
Abstract
Introduction
Hospital admission due to fragility hip fracture has increased significantly in recent years. Annually, 320,000 cases are reported in the United States of America. Among the most common postoperative complications after hip fracture repair is delirium with an incidence of up to 53.3%, a substantially higher rate than with other elective surgeries according to recent meta-analyses. 1
Several risk factors have been recognized, such as gender, age, medications, prior cognitive impairment, and comorbidities, which can precipitate postoperative delirium. Among these factors, perioperative hypotension, hypoxemia, and anemia are some conditions whose prevention and adequate early management can prevent delirium.2,3 Similarly, the physiological stress caused by the injury, hospital admission, associated pain, and surgery contribute to the appearance of delirium. 3
Of these factors, pain management has been extensively studied. In patients with hip fracture, perioperative pain management is usually with opioids, whose dosage is difficult to adjust and have many side effects, especially in older adults. Studies have shown that patients with cognitive impairment or dementia receive less analgesia than cognitively intact patients. 4 In surgical patients, an association has been reported between high levels of pain at rest and the development of post-surgical delirium, as well as in older patients with hip fracture and untreated pain. 5 For this reason, new pain management schemes such as the fascia iliaca block (FIB) have recently emerged. The application of this preoperatively has shown important benefits such as greater early patient mobility, reduced hospital stay, lower pain scores, and fewer opioid requirements.5,6
The purpose of this study was to determine the impact and the advantages of the implementation of the FIB in older adults with hip fracture due to fragility include in the Orthogeriatric Clinical Care Center of the Fundación Santa Fe de Bogotá and of the San José Infantil University Hospital in Bogotá, Colombia.
Methodology
Study design and inclusion criteria
An observational analytical cohort study with retrospective data collection was conducted on patients managed by the Orthogeriatric Clinical Care Center of the Fundación Santa Fe de Bogotá (FSFB) and the San José Infantil University Hospital (HUSJI) from the beginning of 2019 to the end of 2020. The study was approved by the corporate research ethics committee of both institutions and complies with the ethical principles for medical research of the Declaration of Helsinki on 8 October 2020. All patients between January 2019 and December 2020, who were older than 65 years and had a diagnosis of fragility hip fracture or periprosthetic hip fracture confirmed by X-ray were selected consecutively. Patients with a diagnosis of hip fracture due to polytrauma or high-energy trauma, hip fracture associated with tumor or metastatic disease, fracture of more than seven days of evolution, and diagnosis of delirium on hospital admission, identified via the Confusion Assessment Method (CAM) diagnostic algorithm, were excluded. This study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines to ensure transparency and accuracy in the presentation of our findings.
Study population
A total sample of 241 patients was obtained, from which 23 patients were excluded, for a final sample of 218 patients. The flow diagram of patient enrollment can be found on Figure 1.

Flow diagram of patient enrollment.
Sociodemographic data including age, sex, body mass index (BMI), fracture classification (according to the AO Trauma and Vancouver classification), and comorbidities were collected. Within the clinical and surgical parameters, it was recorded whether the patient underwent a preoperative fascia iliaca block, as well as hemoglobin, and hematocrit on admission and 6 h postoperatively, time from admission to the emergency department to surgery, classification of the American Society of Anesthesiologists (ASA) for risk of anesthesia, type of anesthesia, type of surgical procedure, duration of surgical procedure, and hospital stay.
The presence of hospital complications were also collected. This included pressure ulcers, nosocomial pneumonia, urinary tract infection (UTI), transfusion requirement, ICU admission, vasopressor support requirement, inotropic support requirement, surgical site infection, acute myocardial infarction (AMI), acute renal failure (ARF), respiratory failure, cerebrovascular accident, deep vein thrombosis (DVT), pulmonary thromboembolism (PTE), in-hospital delirium, time to onset of delirium, and in-hospital death. Similarly, the consumption and administration of opioids were documented throughout the hospital stay of the patients included in the study. Subsequently, the equivalent dose of the opioid medication administered in milligrams of morphine was calculated. This was done through the morphine milligram equivalence calculator on the MDCalc website, 7 which is a tool used to calculate the morphine equivalent milligrams between the different opioids and their difference in terms of their potencies.8,9
Study outcomes
The primary outcome of our study is the incidence of delirium, identified via the CAM diagnostic algorithm, during hospitalization, a critical concern in the elderly population, as it can significantly impact patient recovery and hospital resources.
