
Abstract
Background and aims
Severe pneumonia represents a serious threat to the health of elderly individuals. This study aims to exploratory analyse the effect of B-type natriuretic peptide (BNP), the neutrophil to lymphocyte ratio (NLR), and APACHE II scores for assessing the 28-day mortality risk in elderly patients with severe pneumonia.
Methods
Our study enrolled 80 elderly patients with severe pneumonia (53 males and 27 females). The associations of NLR, oxygenation index (PaO2/FiO2), and acute physiology and chronic health score II (APACHE II) with 28-day mortality risk were assessed using multivariable logistic regression hazards model. The predictive value of BNP, NLR, and APACHE II scores for 28-day mortality risk in this patient population was assessed by receiver operating characteristic (ROC) curves.
Results
BNP (odds ratio [OR], 1.007; 95% confidence interval [CI], 1.002–1.012; P < 0.05), NLR (OR, 1.496; 95% CI, 1.002–2.192; P < 0.05), and APACHE II scores (OR, 1.411; 95% CI, 1.102–1.806; P < 0.05) were independent risk factors for 28-day mortality in elderly patients with severe pneumonia. ROC curve analysis demonstrated that the combination of BNP, NLR, and APACHE II scores exhibited a strong predictive value for 28-day mortality risk in elderly patients with severe pneumonia, with an area under the ROC curve (AUC) of 0.966 and a specificity of 87.10%.
Discussion and conclusion
This single-center retrospective analysis showed that elevated BNP levels (≥286.5 pg/mL), elevated NLR levels (≥15.76), and increased APACHE II score (≥25.5 points) were associated with an increased 28-day mortality risk in elderly patients with severe pneumonia.
Keywords
Introduction
The aging population is experiencing an annual increase in the incidence of pneumonia among elderly patients. An epidemiological study indicates that approximately 1 million cases of community-acquired pneumonia occur in elderly individuals in the United States each year, 1 and there is a continuous rise in the incidence of severe pneumonia within this demographic. 2 Factors such as aging, malnutrition, and various chronic diseases contribute to a relative compromise in the immune function of elderly patients. Severe pneumonia in this population often presents with a rapid onset and progresses quickly, which can easily lead to respiratory failure, 3 acute respiratory distress syndrome, 4 multiple organ dysfunction syndrome, 5 and other complications. 6 These conditions result in prolonged hospital stays, increased frequency of hospitalizations, elevated healthcare costs, and higher mortality rates among elderly patients. Consequently, elderly patients often require extended hospitalizations, which further escalate treatment costs and mortality risk. A study conducted in Iran highlights that elderly patients impose a significant burden on the national healthcare system and socio-economic structures. 7 Thus, it is clear that severe pneumonia represents a serious threat to the health of elderly individuals and poses a substantial challenge to public health systems.
In clinical practice, C-reactive protein, procalcitonin (PCT), microbial detection, and the pneumonia severity index (PSI) are commonly utilized as prognostic indicators for pneumonia. However, these indicators exhibit certain limitations, including poor sensitivity, lengthy processing times, and operational complexity.8–11 Consequently, there is an urgent need for more effective methods to assess the prognosis of severe pneumonia in this population. Recent studies have indicated that B-type natriuretic peptide (BNP) levels significantly increase during severe infections 12 and have been progressively employed to evaluate the condition of sepsis patients.13,14 Furthermore, some research suggests a potential correlation between BNP levels and the prognosis of community-acquired pneumonia.15–17 The neutrophil to lymphocyte ratio (NLR) is recognized as an important marker of systemic inflammation and has demonstrated predictive value in sepsis, 18 cardiovascular diseases, 19 and oncological conditions.18,20–22 Nevertheless, there is limited research regarding the application of these markers in assessing the prognosis of elderly patients with severe pneumonia. It remains unclear whether the combined testing of BNP, NLR, and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score can enhance the predictive efficacy for mortality in this demographic.
Therefore, this study targets the general elderly population aged ≥60 years (as clearly defined in the Methods) to fill the gap of insufficient data on the prediction of mortality risk in this understudied demographic. The aim was to evaluate the predictive value of B-type natriuretic peptide (BNP) and the neutrophil-to-lymphocyte ratio (NLR), in conjunction with the APACHE II score, for assessing the 28-day mortality risk in this patient population.
