
Abstract
COVID-19 is a sudden, infectious disease that can be life-threatening and may cause people to feel panic and anxiety. This study aimed to investigate the clinical characteristics and psychological status of a specific population using an internet consultation platform during the outbreak of COVID-19. The questionnaire survey included questions regarding basic information (e.g. area, sex, age, occupation, and education level), clinical characteristics, and cognitive and psychological status concerning COVID-19 from January 31, 2020 to March 31, 2020. There were 277 patients (43.49%) with three or more symptoms, 121 (12.11%) with a clinical questionnaire score ≥8, and 6.81% who lived in Hubei in the previous 14 days. Of the respondents, 4.9% had contact fever or were confirmed to have COVID-19 in the previous 14 days. The respondents were mostly aware that COVID-19 can be transmitted from person to person and via the respiratory tract, but awareness of general susceptibility and specific symptoms of COVID-19 was low. Multivariate analysis showed that urban residents, clerk/students and higher education groups were well aware of COVID-19. Regarding mental health, the anxiety score of the respondents was 7.12 ± 2.32, and the proportion of anxiety was 54.15%. Younger women were more likely to have anxiety when they experienced positive symptoms. Individuals with a Hubei residence history and those who had contact with an individual with a fever or were confirmed patients in the previous 14 days were more likely to have moderate or severe anxiety. The COVID-19-related knowledge of the respondents was generally good but still could have been improved. Their psychological status was also affected by the pandemic. The internet consultation platform played a positive role in spreading pandemic-related information, providing medical help and psychological counseling, and strengthening early warning to the potential high-risk population.
Introduction
In recent years, outbreaks of infectious diseases have often become public health issues of widespread concern in the international community, such as the SARS pandemic in China in 2003, 1 the Middle East Respiratory Syndrome (MERS) pandemic in 2012, 2 and the outbreak of Ebola disease in West Africa in 2014. 3 These outbreaks caused great losses in the lives and property of people worldwide, and they also caused serious psychological trauma. Studies have pointed out that the physical damage caused by these sudden public health incidents may recover in a short time, but the psychological impact will last for a long time. 4 After the SARS outbreak in China in 2003, many patients developed acute stress disorder and posttraumatic stress disorder. Therefore, it is necessary to implement a psychological crisis intervention in the public as quickly as possible. 5
In December 2019, several unexplained pneumonia cases were reported in Wuhan (Hubei, China). Subsequent studies showed that the disease was related to a new coronavirus infection. The World Health Organization (WHO) announced that the new coronavirus infection pandemic was designated as a public health emergency of international concern on January 30, 2020, and named the new coronavirus pneumonia “COVID-19” on February 21, 2020, at the same time that the International Classification Committee of the virus named the new coronavirus “SARS-CoV-2.” 6
COVID-19 is a sudden, infectious disease, and due to a lack of specific drugs, if not treated in a timely manner, it can be life-threatening. 7 In addition, the large amount of information concerning the pandemic has had a significant impact on public mental health, causing people to feel panic, anxiety, worry and even depression, especially among the elderly, psychiatric patients, patients with chronic diseases, workers, healthcare workers, and villagers.8–13 To block the spread of the COVID-19 pandemic, China requested some factories to shut down, schools to suspend classes, and restaurants to close during the pandemic. Many shops were forced to suspend business, and the number of people who reduced outdoor activities and holidays increased. Due to the long-term home stay, individuals could not work properly or participate in learning and social activities, which indirectly aggravated their anxiety, especially those with positive symptoms. Because of the limited medical resources and fear of cross-infection in hospitals, some people chose to use an internet consultation platform for health consultation and treatment, as well as to alleviate their anxiety and receive clinical treatment recommendations. The current research on COVID-19 primarily focuses on epidemiological and clinical studies. There are few studies on the cognitive and mental health of the population. This study was conducted to explore the clinical characteristics of the questionnaire group and the cognitive and psychological status of COVID-19 patients through a cross-sectional survey, with the aim of providing treatment information for public health departments and clinicians.
Methods
Participants
Internet questionnaires in this study were distributed throughout 470 cities or counties in China from January 31, 2020 to March 31, 2020. The inclusion criteria were as follows: (1) patients who buy consultation services for free on the internet consultation platform using the subject word “COVID-19-related consultation;” (2) age greater than 16 years; and (3) volunteered to participate in the survey. The exclusion criteria were as follows: (1) age less than 16 years; (2) respondents who were reluctant to participate in the survey due to fear of revealing their privacy; and (3) network consultation patients who could not be contacted using existing contact information. Of the 1100 respondents who completed the questionnaire, 101 non-conforming questionnaires were excluded, yielding a total number of valid questionnaires of 999 (90.82%). All participants provided informed consent.