Secondary outcomes of this study include postoperative opioid requirements, duration of hospital stay, rates of Intensive Care Unit (ICU) admissions, and in-hospital mortality rates. These secondary outcomes will provide a comprehensive overview of the potential advantages of FIB, including pain management effectiveness, overall hospitalization experience, and survival outcomes, thereby offering insight into the holistic benefits of adopting FIB as a standard preoperative analgesic intervention in this vulnerable patient demographic.
Data analysis
An exploratory analysis of the variables was carried out, calculating proportions and frequencies for the discrete variables and measures of central tendency, dispersion, maximum, and minimum for the continuous variables. The Shapiro-Wilk test was applied as a normality test. To analyze the differences between the two study groups, the comparison of proportions test and the chi-square test were implemented, as well as the T-test and the Mann-Whitney test to compare the continuous variables by period. All analyses were performed using SPSS v. 26.0 and Real Statistics v. 7.3.
Results
A total of 218 patients were included in the study. The mean age was 83 years (±7.86) and a general predominance of the female gender was observed with 170 women and 48 men. The average BMI of the sample was 24.2 kg/m2 (±0.3). Regarding comorbidities, most of the operated patients suffered from two or more pathologies (75.7%), including the most common arterial hypertension (34.8%), hypothyroidism (18.3%), and chronic obstructive pulmonary disease (6.4%). The most common type of fracture was AO 31-A2 (22%), followed by AO 31-A1 (14.7%) and AO 31-B2 (11.5%), and more than half (59.2%) were from the left lower limb. The most performed surgical procedures were cephalomedullary nail fixation (55.5%) and total hip replacement (29.4%) (Table 1).