Materials and methods
Study population
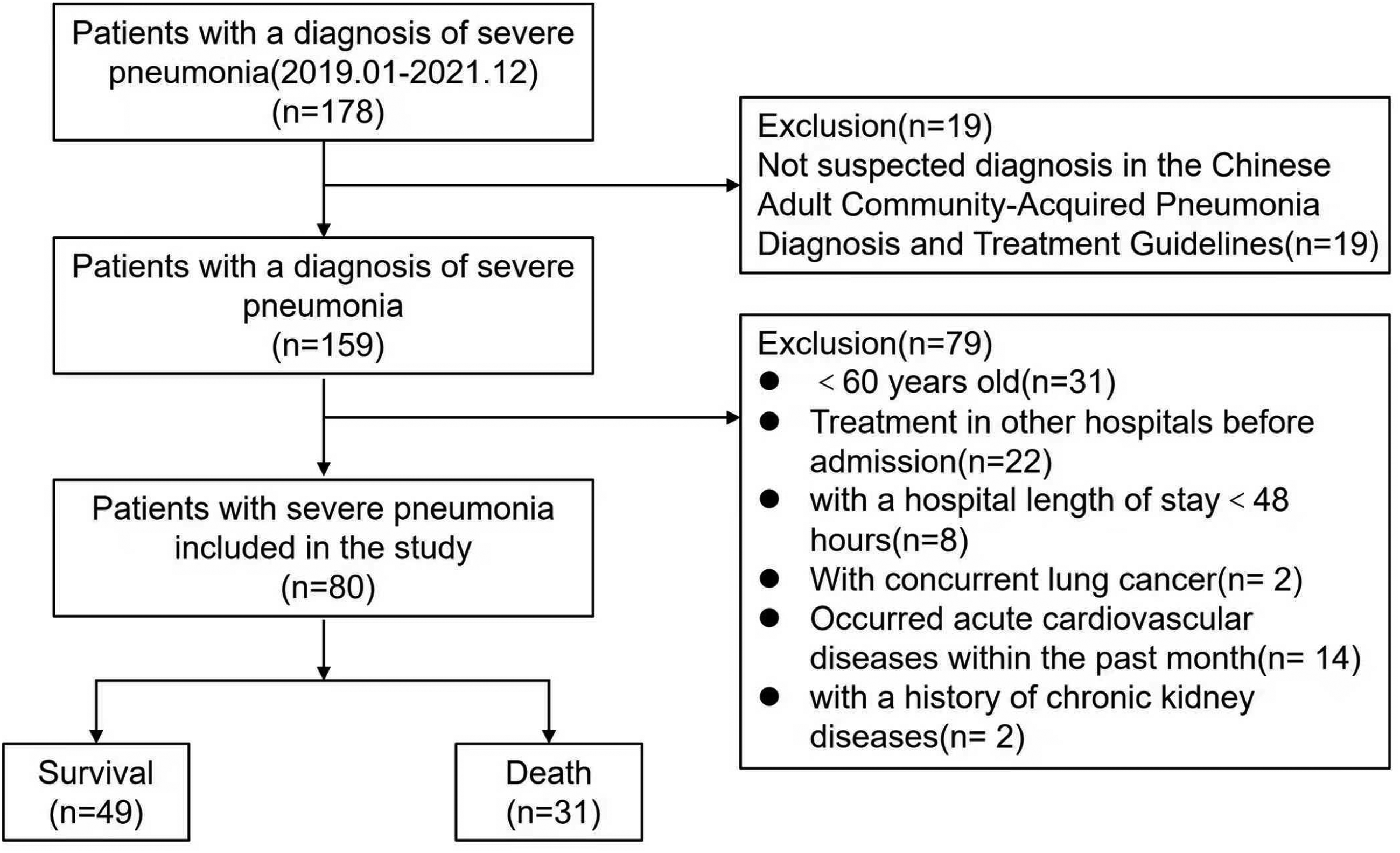
We selected clinical data from 80 elderly patients aged 60 years and older, who were admitted to our emergency and critical care departments with severe pneumonia between January 2019 and December 2021. Severe pneumonia is caused by inflammation of lung tissue (bronchioles, alveoli, interstitium) that progresses to a certain stage of the disease, worsens and forms, causing organ dysfunction and even endangering life. 23 This research comprised 53 male and 27 female patients, with ages ranging from 60 to 97 years, and a mean age of 78.39 ± 9.60 years. Based on their 28-day prognosis, the patients were categorized into a survival group (49 cases) and a death group (31 cases). In order to protect patient privacy, all the detailed information of the patients included in this study has been de-identified.