Measure
We used two electronic questionnaires, namely, the “clinical characteristics questionnaire” and “cognitive questionnaire.” 14 The electronic questionnaires were issued through the “internet consultation platform” or “QQ and WeChat.” All the work was completed by two clinicians and two nurses, and the electronic questionnaires were required to be completed online during an internet interrogation. The clinical characteristics questionnaire included the following: fever (T > 37.3°C), cough, headache, nasal congestion, runny nose, dyspnea, diarrhea, sore throat, and fatigue. Symptom duration was divided into 1–3, 4–7, 8–14, and 14+ d groups. Respondents were asked whether they had a history of residence or travel in Hubei in the previous 14 days and whether the respondents had fever or respiratory symptoms or contact with confirmed cases in the previous 14 days. The total score of the clinical feature questionnaire was 10 points, and those who scored more than eight were considered high-risk patients. The cognitive questionnaire included the following: general demographic characteristics (e.g. area, sex, age, occupation, and education level); COVID-19-related knowledge (main symptoms, transmission route, susceptible population, and protection knowledge); personal prevention; and control behavior (e.g. wearing masks, proper hand hygiene, reduction of interpersonal contact, proper medical treatment). The questionnaire contained eight questions on COVID-19-related knowledge. A correct answer scored one point, and an incorrect answer scored 0 points. The scores of all the questions were combined to obtain a total score for the category. Based on these answers, out of a total score of 8 points, a score of <6 was considered poorly informed and ≥6 was considered well-informed. The study protocol (NO. JD-HG-2020-11) was approved by the Clinical Research Ethics Committee of The Second Affiliated Hospital of Soochow University.
The generalized anxiety disorder 7 (GAD-7) scale
This scale is a quantitative evaluation standard recommended by the American Psychiatric Association, published in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders. It is an effective tool with which to identify possible cases of generalized anxiety disorder 15 and has demonstrated good reliability and validity in previous studies. 16 According to the grading standard, the GAD-7 score is divided into four groups: 0–5, 6–9, 10–14, and 15–21, corresponding to no, mild, moderate, and severe anxiety, respectively. 17
Statistical analysis
SPSS 25 software (MAC) was used to collate, describe and analyze the data. The results are expressed as the mean ± standard deviation (SD). A chi-square test was used to compare the differences in the rates of different characteristics of the respondents. Multivariate analysis was conducted using a disordered multi-category logistic regression analysis. Two-sided p-values < 0.05 were considered to indicate a statistically significant difference.
Results
Demographics of the respondents
The ages of the respondents ranged from 16 to 63 years old, with an average age of 33.24 ± 6.32. Men accounted for 51.5% (514) of the respondents. Urban and rural areas accounted for 59.36% (593) and 40.64% (406), respectively. The most common occupations were students and clerks, accounting for 67.47% (674), and more than half of the respondents had a higher education, accounting for 51.25% (512), as showed in Table 1.
Demographics of the respondents (N = 999).

Urban versus rural p < 0.05.
Clerks/students versus Unemployed p < 0.01.
Clinical characteristics of the respondents
A total of 637 (63.76%) of the 999 respondents had positive symptoms when they consulted the internet consultation platform, and 362 (36.24%) were asymptomatic consultants. The main consultation questions concerned the transmission of the new coronavirus, routes of infection, incubation period, and degree of hazard. Among the respondents, the most common symptom was fever, accounting for 57.46%, and most of these patients had a low fever, with patients with temperatures of 37.3°C–37.6°C accounting for 84.55% of the respondents. The incidences of positive symptoms were ranked as follows: runny nose (53.69%) > nasal congestion (40.19%) > cough (38.76%) > sore throat (33.12%) > fatigue (27.47%) > dyspnea (26.22%) > headache (24.49%) > diarrhea (15.86%). A total of 277 (43.49%) patients reported three or more symptoms. There were 121 (12.11%) patients who scored more than eight on the clinical questionnaire and were considered to be at high risk for COVID-19. The patients with positive symptoms most commonly reported a 1-3-d course (33.44%), followed by a 14+-d course (31.40%). Sixty-eight patients (6.81%) had a history of Hubei residence or travel in the previous 14 days, and 49 patients (4.9%) had been exposed to individuals with a fever and respiratory symptoms or been in contact with confirmed patients in the previous 14 days (Table 2).
