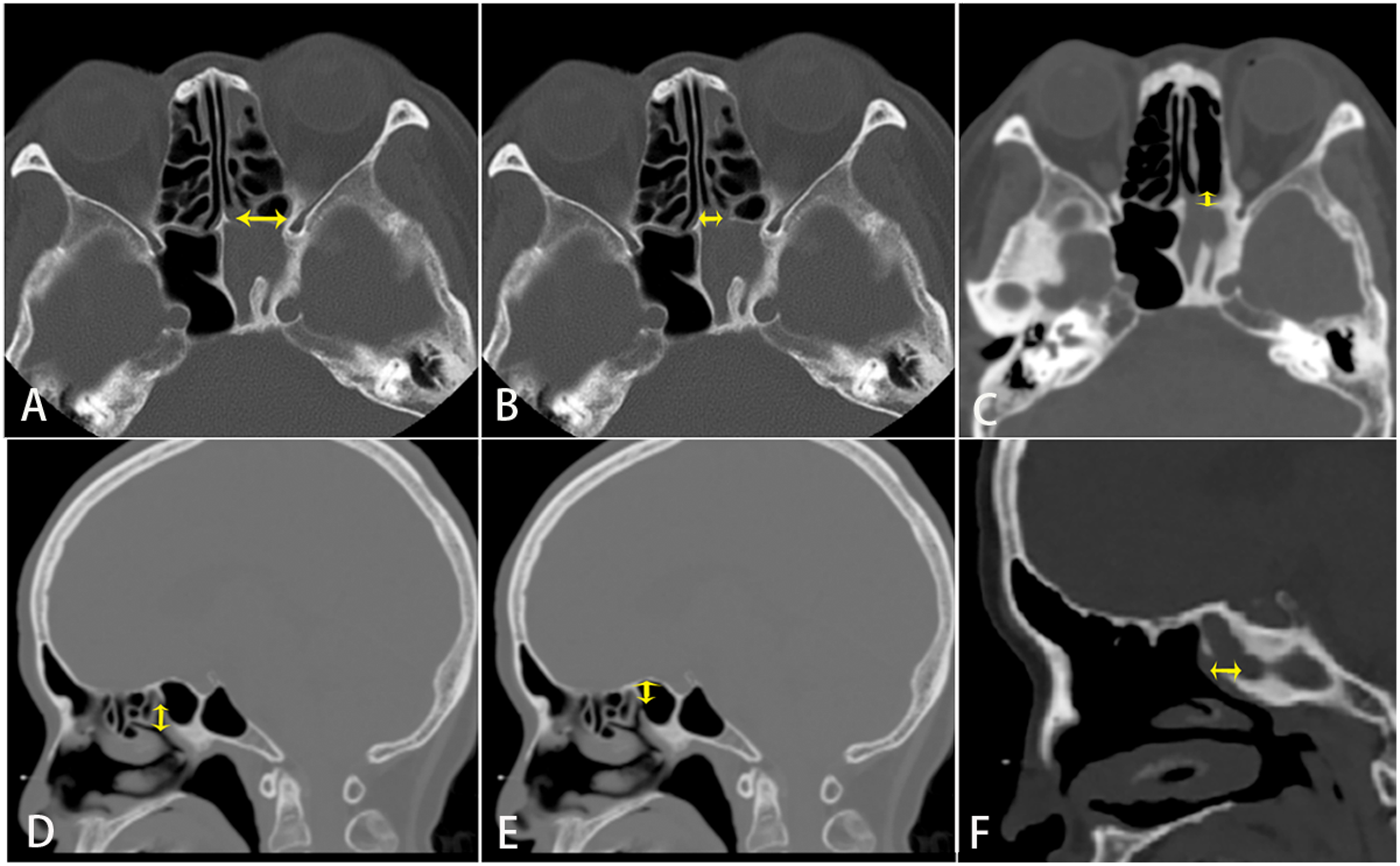
The axial CT bone window was used to measure the distance from the sphenoid sinus natural ostium to the sphenoid septum, the distance from the natural ostium to the paper template, and the thickness of the sphenoid sinus wall. The sagittal CT bone window was used to measure the distance from the natural ostium to the skull base, the natural ostium to the bottom wall of the sphenoid sinus, and the thickness of the sphenoid sinus wall.
Group sample sizes of 41 in group 1 and 76 in group 2 achieve 94.8% power to detect a significant difference with a two-sided type 1 error of 5% between the incidence of the primary endpoint of 0% and 14.5% in group 1 and group 2.