The inclusion criteria were as follows: (1) age ≥ 60 years(We have chosen to use the age range of 60 years old and above as the primary definition for “elderly people”.24,25); (2) patients meeting the diagnostic criteria for severe pneumonia as outlined in the Chinese Adult Community-Acquired Pneumonia Diagnosis and Treatment Guidelines (2016 edition) 23 ; (3) patients with a hospital length of stay ≥ 48 h; and (4) patients who had not received any treatment prior to admission.
The exclusion criteria included: (1) Patients with concurrent lung cancer, tuberculosis, or other pulmonary diseases; (2) Patients who have experienced acute cardiovascular or cerebrovascular diseases within the past month; (3) Patients with a history of severe diseases affecting the heart, liver, kidneys, blood, or endocrine system, as well as those with immunodeficiency; (4) Patients diagnosed with malignant tumors (including all hematological malignancies) or in the terminal stage of illness; and (5) Patients undergoing long-term treatment with immunosuppressants or steroids.
Ethics
This study was conducted strictly in accordance with the Helsinki Declaration of 1975 (revised in 2024). And the study was a retrospective analysis of selected patient data and does not involve any intervention measures on patients. Given the nature of the analysis, it meets the criteria for a waiver of informed consent. Furthermore, this study was approved by the Ethics Committee of Xi'an People's Hospital on May 11, 2022 (No. 20220021).
Methods
Clinical data for the included patients were collected through the hospital's electronic medical record system. All clinical data were classified and summarized as follows: (1) Basic information, including gender, age, length of hospital stay, and comorbidities such as diabetes, hypertension, coronary heart disease, cerebrovascular disease, and a long-term bedridden status (defined as bedridden for more than three months); (2) Clinical indicators recorded within 24 h of admission, comprising white blood cell count (WBC), procalcitonin (PCT), neutrophil count (NET), lymphocyte ratio (LYM), brain natriuretic peptide (BNP), liver and kidney function tests, Acute Physiology and Chronic Health Evaluation II (APACHE II) score,26,27 and the calculation of the neutrophil-to-lymphocyte ratio (NLR) and oxygenation index (PO2/FiO2); (3) Prognostic indicator, specifically the 28-day mortality rate. The tests of all the indicators included in this study were conducted by the Clinical Laboratory Center of Xi'an People's Hospital (Xi'an Fourth Hospital). This department has obtained ISO15189 laboratory certification and strictly follows standard operating procedures (SOP) during the testing process.
Statistical analysis
Continuous variables were presented as means ± standard deviations or as medians with inter-quartile ranges (IQRs), and were compared using the LSD-t test or the Mann-Whitney U test. Categorical variables were expressed as frequencies with percentages and compared using the χ2 test or Fisher's exact test. Multivariable analysis was conducted using binary logistic regression on the statistically significant variables identified in the univariate analysis, with results reported as odds ratios (OR) and 95% confidence intervals (CI). Receiver operating characteristic (ROC) curves were plotted, and the area under the curve (AUC) was evaluated to assess the predictive ability of BNP, NLR, and APACHE II scores for mortality risk in elderly patients with severe pneumonia. A two-sided P-value of < 0.05 was considered statistically significant. All data analyses were performed using SPSS version 20.0.