The clinical characteristics of the respondents (N = 999).

Hubei contact: whether respondents had a history of residence or travel in Hubei in the previous 14 days; Patients contact: whether respondents had contact with fever or respiratory symptoms or confirmed cases in the previous 14 days.
Understanding of COVID-19-related knowledge
Respondents were most aware that COVID-19 can be transmitted from person to person and via the respiratory tract. The percentage of respondents who knew that asymptomatic infected persons are contagious was relatively low. More than two-thirds of the respondents knew that close contacts needed to be quarantined for 14 days. However, the awareness of general susceptibility and specific symptoms of COVID-19 was low. More than half of the respondents believed that bats may carry the virus. Most of the respondents knew that disposable medical masks, medical surgical masks, and N95 respirators can effectively prevent COVID-19 and understood the correct protection time of masks. However, most respondents did not know that 75% alcohol, high temperature (56°C for 30 min) and chlorine disinfectant (84 disinfectant) can kill the virus (Table 3).
Understanding of COVID-19-related knowledge.

Knowledge level of respondents with different demographics
The average knowledge score regarding COVID-19 of all respondents was 6.11 ± 1.98. Among them, 723 (72.37%) scored more than 6 points. The difference in knowledge of COVID-19 with respect to different places of residence, occupations and education levels was statistically significant (p < 0.05; Table 4). The population characteristics with statistical significance in Table 4 were incorporated into the multivariate logistic regression model. Using knowledge as the dependent variable, sex, age, occupation, residence, and educational level were used as independent variables, and multivariate logistic regression analysis was then performed. The results showed that urban residents, clerk/students and higher education groups were well aware of COVID-19 (Table 5).
Knowledge of COVID-19 among populations with different demographics.

The total possible knowledge score was 8 points, <6 points was considered to be Poorly informed, ≥6 points was considered to be Well-informed.
Comparisons between different demographics.

Psychological state of the respondents during the pandemic period
The average anxiety score of the respondents was 7.12 ± 2.32. A total of 541 (54.15%) respondents had anxiety. The numbers of respondents with mild, moderate, and severe anxiety were 312 (57.67%), 141 (26.06%) and 88 (16.27%), respectively. The 88 patients with severe anxiety all reported positive clinical symptoms, and among them, 86 respondents had a clinical feature score greater than eight (high risk for COVID-19). The patients with fever had higher anxiety scores (9.04±0.96). Anxiety was present in 269 (73.50%) of the 366 fever patients. There were 277 patients with more than three positive symptoms, 188 (67.87%) of whom showed varying degrees of anxiety. A total of 458 (45.85%) respondents reported no anxiety, most of whom did not have positive symptoms but were looking for a health information consultation on the network platform or reported only one positive symptom.
Using “no anxiety” as the reference group, younger females and those with positive symptoms were more likely to have mild anxiety. The OR (95% CI) values were 0.90 (0.86, 0.99), 1.28 (1.06, 1.55), and 1.45 (1.16,1.81). Respondents with positive clinical symptoms were prone to mild anxiety at the early stage of the disease. Moderate anxiety was likely to develop after 14 d, with OR (95% CI) values of 9.55 (1.26, 69.15), 8.03 (1.96, 32.75), and 9.50 (1.26, 71.49). Respondents with a history of residence (or travel) in Hubei province in the previous 14 days and a history of exposure to fever with respiratory symptoms (or contact with confirmed patients) in the previous 14 days were prone to moderate to severe anxiety, with OR (95% CI) values of 1.73 (1.06, 2.95) and 0.85 (0.76, 1.01), respectively (Table 6).
Logistic regression analysis of anxiety severity of respondents.