SPSS 22.0 software was used for statistical analysis. The patients were divided into two surgical treatment groups. Numerical variables with normal distribution were expressed as mean ± standard deviation, and analysis of variance was used for the comparisons. Categorical variables were described using the R × C contingency table, and Fisher exact probability tests were used for statistical analysis. The level of the statistical test was set to 0.5.
In this study, the re-surgery rate in the modified surgery group is assumed to be 0%, and the re-surgery rate in the routine surgery group is 14.5%. Type I error α = 0.05 and Type II error β = 0.2 of the hypothesis test was set, and the sample size ratio of the modified surgery group and the routine surgery group was 1: 1.86. According to the calculation formula, sample sizes of 41 in the modified surgery group and 76 in the routine surgery group achieve 94.8% power to detect a significant difference with a two-sided type 1 error of 5%.
Results
A total of 117 patients were included in this study, 39 males and 78 females, with a male-to-female ratio of 1:2, average age of 47.1 years (range 8–77 years). The mean disease duration was 21.5 months (1–120 months), the mean follow-up time was 23.4 months (range 6–83 months). Headache was the most common clinical manifestation, followed by nasal symptoms, and few patients had cranial nerve symptoms or no symptoms (Table 1). Pathological analysis: fungal balls were predominant, followed by mucosal cysts and bacterial sphenoid sinusitis, while fibrous bone dysplasia, cerebrospinal fluid leakage, and hemorrhagic necrotizing polyps were rare (Figure 2).

Pathological composition of isolated sphenoid sinus disease.
Symptoms.

There were 76 cases of traditional surgery and 41 cases of modified surgery. There were no statistical differences in age, sex ratio, proportion of major disease types, duration of disease, and follow-up duration, between the two groups. There were significant differences in the sinus ostium atresia rate (Table 2). There were 11 patients with ostium atresia in the traditional surgery group and no ostium atresia in the modified surgery group, suggesting that the recurrence rate was significantly different after the two surgical methods. Eleven patients with ostium atresia were cured by enlarged sphenoid sinus surgery (opening of bilateral sphenoid sinuses, removal of sphenoid sinus septum, and septal flap covering the wound), and no recurrence was found in the follow-up for more than 1 year (Figure 3).

A: The right sphenoid sinus was traditionally opened downward and inward, with a diameter of about 1 cm, and the wounds on the inner wall and bottom wall were larger. B: The left sphenoid sinus was enlarged upward and outward, and the mucosa of the inner and lower sphenoid ostium was preserved. The diameter of the sphenoid sinus was about 1 cm. C: In a patient with atresia of the sphenoid ostium, the sphenoid septum was surgically removed again, so that the bilateral sphenoid sinuses were penetrated and the septal flap covered the wound. D: Atresia of the sphenoid sinus was found five months after the traditionally sphenoidotomy. E: The sphenoid sinus ostium was not significantly reduced at three months after modified sphenoidotomy, and the adhesion zone was seen. F: In three months after bilateral sphenoid sinuses, the sphenoid sinus ostium did not reduced, and the drainage was smooth.
Characteristics of the routine surgery and modified surgery groups.

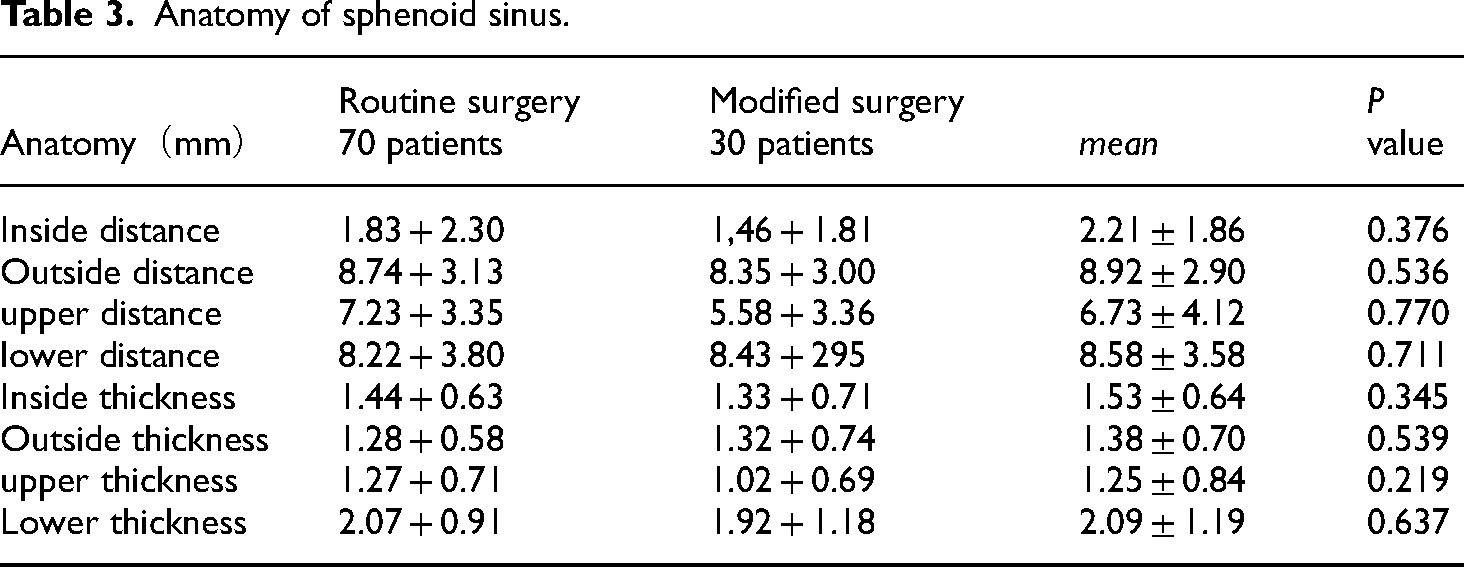
CT measurements showed a total of 200 sphenoid sinuses in 100 adult patients of two groups. The natural ostium was the farthest from the lateral wall of the sphenoid sinus, followed by the bottom wall and the base of the skull, and nearest to the septum. The thickest bone wall around the sphenoid sinus ostium was the bottom wall, followed by the medial wall, while the outer wall and the upper wall were the thinnest. There were no significant differences in anatomical data between the conventional surgery group and the modified surgery group (Table 3). Sphenoid sinus development in children is age-dependent, and Japanese children reach their greatest size and volume at the age of 15 years. 13 This study had only one pediatric patient, and the anatomical measurements were all adults, which may not apply to children with sphenoid sinus disease.
