
Abstract
Physical inactivity is associated with comorbidities and mortality in chronic obstructive pulmonary disease (COPD) patients. Although non-exercise activity thermogenesis (NEAT) is important for evaluating the physical activity level (PAL) of patients with chronic diseases, it has not yet been assessed in COPD patients. This study included male patients with COPD (n = 28) and high risk for COPD (n = 8). Total energy expenditure (TEE) and basal metabolic rate (BMR) were measured using the doubly labeled water (DLW) method and indirect calorimetry, respectively. PAL was calculated as TEE/BMR, while the NEAT was obtained from a questionnaire. Physical activity was also assessed using an accelerometer. The total NEAT score was correlated with PAL (r = 0.534, P < 0.001), while PAL was correlated more strongly with the non-locomotive NEAT score (r = 0.548, P < 0.001) than the locomotive NEAT score (r = 0.278, P = 0.10). Regarding accelerometer-obtained data, this questionnaire mainly reflected steps/day and the duration of light locomotive and non-locomotive daily activities. The NEAT score is a possible option for evaluating PAL in daily clinical practice. The present results indicated that non-locomotive activity may have a greater impact on PAL than locomotive activity in COPD patients.
Keywords
Introduction
Physical inactivity and prolonged sedentary time are recognized indicators of poor prognosis in chronic obstructive pulmonary disease (COPD).1,2 A greater amount of low-intensity physical activity reduces the risk of COPD hospitalization; however, high-intensity physical activity does not. 3 In this respect, being physically active and limiting sedentary behavior (i.e. decreased time sitting and increased time walking or doing housework daily) are essential to improve COPD outcomes. Although questionnaires and accelerometers are generally used for assessing the physical activity level (PAL) of individuals with COPD, they have inherent issues related to over- and underestimation and data reproducibility.4–7
The doubly labeled water (DLW) method is the gold standard for estimating total energy expenditure (TEE) in daily life, which is essential to determine the energy requirements of COPD patients. PAL determined by TEE with the DLW method and BMR with the indirect calorimetry is also the most reliable measure to evaluate daily activity levels. However, this method involves high costs and requires significant technical expertize for implementation and analysis; therefore, studies using the DLW method have been limited to small or moderate-sized populations.8–10
Non-exercise activity thermogenesis (NEAT) is defined as the energy expended performing regular daily activities (such as going to work, attending school, singing, washing clothes, and cleaning floors) that do not constitute planned exercise or sports.11,12 In general, NEAT can be calculated using energy subtraction (NEAT = TEE − basal metabolic rate (BMR) − intended exercise − thermic effect of food) or a questionnaire that incorporates NEAT as a component. Given that NEAT is impacted by two types of factors that may differ between countries—environmental factors, such as the type of dwelling or occupation, and biological factors, such as weight, sex, and body composition 13 —it is essential to compose a questionnaire that is suitable for each region. Recent studies have demonstrated that NEAT in patients with metabolic diseases such as diabetes mellitus and obesity can successfully be evaluated using a NEAT questionnaire that has been modified for the Japanese population. 14 Minakata et al. reported that most Japanese COPD patients have reduced levels of physical activity, at ≥3.0 metabolic equivalents (METs), compared to the healthy older population. 15 However, it is unclear which component of activity energy expenditure (AEE), intended exercise activities or NEAT, was reduced in these patients. Furthermore, we have recently reported that the accelerometer underestimates AEE and that the correlation of PAL with both the DLW method and the accelerometer is moderate (r = 0.642). 16
In this study, we intended to clarify the contributions of NEAT to daily physical activities represented by PAL in COPD. To the best of our knowledge, there are no reports assessing the relationship between NEAT and PAL in COPD. Thus, we evaluated the associations between the NEAT score and PAL by the DLW method and the accelerometer parameters for various activities.
Material and methods
Patients and study design
This study formed part of our previously published cross-sectional observational study. 16 Male outpatients with stable (n = 28) or high-risk COPD (n = 9) were recruited from Saitama Medical University Hospital between June 2017 and February 2018. COPD was diagnosed in accordance with the 2020 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines. 17 We included COPD patients (GOLD 1–4) and high-risk for COPD (GOLD 0) who were clinically stable and free of exacerbations at least for a month before recruitment. All patients classified as GOLD 0 presented with chronic respiratory symptoms including cough, phlegm production or dyspnea during exertion, and had a ≥10 pack-year smoking history with a post-bronchodilator FEV1/FVC ≥ 0.7. Since their COPD Assessment Test (CAT) scores were similar to those of COPD patients (9.6 ± 4.0 vs. 10.2 ± 6.7) and most (n = 6) experienced an improvement in their symptoms after using bronchodilators, GOLD 0 patients were included in the total population of this study. One patient at GOLD 0 discontinued the study because of acute bronchitis, and a total of 36 patients were used in the analysis.