Result
Baseline characteristics
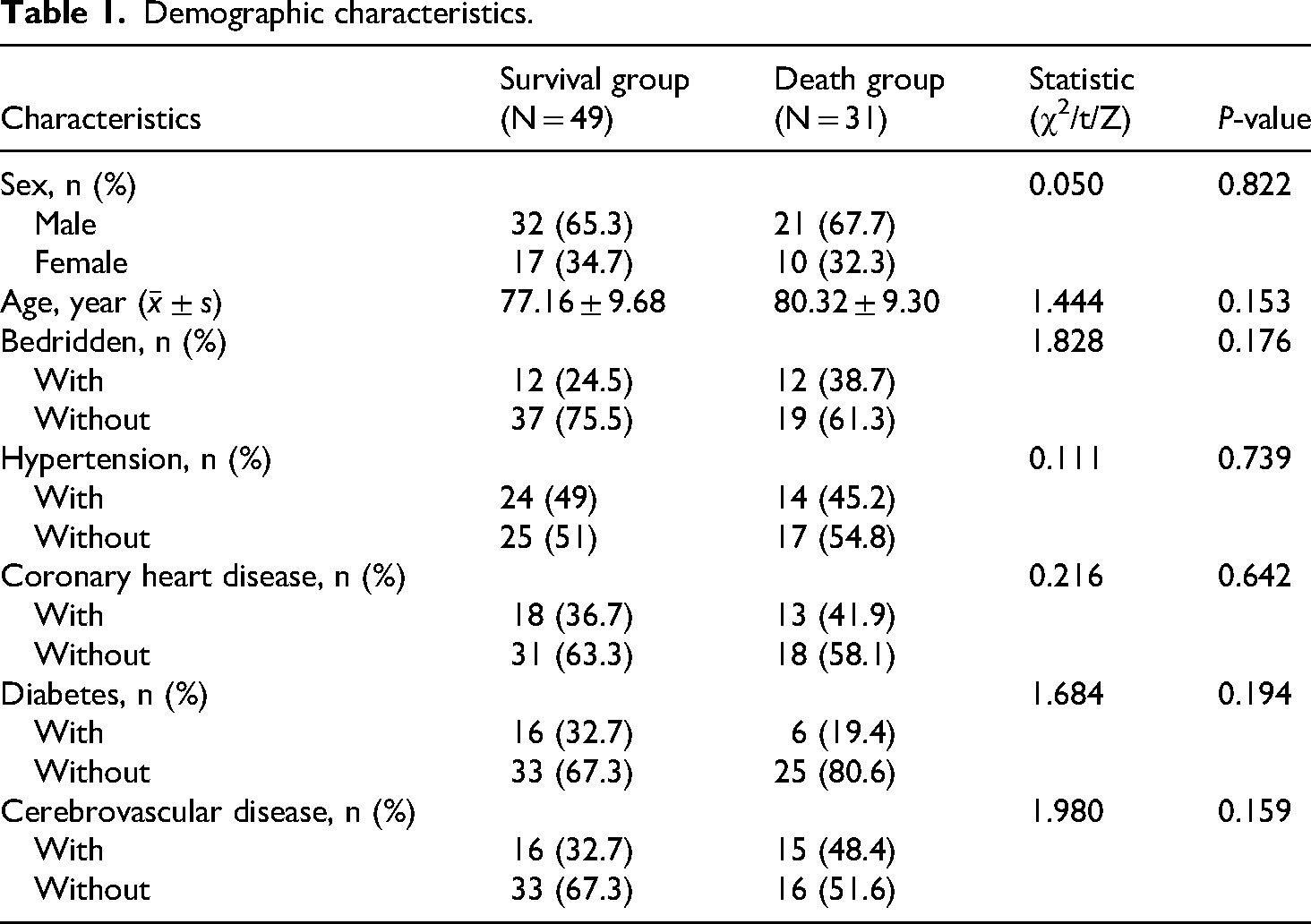
A total of eighty elderly patients with severe pneumonia were included in the final analysis, comprising 53 males and 27 females, with a mean age of 78.39 ± 9.60 years. Among these patients, 49 survived at 28 days (61.2%), while 31 died (38.8%) (Figure 1). There were no statistically significant differences between the two groups regarding gender, age, bedridden history, and comorbidities (P > 0.05) (Table 1).
Inclusion and exclusion criteria.
Demographic characteristics.
Comparison of clinical laboratory parameters between the two groups
Compared to the survival group, patients in the death group exhibited significantly elevated levels of WBC, PCT, NLR, BNP, and APACHE II scores upon admission, while ALB and PaO2/FiO2 levels were significantly decreased (P < 0.001). However, there were no statistically significant differences in platelet count, serum creatinine (SCr), alanine aminotransferase (ALT), or aspartate aminotransferase (AST) between the two patient groups (P > 0.05) (Table 2).
Laboratory parameters of elderly patients with severe pneumonia in the survival and death groups.

WBC: white blood cell count; NLR: the calculation of the neutrophil-to-lymphocyte ratio; BNP: brain natriuretic peptide; PCT: procalcitonin; PLT: blood platelet; SCr: Serum Creatinine; ALT: Alanine aminotransferase; AST: Aspartate Aminotransferase; ALB: Albumin; PaO2/FiO2: oxygenation index; APACHEII: Acute Physiology and Chronic Health Evaluation II.