Anatomy of sphenoid sinus.
Discussion
The proportion of patients with headaches in this study was 71%, and the locations of headaches included the occiput, back of the orbit, the forehead, and other parts, nasal symptoms accounted for only 31%, which was consistent with previous studies. Given the lack of specificity in headaches, many patients in this study were admitted to the Department of Neurology, and were transferred to our department after drug treatment proved ineffective, headache worsened or vision loss occurred. Therefore, it is necessary to increase communication between different departments. Except for acute sphenoid sinusitis, sphenoid sinus disease typically exhibits longer and less severe headaches and occasionally concurrent ocular symptoms such as decreased vision, diplopia, and ptosis, which suggests that the lesion invaded the peripheral nerves of the sphenoid sinus, and the CT or MRI display sphenoid sinus lesions, which was different from nervous headache.
The pathological composition of isolated sphenoid sinus disease varied greatly in different regions. According to statistics in published studies, inflammatory diseases accounted for 75%, tumors accounted for 18.9%, and malignant tumors accounted for less than 7%. 14 This study showed that fungal sphenoid sinus was the most common in Zhejiang Province, China, and the proportion of all fungal sinusitis was 63.6%, which was much higher than that in other countries, and even higher than that in Henan Province, China,4,15 but was similar to the disease composition in Taiwan, China, 16 and may be related to the similar warm and humid climates in Zhejiang and Taiwan.
Isolated sphenoid lesions usually require surgery. Traditional sphenoidotomy is recommended to expand the natural ostium of the sphenoid sinus from the olfactory cleft or the posterior ethmoid sinus, but the window expansion direction is not recommended. Most surgeons prefer to expand the sphenoid sinus downward and inward based on the convenience of transnasal surgery, and tend to avoid the dangerous area of the skull base and lateral wall of the sphenoid sinus. This surgical method is easy and has a low risk. The patient can be operated through the olfactory cleft, but the septal branch of the sphenopalatine artery must be blocked. Meanwhile, the bone at the medial and bottom wall of the sphenoid sinus ostium is exposed, which is susceptible to scarring. Sphenoid sinus inflammatory disease is usually accompanied by mucosal and bone inflammation, more severe scarring, and even bone hyperplasia.
Our measurements data of sphenoid sinus showed that the natural ostium of the sphenoid sinus was farther from the skull base, the lamina papyracea, and the bottom wall of the sphenoid sinus, and very close to the sphenoid sinus septum. The anterior wall of the sphenoid sinus above and outside the sphenoid ostium was thin, while the anterior wall below and medial was thicker. Inward expansion of the sphenoid sinus ostium offered very limited operating space, and it was easy to expose a large area of bone, which may lead to postoperative scar hyperplasia. Expanding the sphenoid sinus ostium downward could offer a larger operating space, but the bottom wall of the sphenoid sinus is thicker than anterior wall; downward expansion leads to larger exposed bone surface. The septal branch of the sphenopalatine artery passes through the middle of the sphenoid sinus ostium and the bottom wall of the sphenoid sinus, and downward expansion will easily damage the sphenopalatine artery. Electrocoagulation must be used to stop the bleeding, which will cause larger wounds and increase the risk of sphenoid stenosis. 8 These factors may explain the need for re-operation in some patients with sphenoid atresia after traditional sphenoid surgery.