The exclusion criteria included those individuals who were; diabetes mellitus with medication use, treatment for infectious diseases, dysphagia, other serious diseases that could interfere with movement, those using drugs that affect energy balance (such as thyroid hormones, and glucagon-like peptide-1 receptor agonists, beta-blockers) or water balance (such as sodium-glucose co-transporter 2 inhibitors); and over 5% weight loss of the body weight during the previous 3 months.
This study protocol was approved by the Ethics Committee of Saitama Medical University Hospital (No. 16-003-1), Keio University (Protocol No. 2015-03), and the National Institutes of Biomedical Innovation, Health and Nutrition (Protocol No. 29). All particssssss gave written informed consent.
Evaluation of PAL using the DLW method and an accelerometer
Details regarding measurements of PALDLW (PAL evaluated using the DLW method) and PALACC (PAL evaluated using an accelerometer) are provided in our previous reports.
16
In brief, TEEDLW (TEE evaluated using the DLW method) was measured for 13–15 days; BMR was measured through indirect calorimetry (BMRI) using a ventilated hood (Quark RMR; Cosmed, Rome, Italy), and was calculated using the modified Weir equation.
18
The PALDLW was calculated using the following equation
19
:


Assessment of NEAT using a questionnaire
We questioned participants about their daily activities to evaluate NEAT and allocated a NEAT score. The questionnaire consisted of 11 and 25 questions concerning locomotive and non-locomotive activities, respectively (Supplementary Material 1). 24 The questionnaire was modified according to the Japanese lifestyle using the Adult Compendium of Physical Activities. 25 Each questionnaire item was allocated a score between 1 and 3 points, based on the level of activity, and the scores were added together to determine the total NEAT score.
Statistical analysis
Results for continuous variables are expressed as mean ± standard deviation (SD), unless otherwise specified. All data were analyzed using JMP version 14 software (SAS Institute Inc., Cary, USA). The normality of outcomes was examined using the Shapiro–Wilk test. Correlation analysis was performed to analyze the correlation of the NEAT scores with PAL, and the values obtained from the accelerometer using Pearson's correlation when the distribution was normal. Results showing non-normal distribution (light/moderate/vigorous locomotive and moderate non-locomotive) were analyzed with Spearman's correlation. P-values ≤ 0.05 were considered statistically significant.
Results
Patient characteristics
Table 1 showed the baseline characteristics of the study participants. The patients presented with a wide spectrum of disease severity with a mean %FEV1 of 69.4. Mild to moderate COPD patients (20/36) were primarily in the total population. The mean ± SD of the total NEAT score and PALDLW was 59.9 ± 8.6 and 1.80 ± 0.2, respectively.
Patient characteristics.

Data are presented as mean ± SD. BMI: body mass index; GOLD: the Global Initiative for Chronic Obstructive Lung Disease; FEV1: forced expiratory volume in 1 s; TEE: total energy expenditure; BMRI: basal metabolic rate measured by indirect calorimetry; PAL: physical activity level; PALDLW: PAL by DLW; PALACC: PAL by accelerometer; AEEACC: activity energy expenditure by accelerometer; NEAT: non-exercise activity thermogenesis.
Correlation of NEAT scores with PAL
Results of the bivariate analysis of the NEAT scores and PALDLW are illustrated in Figure 1. The total NEAT score was correlated with PALDLW (r = 0.534, P < 0.001); PALDLW was also correlated with the non-locomotive NEAT score (r = 0.548, P < 0.001), but not with the locomotive NEAT score (r = 0.278, P = 0.10; Figure 1(a)–(c)). When the data of the patients classified as GOLD 0 were excluded, all three scores were correlated with PALDLW (total NEAT score: r = 0.523, P < 0.01; locomotive NEAT score: r = 0.456, P < 0.05; non-locomotive NEAT score: r = 0.495, P < 0.01). Both the locomotive and non-locomotive NEAT scores were significantly correlated with the total NEAT score (r = 0.689, P < 0.0001 and r = 0.965, P < 0.0001, respectively; Figure 2(a) and (b)).