Sociodemographic and fracture data of the patients.
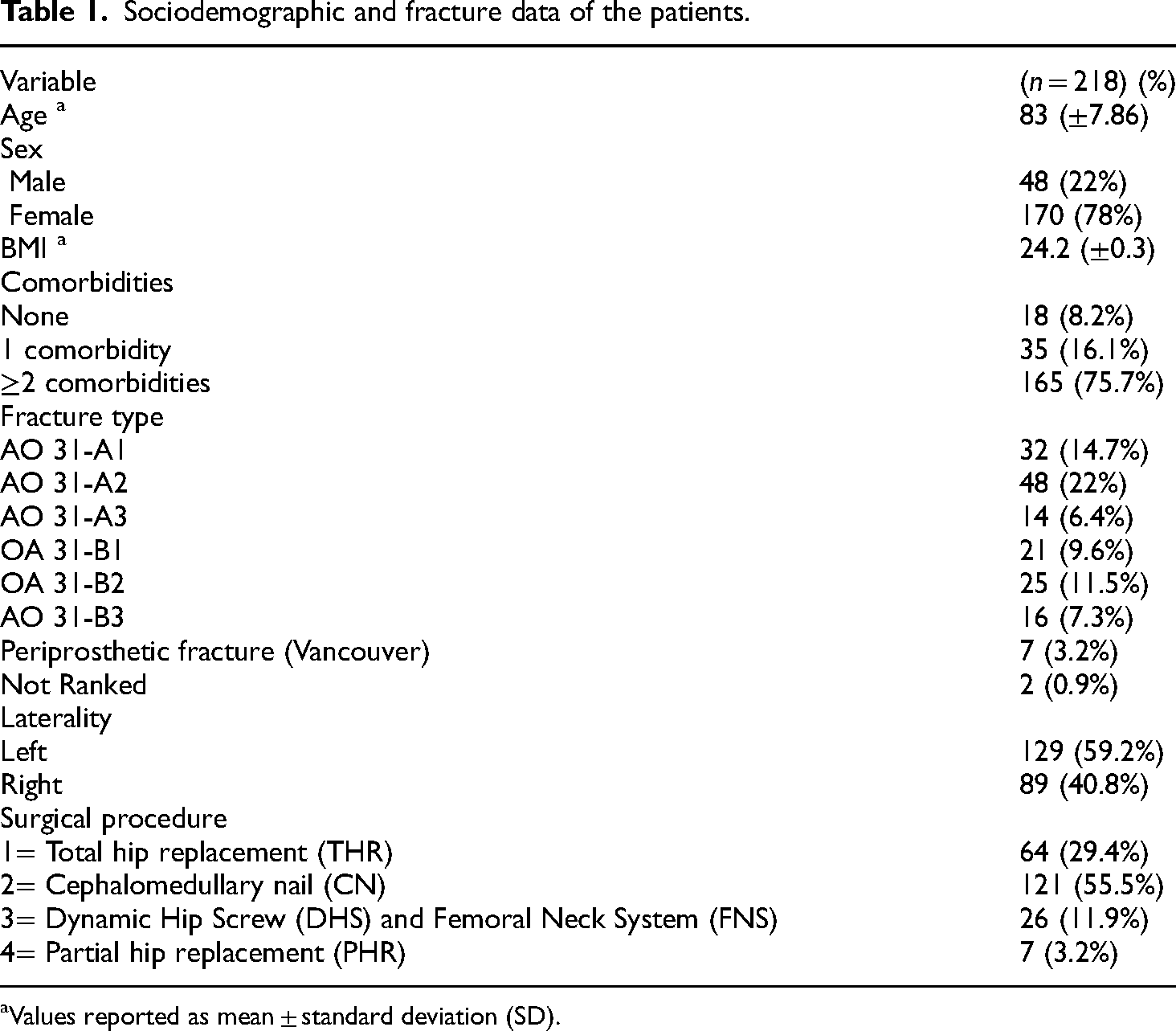
Values reported as mean ± standard deviation (SD).
A total of 119 patients received conventional analgesic management and 99 patients underwent preoperative fascia iliaca block. There was no relationship between the use of blockade and the development of delirium during hospitalization (p = 0.442). However, it was found that older age (p = 0.010), ICU admission (p = 0.021), urinary tract infection (p = 0.002), and respiratory failure (p = 0.001) were associated with delirium. When the Chi-square and Fisher tests were performed to identify whether there was an association between the discrete variables between both groups, no statistically significant difference was identified (Table 2).
Association between discrete variables and preoperative block.
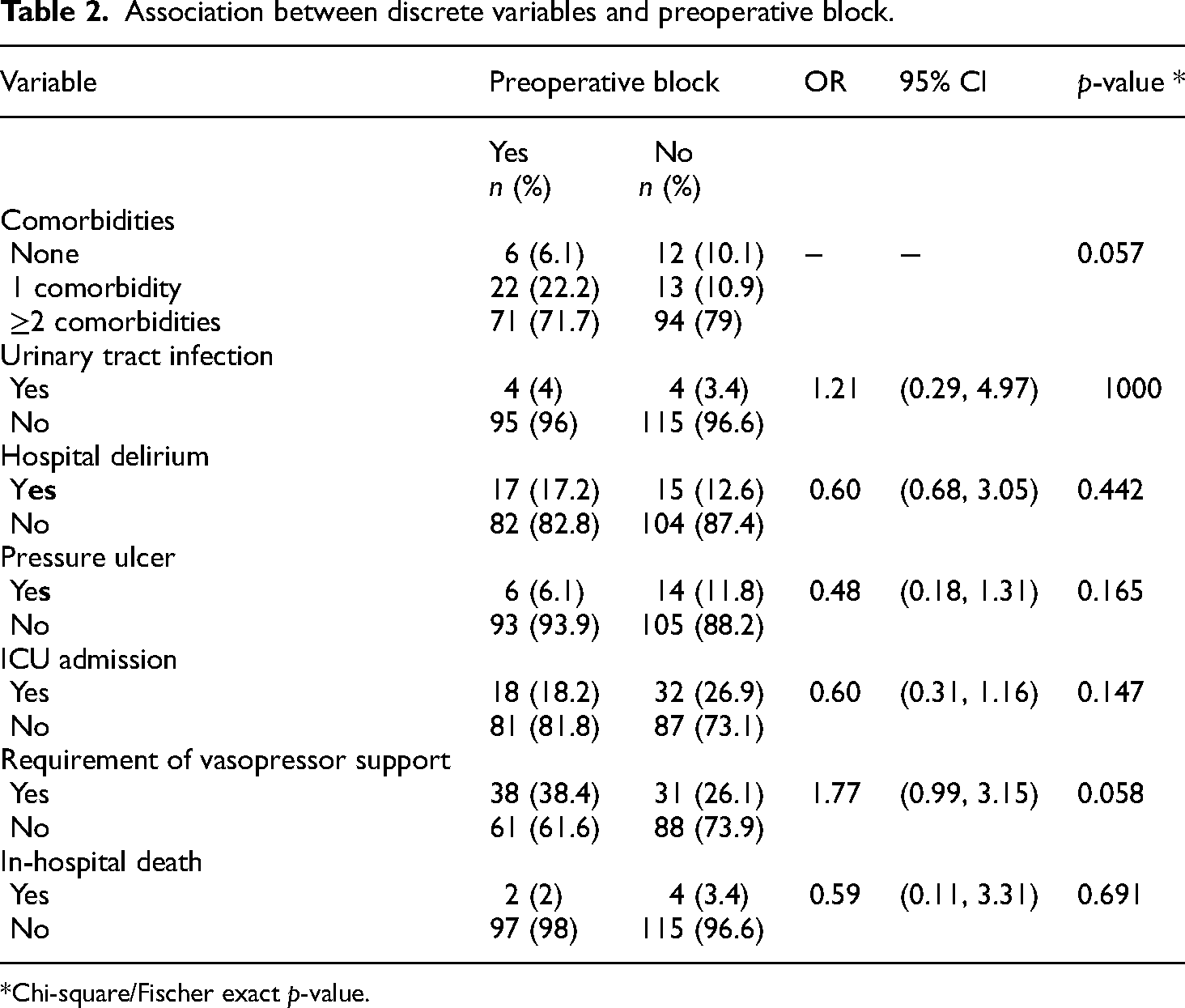
*Chi-square/Fischer exact p-value.
Additionally, a higher consumption of opioids was found in the patients who did not undergo a block compared to the patients who received a preoperative block (27.61 mg vs 16.34 mg, respectively, p = 0.003) and a longer duration of the surgical procedure (90.84 vs 81.08 min, respectively, p = 0.03) with a statistically significant difference in both. The patients with blockade also presented a shorter hospital stay (6.06 vs 5.41 days, respectively, p = 0.641) but without a statistically significant difference (Table 3).
Association between continuous variables and preoperative block.
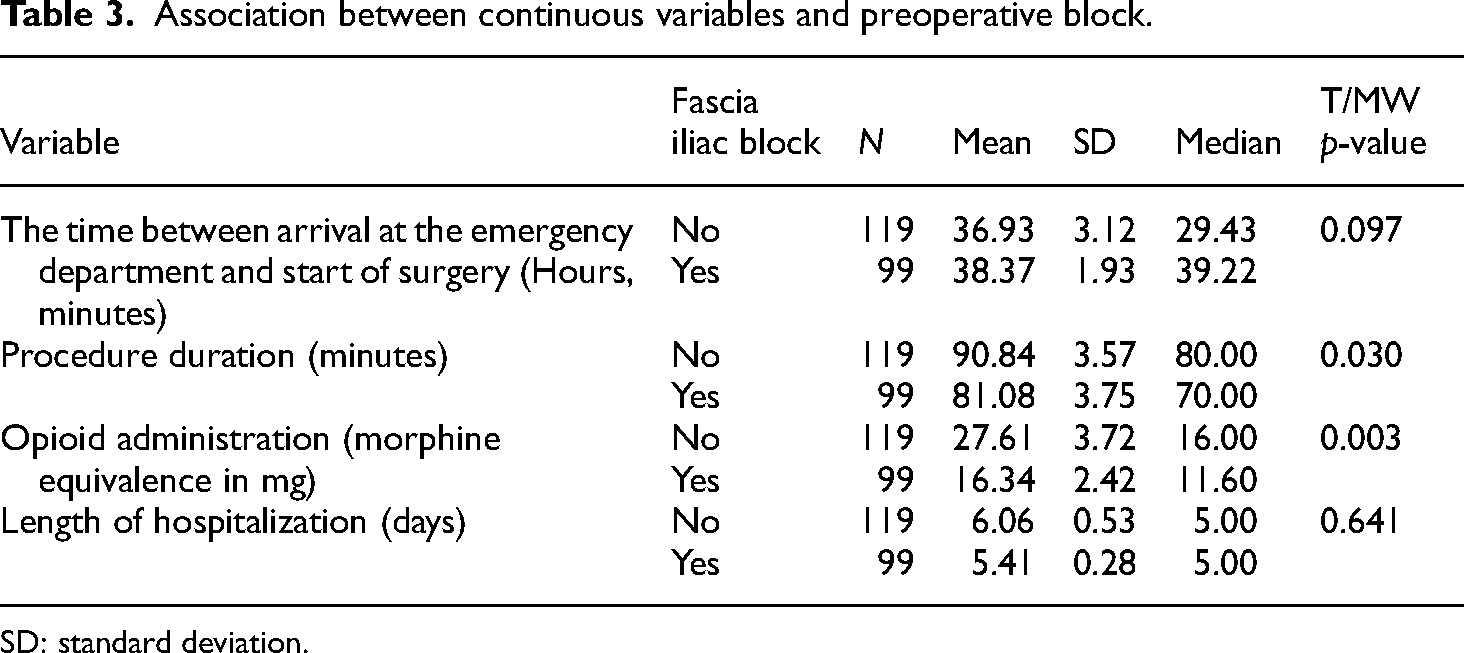
SD: standard deviation.
Discussion