Analysis of possible factors for death in elderly patients with severe pneumonia
An analysis of potential factors contributing to mortality in elderly patients with severe pneumonia was conducted. The significant indicators identified through univariate analysis were further examined using multivariate logistic regression. The results indicated that BNP (OR = 1.007, P < 0.05), NLR (OR = 1.496, P < 0.05), and APACHE II score (OR = 1.411, P < 0.05) emerged as independent risk factors for 28-day mortality in this patient population (Table 3).
Multivariate logistic regression analysis of mortality risk factors in elderly patients with severe pneumonia.
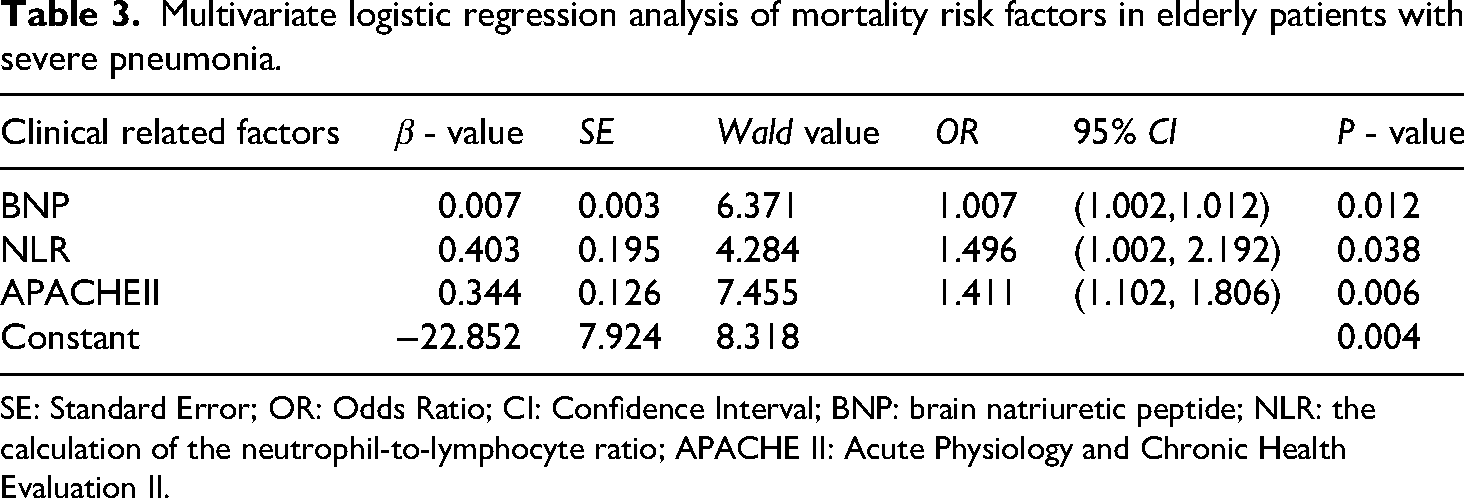
SE: Standard Error; OR: Odds Ratio; CI: Confidence Interval; BNP: brain natriuretic peptide; NLR: the calculation of the neutrophil-to-lymphocyte ratio; APACHE II: Acute Physiology and Chronic Health Evaluation II.
The effect of BNP, NLR, and APACHE II score for mortality risk in elderly patients with severe pneumonia
The results of the ROC analysis indicate that BNP, NLR, and APACHE II have a certain ability to distinguish the prognosis (survival/death) of elderly patients with severe pneumonia, with AUCs of 0.804, 0.907, and 0.907, respectively. The optimal cutoff value for BNP, determined by the maximum Youden's index, was found to be 286.5 pg/mL, yielding a sensitivity of 77.42%, a specificity of 73.47%, a positive likelihood ratio of 2.92, and a negative likelihood ratio of 0.31. For NLR, the optimal cutoff value was 15.76, resulting in a sensitivity of 87.10%, a specificity of 77.67%, a positive likelihood ratio of 3.88, and a negative likelihood ratio of 0.167. The optimal cutoff for the APACHE II score was 25.5 points, which provided a sensitivity of 90.30%, a specificity of 75.70%, a positive likelihood ratio of 3.688, and a negative likelihood ratio of 0.166. The combined AUC for BNP, NLR, and APACHE II scores was 0.966, with a sensitivity of 95.90% and a specificity of 87.10%, significantly surpassing the predictive capabilities of NLR, BNP, and the APACHE II score separately for assessing mortality risk in elderly patients with severe pneumonia (Table 4, Figure 2).

