
Abstract
Background
Tetanus constitutes a significant cause of death in sub-Saharan Africa, with case fatality rates as high as 64%, 47%, and 43.1% reported in Nigeria, Uganda, and Tanzania, respectively. However, the knowledge gap on factors that influence tetanus mortality still exists in Cameroon.
Objective
To identify the factors that influence the mortality of tetanus patients in three regional hospitals in the North West and South West Regions of Cameroon.
Methodology
This was a 7-year retrospective case-series study. Socio-demographic and clinical data of tetanus cases admitted in Bamenda, Buea, and Limbe Regional Hospitals from January 2010 to March 2017 were collected and analysed.
Results
This study recorded 38 cases, but excluded five due to missing inpatient files. Of the 33 cases considered in this study, 27 (81.8%) were males. The mean age of the patients was 32 years. A tetanus mortality rate of 48.5% was recorded – thus, 16 tetanus-related deaths. Mortality was higher amongst patients with incubation periods less than 7 days; the onset of trismus and generalized spasms less than 8 days after exposure; the presence of autonomic dysfunction; the presence of respiratory dysfunction; application or introduction of local regimens, soil or animal waste at the portal of entry; delayed debridement greater than 2 days after onset of tetanus; and a severe clinical disease state.
Conclusion
This study, therefore, highlights the need to ensure universal vaccination coverage for high-risk populations; males, active population (20–40 years), and farmers. More still, this study emphasizes the need to improve access and utilisation of mechanical ventilation in severe tetanus cases.
Introduction
Tetanus is an acute and often fatal disease caused by a toxin known as tetanospasmin produced by the bacterium, Clostridium tetani. It is characterised by progressive generalized rigidity and skeletal muscle spasms. 1 The global estimated incidence is one million cases annually. 2 In the United States of America, tetanus cases declined by over 95% and tetanus-related deaths by about 99% since 1947. 3 The marked reduction in tetanus incidence and mortality rate in high-income countries is due to the widespread use of tetanus toxoid-containing vaccines, improved wound care, and the use of tetanus immunoglobulin (TIG) for post-exposure prophylaxis and management of tetanus cases. 4
Conversely, tetanus is a significant cause of death in sub-Saharan Africa, with a case fatality rate ranging from 26% to 64% in neighbouring Nigeria. 5 Values as high as 64%, 47%, and 43.1%, have been reported in Nigeria, Uganda, and Tanzania. 6 The outcome is usually poor without a standard intensive care unit to manage tetanus complications such as airway obstruction, respiratory failure, and renal failure. 7 Moreover, autonomic instability and more recently, high urinary excretion of several catecholamines has been associated with poorer prognosis in patients with tetanus. 8 In a nutshell, the limited availability of intensive care facilities, the poor socio-economic status of patients, and poor vaccination coverage can explain the high tetanus-related mortality rates in sub-Saharan Africa. However, there are other modifiable and non-modifiable factors such as the patient's age, the incubation period, prior history of tetanus vaccination, tetanus severity, complications, and delays in treatment that may influence the mortality of tetanus patients.7,9,10 Currently, there are no studies in Cameroon that determines factors associated with tetanus mortality; hence the need to conduct this study to close the knowledge gap, and inform clinical and public health policies to reduce tetanus mortality.