Delirium, a common postoperative complication, is associated with longer hospital stays, increased healthcare costs, and elevated morbidity and mortality rates.10,11 The use of opioids for pre and postoperative pain management in older adults with hip fracture is a common practice that has numerous limitations due to its wide spectrum of side effects, especially in this population. 10 For this reason, alternatives have recently been proposed for multimodal pain management using regional anesthesia techniques such as fascia iliaca block, which has shown a significant decrease in opioid use in these patients in various studies. 11
Likewise, the relationship between pain management in older adults with a hip fracture and the risk of pre-and postoperative delirium has been extensively studied due to the important negative effect that this complication can have on the morbidity and mortality of these patients. 12 In a systematic review and meta-analysis by Kim et al. (2022), no significant difference was identified between the use of a fascia iliaca block and the incidence of delirium (OR, 0.89; 95% CI: 0.19–4.19; p = 0.88; I2 = 78%). 13 Similarly to our results, in the study by Mouzopoulos et al. (2009) it was evidenced that in the group that underwent the fascia iliaca block compared to the placebo group, the incidence of delirium was 10.78% versus 23.8%, respectively (RR 0.45, 95% confidence interval 0.23–0.87). Furthermore, the duration of delirium was 5.22 days versus 10.97 days, respectively (95% CI 3.87–7.62, p = 0.001). 14
Additionally, the study by Lim et al. (2021), found a lower incidence of delirium in the group that underwent peripheral nerve block compared to the control group (15% vs 27%, respectively, p = 0.027). However, there was no evidence of a difference in the consumption of opioids during the first two postoperative days. 10 On the other hand, in the present study, a statistically significant decrease in the consumption of opioids was obtained in the group of patients with fascia iliaca block from their admission to the emergency department. Likewise, the randomized clinical trial by Unneby et al. (2017) showed a reduction in the consumption of opioids in the group that underwent blockade (2.3 ± 4.0 vs 5.7 ± 5.2 mg, p = 0.001). 