The ROC curve for the combined prediction of 28-day mortality risk in elderly patients with severe pneumonia by BNP, NLR, APACHE II, and various indicators upon admission.
Combined effect of BNP, NLR, APACHE II, and various indicators upon admission for predicting 28-day mortality risk in elderly patients with severe pneumonia.

AUC: Area Under Curve; CI: Confidence Interval; BNP: brain natriuretic peptide; NLR: the calculation of the neutrophil-to-lymphocyte ratio; APACHEII: Acute Physiology and Chronic Health Evaluation II.
Discussion
Despite continuous updates and improvements in treatment measures, the mortality rate of severe pneumonia remains high, particularly among elderly patients. The results of this study indicate that the 28-day mortality rate for elderly patients with severe pneumonia is 38.75% (31/80), which aligns with previous research findings approximately.28,29 This further underscores the elevated mortality rate among elderly patients suffering from severe pneumonia, and highlighting the need for vigilance among clinical practitioners. Consequently, timely assessment and early prognostic analysis of elderly patients with severe pneumonia could be of significant clinical value in reducing mortality rates, improving prognosis, and alleviating the societal healthcare burden.
The results of this study indicate that BNP was associated with 28-day mortality in elderly patients with severe pneumonia [OR 1.007, 95%CI (1.002, 1.012)]. Even after adjusting for confounding factors, it remained statistically significant, suggesting that BNP might be a potential factor associated with mortality risk in this population (AUC of 0.804, specificity of 73.47%), which aligns with the findings of Seo et al. 17 BNP, a significant cardiac biomarker synthesized and secreted by the ventricles, exhibits markedly elevated levels during instances of heart failure, myocardial infarction, and other forms of cardiac dysfunction. Research indicates that the incidence of myocardial infarction among patients hospitalized for pneumonia is approximately 7–8%. 30 In this study, we excluded patients with acute cardiovascular conditions such as acute coronary syndrome to prevent any potential influence on the research outcomes. Although the reasons for the notable increase in BNP levels among elderly patients with severe pneumonia remain unclear, several factors may contribute: 1) Tissue hypoxia may lead to pulmonary vasoconstriction, pulmonary hypertension, and right ventricular overload, thus promoting BNP secretion 31 ; 2) Inflammatory mediators, including interleukin-6, interleukin-1β, and TNF-α, have been shown to stimulate BNP release 32 ; 3) Advancing age may also contribute to elevated BNP levels. Importantly, our study further suggests that when BNP levels reach or exceed 286.5 pg/mL, the risk of mortality in these patients increases. This finding may alert clinicians to consider evaluating cardiac function in elderly patients with severe pneumonia who present with elevated BNP levels, while also formulating an appropriate and effective anti-infection strategy. It should be noted that, despite the exclusion of bias and confounding factors, the small OR values observed in the study results may be related to the limited sample size of this research, and further validation is required in subsequent studies.
As an inflammatory biomarker, the neutrophil-to-lymphocyte ratio (NLR) provides a more accurate reflection of the balance between neutrophil and lymphocyte responses, and correlates more effectively with the severity of inflammatory responses. Zhang HF et al. 10 demonstrated that NLR could enhance both the sensitivity and accuracy of the pneumonia severity index (PSI) score in predicting the 30-day mortality rate among patients with community-acquired pneumonia. Our study results indicate that neutrophil-to-lymphocyte ratio (NLR) levels in elderly patients with severe pneumonia who succumbed to the illness were significantly higher than those in the surviving research. Furthermore, multifactorial logistic regression analysis revealed that NLR serves as an independent risk factor for the 28-day mortality rate in this demographic [OR 1.496, 95%CI (1.002, 2.192)]. Specifically, the threshold value of NLR ≥ 15.76 correlates with an increased risk of death, which suggesting a poorer prognosis. Particularly worth mentioning is that NLR, derived from the ratio of neutrophils to lymphocytes, is readily obtainable from the complete blood count (CBC) test. This will be more conducive to the promotion and application in different healthcare institutions from different healthcare levels (primary, secondary, and tertiary healthcare levels). Moreover, as the cost of blood routine tests is relatively low, this may be helpful to reduce patients’ hospitalization expenses to some extent and alleviate the national healthcare burden.