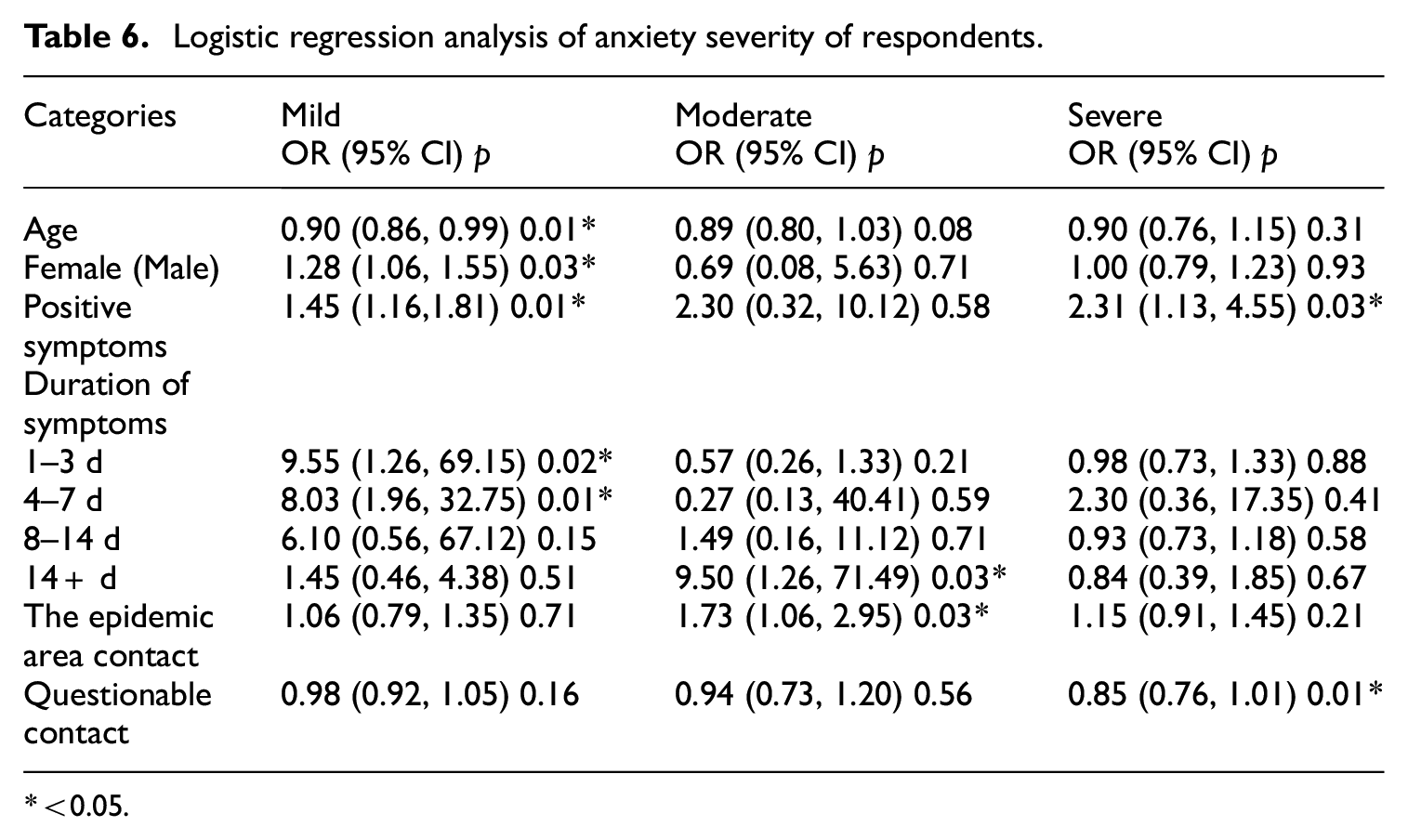
<0.05.
Follow-up
From May 1, 2020 to June 10, 2020, 121 patients with a clinical questionnaire score greater than eight were followed up online (e.g. internet consultation platform, Telephone, WeChat), and 89 (73.55%) responded. The results showed that eight of them tested positive for COVID-19 antibodies or throat swabs at the hospital following the internet consultation. COVID-19 was diagnosed based on these results combined with chest CT findings, and all eight patients recovered completely after treatment. The other 81 patients had a normal respiratory tract infection or intestinal infection and were cured through timely and effective treatment.
Discussion
China’s pandemic started in Wuhan (Hubei province) but soon spread to all parts of the country. The outbreak of COVID-19 has had a direct or indirect impact on all aspects of society. 18 However, with the joint efforts of the government, health departments, and organizations at all levels, the pandemic situation in China has been well-controlled. 19 During this period, all of society made adjustments, and as public and designated hospitals became filled with COVID-19 and fever patients, which resulted in a shortage of medical resources, the Chinese Government recommended and encouraged people to consult with medical care providers online if they could not get to the hospital in time, if they had mild symptoms or for various other reasons. An online medical consultation platform can be used to consult qualified doctors online and receive a timely response. During the pandemic period, all internet, virus-related consultations conducted via mobile phones or computers were free of charge. Therefore, a large number of patients chose to consult COVID-19-related questions on the internet platform.