15 Furthermore, in a retrospective study conducted by Jain et al. (2022), 81 patients from their cohort of 166 were administered a fascia iliaca block plus systemic opioids, resulting in a reduction of morphine equivalents by 0.6 mg/h compared to the 85 patients who received only systemic opioids. 16
In this article, it was evidenced that the group with fascia iliaca block had a shorter duration of the surgical procedure (81.08 vs 90.84 min, p = 0.030) and hospital stay (5.41 vs 6.06 days, p = 0.641) compared to the patients who received conventional analgesia. These benefits of using the fascia iliaca block can be corroborated by the study by Hao et al. (2022) where a reduced hospital stay of 2.12 days was evidenced in the blockade group compared to the control group (p = 0.13). In addition, it was found that the pain score at rest and when moving the lower extremity at six hours, one day, three days, and one week postoperatively was lower in the block group compared to the routine analgesia group (p = 0.05). 17 Although the FIB has shown promise in reducing hospital stay, its impact on the duration of surgery remains unclear and is not well-documented. One possible explanation is that effective preoperative analgesia from FIB may reduce the need for intraoperative pain management and sedation adjustments. This could allow for a smoother surgical workflow, as patients who receive a blockade may experience less anxiety and discomfort before and during the procedure. Additionally, FIB might help minimize intraoperative interruptions for pain control, thereby contributing to shorter procedural times. While these effects are plausible, further studies are needed to confirm any influence of FIB on surgical duration.