Methodology
The study was a seven-year retrospective case series of tetanus cases admitted in the three regional hospitals (Bamenda, Buea, and Limbe Regional hospitals) in the Northwest and Southwest Regions of Cameroon from January 2010 to March 2017. Bamenda Regional Hospital is a state-owned referral hospital in an urban setting, Bamenda (the capital of Northwest Region) with medical specialists in surgery, internal medicine, paediatrics, obstetrics, and gynaecology. It is equipped with an intensive care unit and Isolation wards for the management of severe cases such as tetanus. It has about 400 admission beds and a yearly admission rate of over 5000 patients. Buea Regional Hospital is one of the referral centres in the Southwest Region of Cameroon. They have medical specialists in the field of surgery, paediatrics, obstetrics and gynaecology, and internal medicine. They have isolation wards but no intensive care unit. It has about 111 admission beds and admits over 3000 patients annually. Limbe Regional hospital is found in an urban setting. It is also a referral centre in the Southwest Region of Cameroon with medical specialists in the field of surgery, paediatrics, obstetrics and gynaecology, and internal medicine. During the study period, there was no intensive care unit. There are about 108 admission beds in the hospital with an annual admission rate of over 2500 patients. All patients presenting with trismus, neck or abdominal muscle rigidity, spontaneous or reflex spasm, or convulsions5,10 were included. Patients with other apparent medical causes of these symptoms and any missing inpatient files were excluded from the study. The choice of hospitals was based on convenience and the likelihood of finding cases since they are high-volume sites and referral centres. Metronidazole was the main antibiotic used during the study period. Penicillin has been associated with increased spasms since it potentiates the effect of tetanus toxin by inhibiting the type A (GABA A) receptor of gamma-amino-n- butyric acid. As such penicillin is not the antibiotic of choice.11,12 Spasms were managed solely using diazepam. This was because of its wider therapeutic index and lower incidence of side effects compared to magnesium sulfate, which is known to cause respiratory depression. Similarly, beta-blockers were seldom used because of their potential risk of symptomatic bradycardia which may require ICU care; not readily available in resource-limited settings.13,14
Using Ablett's classification of tetanus severity, we grouped patients into mild, moderate, severe, and very severe. To guide data collection, generalised tetanus was defined as trismus and generalized rigidity + /-generalized spasms. Localised tetanus was defined as rigidity and/or spasms limited to the wound area. Cephalic tetanus was defined as tetanus restricted to the head and neck (a form of localized type). Neonatal tetanus was defined as tetanus occurring between 0–28 days. Autonomic dysfunction was defined as a pulse rate of < 60 or >100 beats per minute and Blood pressure of < 90/60mmHg or >140/90 mmHg in patients not previously hypertensive.
Data were cleaned and analysed using Microsoft Excel 2007 and Statistical Package for Social Sciences (SPSS) version 20. This study was carried out after obtaining Faculty approval from the Dean of the Faculty of Health Sciences of the University of Buea; Administrative clearance from the Northwest and Southwest Regional Delegations; Ethical clearance from the Institutional Review Board; and approval from the different hospital management.
Results
The tetanus admission rate was estimated at 1 per 2500 admissions, with 86,000 patients admitted during this study period. Of the 33 cases included in the study, 27 (81.8%) were males. Their ages ranged from seven to 84 years with a mean age of 32.4 years (standard deviation (SD) ± 18.9). The most predominant age group was between 31 and 40 years (27%). The majority of patients were farmers (24.2%), followed by students (18.2%). There were two leading portals of entry: a wound (cuts, lacerations, ulcers, puncture wounds) seen in 31 (93.9%) patients and chronic ear infection found in two (6.1%) patients. The most common route of contamination was puncture wounds from metal objects, 11 (35.5%) as shown in Table 1. Of the 11 patients with puncture wounds, six (54.6%) were injured at a construction site. More than half of the patients had wounds on their lower limbs, 19 (57.6%).
Route of contamination.

ROC = Route of contamination; RTA = Road Traffic Accident.
Clinical presentation and management of these patients
In our study, the most common clinical type of tetanus was generalised tetanus, as seen in 29 (75.8%) patients. No case of neonatal tetanus was seen during our study period. However, two cases were less than ten years old with no history of childhood vaccination. There were three cephalic (9,1%) and one localised (3%) tetanus case. Information on the vaccination history of patients was available in 17 inpatient files (36.4%), all of whom were not vaccinated (0%). Of the 29 inpatient files (87.9%) that had information on the use of ATS as post-traumatic tetanus prophylaxis, only three patients (9%) had received ATS. In our study, ten patients (30%) presented with moderate tetanus severity (grade II) and ten (30%) others with severe tetanus (grade III) according to Ablett's classification of tetanus severity. Based on clinical severity, the outcome of patients was as in Table 2 below. All 33 (100%) patients were placed on ATS, Metronidazole, and Diazepam on admission. Of the 32 patients (96.7%) who had a wound, 22 (68.8%) underwent wound debridement. One patient was intubated (3%). Of the 14(42%) patients that survived, Just seven (50%) were vaccinated after recovery from the disease.
Distribution of patient outcome based on tetanus severity.

DAMA = Discharged against medical advice.