The APACHE II score serves as a valuable prognostic tool for critically ill patients,26,27 with elevated scores correlating with increased mortality rates. This study indicates that an APACHE II score of ≥25.5 points is significantly associated with an elevated risk of mortality in elderly patients suffering from severe pneumonia [OR 1.411, 95%CI (1.102, 1.806)]. Nonetheless, the exclusive reliance on the APACHE II score presents certain limitations, 33 including diminished accuracy and sensitivity in specific populations, such as elderly patients with dementia or those with ambiguous medical histories.
Previous studies have indicated that the integration of blood biomarkers with validated clinical prediction scores can enhance predictive performance. 17 The findings of this study reveal that the combination of B-type natriuretic peptide (BNP) and neutrophil-to-lymphocyte ratio (NLR) yields an area under the curve (AUC) of 0.936, which is comparable to, or even exceeds the predictive performance of the APACHE II score alone (AUC of 0.905). Furthermore, the combined application of BNP, NLR, and APACHE II scores for prognostic assessment in elderly patients with severe pneumonia significantly surpasses the prognostic evaluation based on any single indicator, which achieving an AUC of 0.966. These results maybe suggest that BNP and NLR could substantially enhance the efficacy of APACHE II in predicting the 28-day mortality risk among elderly patients with severe pneumonia. The clinical integration of BNP, NLR, and APACHE II scores may address the limitations associated with relying on a single indicator for patient assessment, thereby providing improved predictive value for the prognosis of elderly patients with severe pneumonia in the early stages of the disease. This approach offers clinicians a more comprehensive theoretical foundation, assisting healthcare professionals in identifying high-risk patients early on. Consequently, this enables clinician to make the implementation of more precise and effective diagnostic and treatment strategies, rigorous monitoring, and timely interventions to prevent complications, ultimately enhancing patient prognosis and reducing mortality rates. One point that needs to be clarified is that the AUC in this study merely reflects the initial performance of the model, and the final prognostic value should be determined based on the external validation results.
This study has several limitations. First, it is a single-center retrospective analysis with a relatively small sample size, which may have resulted in incomplete data collection, potential selection bias and overestimation of the AUC value. Second, the model explored in this study lacks external validation, and the generalization capability of the model is unknown. Finally, the analysis was restricted to the BNP, NLR, and APACHE II scores recorded at admission, without the benefit of dynamic monitoring throughout the disease course. To address these limitations, subsequently, the external validation and update of the model will be accomplished by increasing the sample size and conducting multi-center prospective studies. And implement dynamic monitoring to explore the relationship between changes in these indicators and the progression of severe pneumonia. Additionally, our study population consisted of individuals aged 60 years or older, which may not fully capture potential heterogeneity within this age group. In future studies, stratified analysis by age might be conducted to further explore this issue.
In summary, this study demonstrates that elevated BNP levels (≥286.5 pg/mL), elevated NLR levels (≥15.76), and increased APACHE II score (≥25.5 points) were associated with an increased 28-day mortality risk in elderly patients with severe pneumonia. And the combined application of BNP, NLR and APACHE II score may be more meaningful for assessing the 28-day mortality risk of elderly patients with severe pneumonia. The above conclusion requires further verification through prospective studies.
Footnotes
Abbreviations
Ethics approval and consent to participate
This study was carried out in accordance with the International Conference on Good Clinical Practice Standards and the Declaration of Helsinki. All study protocols were approved by the Ethics Committee of Xi'an People's Hospital (Xi'an Fourth Hospital) (No. 20220021). The requirement of informed consent from the study subjects or their guardians was waived due to the deidentification of information in this retrospective study.
Consent for publication
Not applicable.
Authors’ contributions
Fu Wei and Jueheng Liu shared first authorship. Fu Wei contributed to methodology, software, validation, formal analysis, investigation and writing of the original draft. Jueheng Liu contributed to software, validation, formal analysis, and supervision. Tianlu Chen contributed to investigation. Sirui Ma contributed to methodology, validation and project administration. Jian Wang contributed to conceptualization, methodology, validation and project administration. All authors contributed to resources, writing, reviewing and editing. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Xi'an Health Commission, (grant number NO.2024yb34).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.