Correlation of the NEAT scores with PAL in the total population (n = 36). NEAT: Non-exercise activity thermogenesis, PALDLW: Physical activity level measured using the double labeled water method.
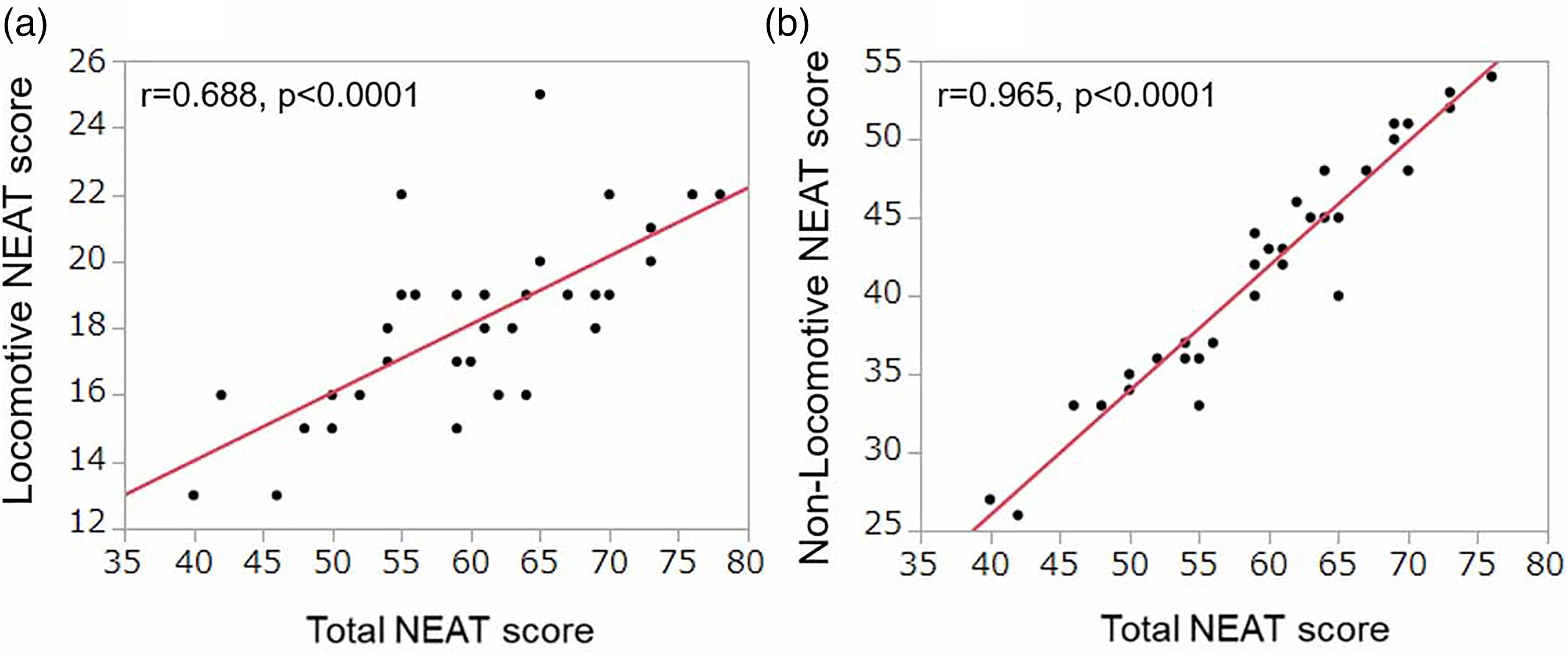
Correlation of the total NEAT score with (a) the locomotive NEAT score, and (b) the non-locomotive score in the total population (n = 36). Significant correlations were observed between the two variables. NEAT: Non-exercise activity thermogenesis.
Correlation of NEAT scores with accelerometer-obtained data
Results of the bivariate analysis of the NEAT scores and the data obtained from the accelerometer are shown in Table 2. All the three NEAT scores were correlated with steps/day and the duration of moderate locomotive/non-locomotive activities. The total and the non-locomotive NEAT scores were also correlated with the duration of light non-locomotive activity as well as AEEACC and PALACC but not with the locomotive NEAT score. When we calculated PALACC using BMRI instead of BMRG, the correlation was similar to that of PALACC with BMRG (total NEAT score (r = 0.477, p = 0.003), non-locomotive NEAT score (r = 0.465, p = 0.004), and locomotive NEAT score (r = 0.31, p = 0.062)).
Correlation of NEAT scores with values obtained from the accelerometer (n = 36).