The outcome of the patients
In this study, the case fatality rate of tetanus was 48.5%. Some were discharged against medical advice, and three (9.1%). Most patients, 17 (51.5%), were admitted for less than seven days. Table 2 shows worse outcomes for those with more severe disease at presentation based on Ablett's classification of tetanus severity. Table 3 describes how age, gender, and year of consultation affect the outcome of the patients. The mean hospital stay for patients who died was four days (SD = ± 3), as shown in Table 4. The relationship between tetanus mortality and key factors is shown in Table 5. The higher mortality rate was found in patients with an incubation period of fewer than seven days, the onset of trismus less than eight days after exposure, generalized spasms less than eight days after exposure, presence of autonomic dysfunction (abnormal pulse and/or abnormal blood pressure) and presence of respiratory dysfunction. The lone patients who had their portal of entry located on the trunk died. Patients who applied or introduced local regimens, and soil or animal wastes at the portal of entry had higher mortality. Similarly, higher mortality was noted amongst patients with late-onset of debridement (done more than 48 h after the onset of tetanus). Higher mortality was also noted in patients with high Ablett's classification.
Patient's outcome based on age categories, gender and year of consultation.
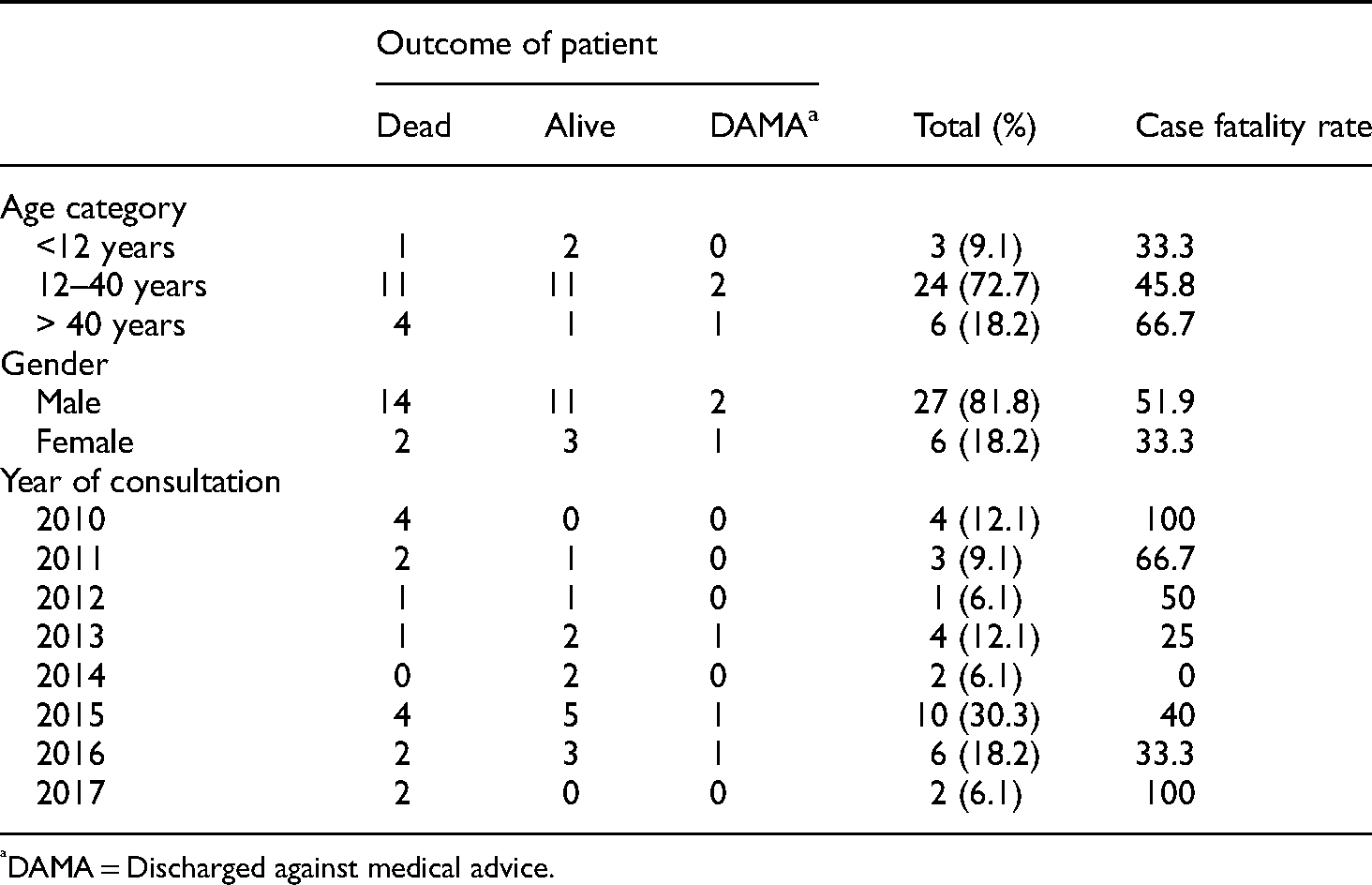
DAMA = Discharged against medical advice.