In this study, the clinical characteristics of the internet consultation patients were analyzed, and their knowledge of COVID-19 and psychological response to the pandemic were investigated. The study showed that the most common symptoms were fever, mainly low fever, and most of the other symptoms were respiratory symptoms, in accordance with the symptoms of COVID-19. In the survey, we found that there were 277 patients (43.49%) who had three or more symptoms, and there were 121 (12.11%) respondents with a clinical questionnaire score of eight or above. These respondents were high-risk patients who required additional attention. We followed them up closely, and we also actively advised these patients to undergo COVID-19 nucleic acid tests and chest CT scans in local hospitals to rule out positive infections. Our work has also been supported by government departments. In subsequent studies, we found that the respondents’ knowledge of COVID-19 was generally good, but the spread of the pandemic and the combination of positive symptoms have also caused some psychological burden on the respondents. Internet consultation patients are a small percentage of the Chinese population. Additionally, although this segment of the population resided in 470 regions in China, they are not fully representative of the disease and psychological characteristics of the entire population. Through investigation of their knowledge, disease characteristics and psychological status, we can obtain a better understanding of the general characteristics of the public in a particular population during the outbreak, and the study also provides a basis for health authorities to indirectly understand the mental state and characteristics of all residents. It is highly effective to encourage residents to take active personal prevention and control measures to improve their psychological status. Furthermore, the results of this study will provide a scientific basis for further targeted prevention and control strategies, measures and health education.
Raising awareness of COVID-19 can help people cope with the pandemic more effectively and scientifically.20–22 The results of this study showed that the average knowledge score regarding COVID-19 of all respondents was 6.11 ± 1.98, and 723 (72.37%) scored more than 6 points, suggesting that residents’ knowledge still needs to be improved. The respondents had a greater awareness of COVID-19 transmission channels and related protection knowledge, all of which were approximately 90% (98.60 and 89.99%, respectively). However, awareness of infectious and proper protective measures among asymptomatic infected individuals was relatively low at 32.83% and 38.74%, respectively. The awareness of general susceptibility and specific symptoms 23 of COVID-19 was low (31.23%). Since respondents generally did not fully understand COVID-19-related information, public health departments, and medical institutions should strengthen publicity and education on pandemic-related symptoms to enhance their knowledge of virus and self-protection awareness.
According to the analysis of the cognition of COVID-19 among people with different characteristics, the results showed that there were statistically significant differences in knowledge of COVID-19 among people with different places of residence, occupations, and educational backgrounds. In a further logistic analysis, we found that urban residents, clerks/students, and higher education groups were associated with being well-informed, possibly because urban residents are more concerned with information about the pandemic situation, and the clerks/students and higher education groups have more access to information. These individuals are also willing to obtain information about the pandemic through official authoritative channels and are also more capable of differentiating between true and false information. However, it is suggested that the related health education on COVID-19 in rural areas and in low educational level groups is important, and measures should be taken to promote good hygiene practices and raise awareness of the pandemic among this group.24,25 There were no significant differences in knowledge of COVID-19 among the different sex and age groups and groups with and without positive symptoms.
Previous emergency-related research revealed that a large number of people lack experience in coping with emergencies, lack emotional stability, lack analysis and decision-making ability and are more likely to be misled and act more impetuously. 26 To prevent the pandemic from escalating, colleges, and universities postponed school, factories shut down, businesses suspended operation, and residents reduced outings, which resulted in the inability of people to work, study and participate in social activities and may have affected their normal life and aggravated their anxiety. Therefore, the mental health problems of people cannot be ignored. 27 In this study, we surveyed 999 internet consultation patients, and the incidence of anxiety was 54.15%, which is higher than that of the general population. 4 It is apparent that the incidence of anxiety in the public is obviously increased under the stress of the COVID-19 pandemic, and it is urgent to adopt precise psychological intervention and health education measures.