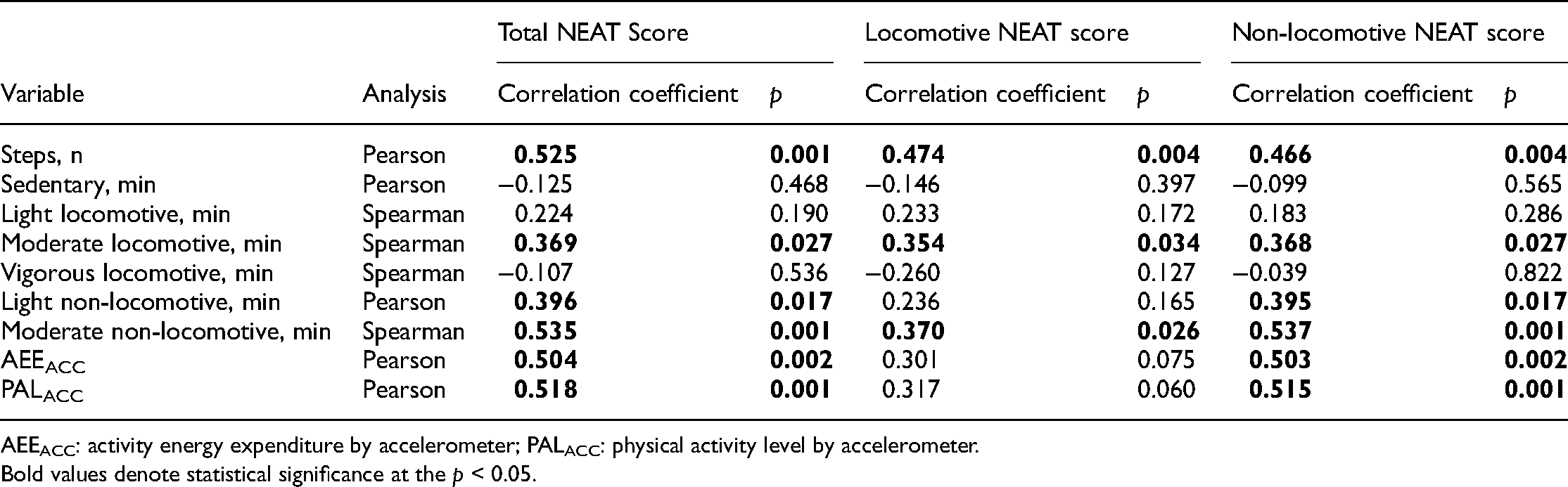
AEEACC: activity energy expenditure by accelerometer; PALACC: physical activity level by accelerometer.
Bold values denote statistical significance at the p < 0.05.
Discussion
To the best of our knowledge, this is the first study to assess the relationship between NEAT and PAL in COPD patients. We demonstrated that the total NEAT score was modestly correlated with PALDLW, steps/day, the duration of moderate non-locomotive activity, AEEACC, and PALACC, and was weakly correlated with the duration of moderate locomotive and light non-locomotive activities evaluated using an accelerometer.
TEEDLW is comprised of BMR, AEE, and DIT, while PALDLW is calculated using the equation TEEDLW/BMR; furthermore, AEE includes both intended exercise and NEAT. In this study, few participants performed vigorous locomotive and non-locomotive activity (3 and 0 participants performed vigorous locomotive and vigorous non-locomotive activity, respectively). Thus, it is reasonable that the NEAT score was modestly correlated with PALDLW. The accelerometer detected steps/day, as well as the duration of sedentary, light, moderate, and vigorous locomotive and non-locomotive activity, which included both intended exercise and NEAT. Moreover, the accelerometer underestimates AEE. 16 These observations led to weak-to-moderate correlations between the NEAT score and the duration of light and moderate activities as measured using the accelerometer. It was also noted that the non-locomotive NEAT more significantly contributed to PAL evaluated using the DLW method and the accelerometer than the locomotive NEAT did. Besides, we demonstrated that the locomotive NEAT score was correlated with PALDLW when GOLD 0 group was excluded. One possible reason is that the PAL of patients with GOLD 0 had the greatest variation. Larger studies including healthy control will need to conduct.