Average length of hospitalisation.

SD = Standard deviation.
Factors significantly associated with mortality in patients with tetanus.

Discussion
This study identified, 33 tetanus cases, giving a proportion of about 1 per 2500 admissions; which is lower than that reported by Fawibe et al. in 2010 in Nigeria (11.7 per 1000). 9 The difference in the above findings is probably because their study period involved an earlier time frame (2002 to 2006); hence there may have been a significant improvement in vaccination coverage and other preventive measures, especially in combating maternal and neonatal tetanus.
The mean age of tetanus cases in this study was 32.4 (SD ± 18.9) years; which included two children of ages 8 and 10 years. This illustrates the impact of low vaccination coverage in a low-resource country. High-income countries have reported tetanus cases to be more frequent in elderly women, as a result of better vaccination coverage in these settings.15,16 There was a higher prevalence of tetanus in males than in females. Owolabi et al. in 2011 in Northwestern Nigeria, 7 Chalya et al. in 2011 in Northwestern Tanzania, 10 and Fawibe et al. in 2010 in a sub-urban tertiary hospital in Nigeria 9 reported similar findings. Low tetanus vaccination rates could explain these findings among males compared to their female counterparts who often get vaccinated during pregnancy, as shown by Shona et al. in a study done in 2016 in 14 Countries in Eastern and Southern Africa. 17 Moreover, the involvement of males in more risky professions, including farming and construction, with greater vulnerability to injury may also be a logical explanation.
In our study, the most common type of tetanus was generalised tetanus, which is similar to previous studies by Fawibe et al. in 2010 in a tertiary hospital in Nigeria 9 and Godfrey et al. in 2009 in Uganda. 18 There was no case of neonatal tetanus in our study and this could be the result of actions implemented by the ministry of public health which includes but is not limited to tetanus vaccinations in children and pregnant women and the active surveillance of neonatal tetanus cases.
Our study revealed that no patient was immunised for tetanus before the onset of the disease. This finding could explain the high mortality rate since previous tetanus immunisation history is a prognostic factor according to the research carried out by Owolabi et al. in 2011. 7 Other studies have shown a higher number of patients that have been vaccinated against tetanus before the onset of the disease, such as the study carried out in Tanzania by Phillipo et al. in 2011, which revealed that 24 (23.5%) patients had a history of prior tetanus vaccination 10 and similarly Owolabi et al. reported an immunisation rate of 49% in Northwestern Nigeria among tetanus cases. 7 The disparity in this result could be because they had a larger sample size. For instance, the study carried out in Tanzania had a sample size of 102 patients, and a tetanus immunisation history was available in all inpatient files. Unlike in our study, we had a smaller sample size, and only one-third of the inpatient files had information on tetanus immunization.
The mortality rate of tetanus in our study (48.5%) was higher than that obtained in some studies outside Africa, such as Bangladesh, with a mortality rate of 22.5%, as reported by Feroz et al. 19 The absence of an intensive care unit in Buea and Limbe Regional Hospitals and inadequate intensive care facilities in Bamenda Regional Hospital is a probable explanation for this. Routinely, tetanus cases are managed with wound care, metronidazole, antitetanus vaccine, TIGs, and diazepam to control spams. Other more advanced management modalities include the use of magnesium sulfate for severe spasms, beta-blockers for autonomic dysfunction, and mechanical ventilation for patients with respiratory insufficiency. 14 However, these modalities are seldom available in our setting and most probably contributed to the high mortality reported in this study. Financial constraints that often hamper the successful management of such patients could also explain the high mortality rate. Other possible reasons for the high mortality rate include no history of tetanus vaccination, more than one-third of patients not given proper wound care following admission, and up to 95% of patients with respiratory dysfunction never receiving respiratory support. However, the mortality rate in this study is comparable to other studies in Africa, such as Nigeria, where three studies revealed a 42.9%, 46%, and 36.9% mortality rate in Rivers State 5 North-western Nigeria, 7 and Lagos respectively, 20 42% in rural Ugandan Hospital 18 and 43.1% in North-western Tanzania. 10
A higher mortality rate was found in patients with incubation periods that were less than seven days. This is similar to previous studies such as that carried out by Onwuchekwa et al. in 2009, 5 Owolabi et al. in 2011, 4 Chalya et al. in 2011 10 and Saltoglu et al. in 2004. 21
The onset of trismus and generalized spasms less than eight days from exposure equally showed a higher mortality rate. This was similar to a study by Owolabi et al. in Northwestern Nigeria in 2011 that showed an association between mortality and the period of onset of spasms (defined as the duration from the first symptom to spasms). 7 A study carried out by Fawibe et al. could explain this finding, which showed that patients with prolonged and severe spasms at a sub-urban tertiary hospital in Nigeria were more likely to suffer cardio-respiratory complications of tetanus and are more likely to die from it compared to those with mild spasms. 9 It, therefore, implies that effective control of severe spasms can significantly reduce the mortality rate, especially in cases of early onset of spasms.