Previous studies have shown that women were vulnerable to adverse mental health outcomes before COVID-19, 28 and our research shows that younger women and those with positive symptoms were more likely to have mild anxiety. This suggests that more attention should be paid to the mental health problems of young women and patients with positive symptoms. Women are more likely to have mild anxiety than men, so public health departments, women’s organizations, and psychological counseling centers should pay more attention to the psychological health of women and implement psychological intervention measures as early as possible. Further studies revealed that the respondents with positive clinical symptoms were prone to mild anxiety at the early stage of the disease, especially those with fever and those with three or more positive symptoms. These patients require more active psychological counseling and treatment. At the same time, with the extension of the disease course, especially after the course of disease exceeds 14 d, moderate anxiety is likely to develop. This may be because when positive symptoms are experienced in the early stage of the disease, the respondents are likely to be confused and unsure whether they may be infected by COVID-19. As time goes on and the patient’s symptoms persist, the respondents may start to experience panic. In addition, respondents with a history of residence (or travel) in Hubei province in the last 14 days and a history of exposure to fever with respiratory symptoms (or contact with confirmed patients) in the previous 14 days were prone to moderate to severe anxiety. The possible reason for this could be that respondents believe that people who come into contact with infected areas or confirmed cases are likely to become infected, resulting in moderate to severe anxiety in this part of the population. Medical institutions and internet consultation platform doctors should take the initiative to provide correct guidance to these patients, including explaining the typical symptoms of COVID-19, how to exclude COVID-19, whether to go to the hospital for a detailed examination, reasonable prevention strategies to avoid being infected and how to decrease anxiety, to promote the understanding of COVID-19-related knowledge more comprehensively, enhance the awareness of COVID-19 and reduce anxiety and panic. If we encounter patients with anxiety, fear or insomnia on the online consultation platform, we can cooperate with psychiatrists to implement psychosocial therapies to improve these symptoms, as psychosocial therapies, such as cognitive behavioral therapy (CBT), have been proven to be useful and efficacious for both psychiatric symptoms and insomnia not just before COVID-19 but also during the pandemic.29,30 At the same time, internet-based CBT therapy is also playing an increasingly important role and could be used instead as a cost effective method to implement and deliver such therapies. 31
All the respondents in the study completed a questionnaire through an internet consultation platform and through internet social networking tools (e.g. QQ, microblog, WeChat). In this manner, patients were able to communicate with qualified doctors without leaving their homes, reducing the risk of cross infection in hospital visits and reducing the waste of medical resources. This has been an effective part of the Chinese government’s pandemic prevention work, and it has played a certain role in reducing the cross infection as much as possible. Internet consultation and online social networking tools have the characteristics of high efficiency, convenience and rapid response times. They also help residents obtain timely information about COVID-19 during the pandemic. This suggests that relevant government departments and medical institutions can enhance public awareness of health education on pandemic prevention measures and COVID-19-related knowledge by means of social media, social software and other new media. 32 Finally, in the follow-up, we found that the high-risk patients with positive symptoms were confirmed to be infected with COVID-19 after visiting the hospital. These patients received timely diagnosis and treatment because of our correct and timely treatment options and recommendations, demonstrating the effectiveness and timeliness of the internet consultation platform for disease screening. In addition, the internet consultation platform played a certain early warning role for high-risk patients and has performed a complementary role within medical institutions.
The WHO announced that the global transmission risk and risk level of COVID-19 should be upgraded to “very high” 33 in February 2020 and then announced that COVID-19 had the characteristics of a “global pandemic” 34 in March 2020. Thus, the pandemic prevention and control work could not be taken lightly at this stage. We need to unite, and all of society should address this public health issue together. Internet survey tools were used to investigate the cognitive and psychological status of the patients on the internet consultation platform to provide evidence for pandemic prevention and control. However, there are some limitations of this study. Due to the causes of the pandemic, the survey is mainly based on network use rather than random sampling, which may cause certain underrepresentation of those who are not familiar with the network, and there may be underrepresentation of the entire population. A follow-up study will further expand the population sample size to obtain more complete information to enable people to correctly understand the COVID-19 information and enhance their self-protection awareness, as well as to guide them to adopt healthy behaviors 35 and help them to avoid the negative societal effects of COVID-19.
Limitations: (1) Due to the COVID-19 pandemic, participants were internet users, which reduced the generalizability of this study’s findings. To improve the generalizability of the results, external surveys need to be conducted in wider populations. (2) Given the small number of patients included in this study, there is a need to conduct further studies and obtain more complete information to make the results more convincing. (3) This study mainly used self-reported questionnaires to measure psychiatric symptoms and was not based on clinical diagnoses. The gold standard for establishing psychiatric diagnosis involved structured clinical interviews and functional neuroimaging.36,37
Footnotes
Author’s contributions
Han Ouyang and Jian Wen and Wenyong Gu contributed equally to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the National Natural Science Pre-Research Fund of the Second Affiliated Hospital of Soochow University (SDFEYGJ1702).