No significant difference was found between the use of blockade and the development of in-hospital complications such as urinary tract infections, delirium, and pressure ulcers. These results are similar to those of the study by Hao et al. (2022) and Unneby et al. (2020).15,17 However, a Cochrane systematic review on the use of peripheral nerve blocks in hip fractures found no difference in the risk of delirium in seven of the 31 included trials (RR 0.69, 95% CI 0.38 to 1.27 I2 = 48%; very low quality of evidence) but there was a difference in complications such as pneumonia (RR 0.41, 95% CI 0.19 to 0.89; I2 = 3%; number needed to treat for additional beneficial outcome 7, CI 95% 5 to 72; moderate quality of evidence). 18 This demonstrates the wide spectrum of findings that exist about this topic and its complexity.
Regarding the study's weaknesses, one of the main ones is the retrospective nature of the data collection, since for this reason the initial reporting of patient information in the medical records was not done homogeneously (for example, not all patients had the same rating scales for certain variables) and there was a significant loss of data that limited the number of subjects included in the study, which in turn diminished the power of the study. An additional limitation of this study is the lack of a pre-calculated sample size, as we used a non-probabilistic convenience sampling method. This approach may introduce selection bias and limit the generalizability of the findings, potentially reducing the study's statistical power.
On the other hand, one of the strengths of the study is that it collects data from patients with similar characteristics from two different medical institutions, which increases the external validity of the results obtained.
The findings of this study are important because it is an adjuvant method for the analgesic management of patients with hip fracture. This study and the review of the literature showed a reduction in opioid consumption and a shorter length of hospital stay. In addition, it does not present a risk of presenting any adverse event and/or complications during hospitalization in these patients.
Conclusion
This study sought to identify the benefits of fascia iliac block. Favorable results were evidenced about in-hospital orthogeriatric management. Likewise, the impact it has on the functionality and future morbidity and mortality of these patients. Therefore, the fascia iliac block can be considered an effective analgesic method for admission to the emergency department for older adults with fragility hip fracture.
Footnotes
Author contributions
Andres Libos: conceptualization, original draft preparation, writing of the manuscript and supervision of the research activities. Jonathan Tihanyi: conceptualization, original draft preparation, writing of the manuscript and supervision of the research project. Juan Bernate: review and editing of the manuscript, visualization of data, data curation, and analysis of study data. Laura Ricaurte: review and editing of the manuscript, formal analysis of the study data, and anaesthesiologist in charge of investigation processes. Diana Morales: validation of results, formal analysis, and review and editing of the manuscript. Aldo Patiño: validation of results, formal analysis, data curation, and review and editing of the manuscript. Rodrigo Pesantez: validation of results, formal analysis, and review and editing of the manuscript. Julian Salavarrieta: validation of results, formal analysis, and review and editing of the manuscript. Valentina Sanint: validation of results, formal analysis, and review and editing of the manuscript. Ana Lopez: supervision, project administration, and geriatrician in charge of final review of manuscript. Carlos Olarte: supervision, project administration, and orthopaedic surgeon in charge of final review of manuscript. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and approval was granted on October 8, 2020 (CCEI-12504-2020). The Institutional Review Board (IRB) at Fundación Santa Fe de Bogotá acted as the central IRB, whose review was acceped by all participating institution's IRBs. The central IRB determined that this research involved no greater than minimal risk and approved a waiver for informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.