Although there are several questionnaires that measure and evaluate PAL in healthy individuals,26,27 there are no reports using questionnaires to evaluate PALDLW in COPD patients. Furthermore, it has been reported that the evaluation of PAL using a questionnaire is less sensitive than using an accelerometer; the accuracy of questionnaires is further decreased in the assessment of light physical activity, which is important in the assessment of PAL in COPD patients.28,29 In fact, Garfield et al. reported that the association between several questionnaires and PAL measured using an activity monitor was weak. 30 The NEAT questionnaire we used in the present study was modified, using the Adult Compendium of Physical Activities, according to the Japanese lifestyle and the score was correlated with PALDLW and light-to-moderate walking and daily activity duration. In addition, a previous report demonstrated that PAL measured using a triaxial accelerometer significantly correlated with the NEAT score in patients with type 2 diabetes. 14 In that study, total, locomotive, and non-locomotive NEAT scores were reported to be 63.2 ± 11.6, 19.5 ± 4.0, and 43.7 ± 9.7, respectively (male/female: 24/27, age: 58.5 ± 12.3, body mass index (BMI): 26.7 ± 5.2). These scores were slightly higher than those obtained from COPD patients in the present study, although the age, sex, and BMI differed between the groups, and control scores for healthy older Japanese adults are not available at present. However, these results indicate that this questionnaire is valid for Japanese patients with diabetes.
Presently, PAL is often objectively evaluated using pedometers or accelerometers. However, the data obtained from these devices may have poor reproducibility depending on the patient's mood, the weather, and whether they are correctly worn as instructed. In fact, a previous study reported that 88% of studies among COPD patients do not indicate how non-wear time was determined. 31 If patients do not wear the accelerometer correctly, it does not matter how objective the model is, PAL cannot be evaluated accurately. Furthermore, the accelerometer underestimates the intensity of physical activity in older adults. 32 We previously reported that the energy expenditure measured by the triaxial accelerometer underestimates that of the DLW method by approximately 215 kcal/day in COPD patients. 16 However, in the present study, the PAL measured using the triaxial accelerometer was also correlated with the total NEAT score.
Waschki et al. revealed that a decreased PAL and fewer steps in COPD patients have a significant negative impact on prognosis, 1 and that wearing a pedometer significantly increases the number of steps and leads to improvement in exercise capacity and quality of life. 33 This suggests that locomotive activity is essential for improving COPD outcomes. Conversely, we showed that the non-locomotive NEAT score was more strongly correlated with PAL in comparison to the locomotive NEAT score, suggesting that non-locomotive activities may be equally, or even more, important with respect to improving the physical status of COPD patients; however, further investigation is required. Hence, a stronger focus on the non-locomotive activities of COPD patients is warranted to enhance their PAL.
This study has several limitations. First, the sample size was relatively small (n = 36) owing to the difficulty in using the DLW method. Future studies with larger sample sizes are needed. Second, female patients were not included. Given that most (>90%) Japanese COPD patients are male34,35 and considering the small study sample size, unifying the sex of the sample was presumed reasonable.
Conclusion
In this study, we demonstrated that the NEAT score was correlated with PAL assessed using the DLW method in COPD patients. Accelerometers are occasionally problematic with regard to measuring PAL, and the DLW method is impractical for use in daily practice given its high cost and the expertize required for analysis. Therefore, the NEAT score may be an option for evaluating PAL in COPD patients in daily clinical practice owing to its convenience and cost-effectiveness.
Supplemental Material
sj-doc-1-sci-10.1177_00368504221117064 - Supplemental material for Impact of non-exercise activity thermogenesis on physical activity in patients with COPD
Supplemental material, sj-doc-1-sci-10.1177_00368504221117064 for Impact of non-exercise activity thermogenesis on physical activity in patients with COPD by Toru Shirahata, Yuki Nishida, Hideaki Sato, Sanehiro Yogi, Tomoe Akagami, Makoto Nagata, Shigeho Tanaka, Hidetoshi Nakamura and Fuminori Katsukawa in Science Progress
Footnotes
Acknowledgements
We thank Azusa Sasaki (National Institutes of Biomedical Innovation, Health and Nutrition, Tokyo, Japan) and Hitoshi Miyazawa (Saitama Medical University, Saitama, Japan) for their skillful technical assistance.
Author contributions
TS designed the study, collected and analyzed the data, and wrote the manuscript; HS, SY, TA, and YN collected and analyzed the data; FK and ST contributed to study design, data interpretation, and acquisition of funding; MN contributed to data interpretation; and HN contributed to study design, data interpretation, and acquisition of funding and has taken responsibility for the design and final content of the article. All authors have approved the final version of the manuscript.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Agency for Medical Research and Development (grant number JP17ek0210045 and JP20ek0210112.).
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.