The presence of autonomic dysfunction with abnormal pulse and/or abnormal blood pressure was found to be higher in patients who died. This is similar to findings in two different studies in North-western and South-eastern Nigeria.7,22 Amongst patients who did not survive, many had respiratory dysfunction. This result was similar to other studies carried out by Feroz et al. in 2007 in Bangladesh, Godfrey et al. in 2009 in Uganda, and Chalya et al. in 2011 in North Western Tanzania(10,18,19).
Most patients that applied or introduced local regimens, soil, or animal waste at the portal of entry died. This finding is consistent with the literature that explained that Clostridium tetani is found in soil and animal waste; thus, applying it to a wound exposes the patient to more tetanus spores and, hence, severe infection.23–25 Debridement or proper wound cleaning and dressing after 48 h of the onset of symptoms of tetanus was found more frequently among patients who did not survive. This is similar to the finding in a study conducted by Farrar et al., which showed a decrease in mortality in cases of proper wound care. 26 Most patients who had higher disease severity on admission based on the Ablett Severity score died. Similar results were seen in studies in Nigeria and Turkey.7,10,21
Conclusion
Vaccination policies for pregnant women and infants seem to be effective in Cameroon since there were no cases of tetanus among infants. This study, therefore, highlights the need to ensure universal vaccination coverage for high-risk populations; males, active population (20–40 years), and farmers. More still, this study emphasizes the need to improve access and utilisation of mechanical ventilation in severe tetanus cases.
What is known about the topic?
Tetanus is a significant cause of death in sub-Saharan Africa, with a case fatality rate ranging from 26% to 64%.
In addition to the limited availability of intensive care facilities, poor socio-economic status of patients, and poor vaccination coverage, mortality of tetanus patients in sub-Saharan Africa may be influenced by modifiable and non-modifiable factors such as patient's age, the incubation period, prior history of tetanus vaccination, tetanus severity, and complications, and delays in treatment.
In Cameroon, no published data exist on the factors associated with mortality in patients with tetanus. Filling this research gap will help guide preventive strategies and coin adequate clinical and public health policies to lower the mortality rate of this highly preventable disease.
What this study adds to the topic
The mortality rate of tetanus in this study was 48.5%.
Only one patient was intubated (3%) in our study. This emphasizes the need to improve access and utilisation of mechanical ventilation in severe tetanus cases which could have reduced mortality significantly.
Vaccination policies for pregnant women and infants seem to be effective in Cameroon since there were no cases of tetanus among infants. High-risk populations (males, active population, farmers) are missed by routine tetanus vaccination programs.
Limitations of the study
This study was based on a small number of patients recruited from three urban hospitals, thus generalisability of our results is limited. Moreover, this study was retrospective, and records were sometimes void of essential information to grade the severity of diseases, hence increasing the risk of nondifferential misclassification of cases.
Footnotes
Acknowledgments
Our deep gratitude goes to the hospital staff and administration for permitting us to conduct this study.
Author's contributions
SCN designed the study, wrote the protocol, and collected and analyzed the data. CAM, and PJN supervised the study at every stage. EM and SCN wrote the article. EM, TVB, NAF revised the article until submission for publication. All authors have given their consent to submit the article.
Availability of data and materials
Data used for this research is available from the corresponding author upon reasonable request
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethics approval and consent to participate
This study was conducted in compliance with the Helsinki Declaration and all applicable national laws and institutional rules and has been approved by the author's institutional review board. Ethical approval was granted by the faculty of health sciences institutional review board under the reference 2017/003/UB/SG/IRB/FHS on 12/04/2017. Since this was a retrospective database study, informed consent was not obtained from the participants and/or legal guardians.