We found that opening the sphenoid sinus from the natural ostium of the sphenoid sinus to the base of the skull outward to the lamina papyracea offered a larger operating space (above 10 × 10 mm2), and the use of the angle endoscope combined with the flexible suction device could clear the fungus and pus in the sphenoid sinus easy. The surface of residual bone wound is very thin, and rapid healing of the mucosa can maximally prevent the sinus atresia caused by scar hyperplasia. If the sphenoid sinus ostium is located on the upper side, patients with excellent sphenoid sinus gasification may be unable to clear the lesion. They can bite down to remove part of the anterior wall of the sphenoid sinus, which should not exceed the septum of the sphenopalatine artery, in order to avoid scar hyperplasia caused by electrocoagulation and exposed bone of the bottom wall. In this study, there was no atresia in 31 patients with this treatment, which was significantly better than traditional sphenoidotomy. There was no difference between the two groups in terms of disease composition and anatomical data of the anterior wall of the sphenoid sinus, indicating that the surgical method is the key factor for atresia of the sphenoid sinus ostium.
Follow-up after sphenoidotomy is critical. The blood scab and fibrin in the sphenoid ostium should be cleaned within 2 weeks after surgery, and the sphenoid ostium should be regularly observed by endoscopy. We found that if the sphenoid sinus ostium was significantly reduced in diameter by less than 3 mm, there was a greater chance of atresia. Direct ethmoid forceps can be used to expand the sphenoid ostium while maintaining the integrity of the surrounding mucosa. If necessary, a stent with sustained-release glucocorticoids can also be placed after the expansion to reduce the chance of atresia. One patient with fungal sphenoids found a stenosis of the sphenoid sinus orifice after surgery. A sustained-release glucocorticoids stent was placed one month after surgery, removed 26 days later, and the sphenoid sinus orifice was reduced but remained unobstructed 2 years after surgery. However, intraoperative wound minimization and mucosal integrity remain the top priority. We found that the reduction degree of modified sphenoidotomy is significantly less than that of traditional surgery, and expansion is rarely required.
For sphenoid mucoceles caused by atresia of the sphenoid ostium, Thompson CF advocated the use of a modified nasal septum flap to cover the exposed bone behind the sphenoid ostium to accelerate healing and prevent atresia. 17 Leight et al. advocated sphenoid “drill-out” for recurrent sphenoid sinusitis. Endoscopic resection of the sphenoid sinus septum to allow bilateral sphenoid sinus penetration can effectively relieve recurrent sphenoid sinus headache. 18 Donald PJ recommended a more radical sphenoid sinusostomy, in which the anterior wall, septum, and bottom wall of bilateral sphenoid sinuses were removed to achieve complete fusion between bilateral sphenoid sinuses and nasopharynx. 19 We typically used the surgical method reported by Leight, and simultaneously transferred bilateral septal mucosal flaps to cover the surgical wound. The operation mode similar to frontal sinus Draf III surgery can maximize the diameter of the sphenoid sinus fenestrum, which helps postoperative follow-up, and mucosal covering on the wound surface can reduce scar hyperplasia.
Conclusion
CT measurement showed that the anterior wall of the sphenoid sinus had sufficient space on the lateral and upper sides of the natural ostium, and the bone was thin, which was suitable for expansion of the sphenoid sinus. Compared with the traditional inward–downward sphenoidotomy, the modified nasal endoscopic upward-outward sphenoidotomy is less invasive and may have a lower chance of sinus atresia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Medical and Health Research Program grant of Zhejiang Province supports this work (Grant no. 2020KY145).
Author biographies
Hong-Gang Duan holds a PhD in Otolaryngology. His area of research is rhinology.
Fang Ji holds an MD in Neurology. Her area of research is electromyography.
Hui Yuan holds a PhD in Otolaryngology. His area of research is rhinology.
Hua-Lin Wang holds an MD in Otolaryngology. His area of research is rhinology.
Ming Chen holds a PhD in Otolaryngology. His area of research is rhinology and laryngology.
Di-Jiang Ma holds a MD in Otolaryngology. His area of research is rhinology, laryngology, and Otology.