
Abstract
Spontaneous colonic perforation in adults (SCPA) is rare but important. Its clinicopathological features and outcomes remain unclear. Therefore, the aim of the current study was to explore and investigate the clinicopathological characteristics, clinical outcomes and potential risk factors for patients with SCPA. Data of seven patients with SCPA treated in our hospitals from January 2008 to December 2017, and 221 cases from research databases before 2018 were retrospectively analyzed. The description of SCPA included stercoral perforation of the colon (SPC), idiopathic perforation of the colon (IPC) and spontaneous colonic perforation (SCP) in the study. All SCPA patients presented with unexplained abdominal pain and peritonitis. The median age was 62.5 years. The definite diagnosis preoperatively was 20.6%. The commonest lesion location was sigmoid colon and Hartmann’s operation accounted for 59.3%. Histopathology of stercoral perforation (HSP) and histopathology of idiopathic perforation (HIP) were two histopathological findings. Postoperative complication was 67.7% and mortality was 31.1%. Univariate and multivariate analyses showed that chronic constipation was an independent risk factor for histopathological features (p ≤ 0.001, p = 0.005). Age of patients was associated with both postoperative complication (p = 0.012, p = 0.044) and mortality (p = 0.013, p = 0.034). Univariate analysis showed that HSP was associated with postoperative complication (p = 0.015). Our findings from the analysis pertaining to SCPA confirm those from previous studies, supporting the SCPA, as a uniform description, is an infrequent and life-threatening disease requiring early surgical intervention. We found that the elderly with chronic constipation was a high-risk category and those with HIP had a more favorable outcome than that of patients with HSP.
Keywords
Introduction
Spontaneous large bowel perforations not associated with disease or trauma, especially colonic perforations, are not common in adult populations. Spontaneous colon perforation in adults (SCPA) is rarely reported in the literature. It can be defined as an abrupt perforation of normal colon without tumor, diverticulosis, or traumatic disease, and is characterized by difficulty in diagnosis before surgery and high mortality. 1 Unexplained abdominal pain and perforating peritonitis are fairly common emergencies for surgeons and they can be life threatening if not diagnosed and treated early. 2 Nevertheless, due to the lack of a case series related to SCPA, its clinicopathological characteristics and outcomes remain unclear.
As early as in 1827, Sir Benjamin Brodie first reported a case of spontaneous rupture a normal colon. 3 Sixty years later, a sudden perforation of the normal colon was further described and classified as “stercoral” and “idiopathic” perforation by Berry. 4 Afterwards, idiopathic intestinal perforation was described as spontaneous bowel perforation.5,6 To be sure, there have been various descriptions of this disease such as “stercoral” perforation, “idiopathic” perforation, “spontaneous” perforation, “spontaneous stercoral” perforation, etc. It is currently described as stercoral perforation of the colon (SPC), idiopathic perforation of the colon (IPC), and spontaneous colonic perforation (SCP) in the published literatures, among which the majority appear to be reported by SPC. 2 Nevertheless, there may be some differences between them. Indeed, spontaneous perforation of the colon was a rare disease that was previously classified into stercoral and idiopathic perforation of the colon.1,5 In their opinion, the main differences between stercoral and idiopathic perforation were the macroscopic and histological manifestations of perforation, which had not yet been extensively studied. Although the two-type classification of SPC and IPC had been proposed and there were sporadic case reports, the description of the disease in the literatures was still inconsistent. Moreover, the published literature did not provide reliable information whether this rare entity was the same in children or adults. 7 Based on these reasons, we uniformly described it as SCPA.
In reality, because of its rarity, evaluating its clinicopathological profiles and other physical findings is quite challenging. However, a prospective study by Maurer et al. 8 found that stercoral perforations accounted for approximately 1% of all emergency colon surgery and 3% of all colon perforations, suggesting that the true incidence may be higher than previously thought. Furthermore, the condition may represent 2% of randomly selected autopsy examinations. 9 Up to now, however, data on the clinicopathological characteristics and outcomes of SCPA remain limited, and all studies in the literature are case reports.
In the current study, we collected data on 228 patients with SCPA in order to explore and analyze the clinicopathological characteristics and outcomes of SCPA. We also investigated potential risk factors that may be associated with SCPA.
Patients and methods
The cases of spontaneous colonic perforation in adults (SCPA) were from our center and in addition from the literature. From January 2008 to December 2017, seven patients with SCPA were diagnosed and treated in our center. A literature search was conducted on the research database (MEDLINE) for all articles published in English from 1998 to 2017. MEDLINE retrieved 39 case reports,7,10–47 including 46 patients, and four case series including 175 patients.1,2,5,48 To this end, a total of 228 patients with SCPA were identified (Figure 1). In particular, all enrolled and qualified cases were collectively referred to as SCPA, including SPC, IPC, and SCP. Among them, our seven cases were described by SCP (Table 1). The criteria for case inclusion were as follows: (1) Ages of the patients were more than 18 years old; (2) The patients complied with definition of spontaneous colonic perforation. Exclusion criteria: (1) Colonic perforation due to potential disease or injury; (2) Cases of colonic perforation found after surgery or other types of invasive surgery. Two patients were excluded because of the lack of histological examination after surgery. Seven patients with SCP were enrolled in our case series.

Schematic diagram regarding selection of SCPA.
Clinicopathological characteristics and outcomes of 228 cases of SCPA.

SCPA: spontaneous colonic perforation in adults; SPC: stercoral perforation of the colon; IPC: idiopathic perforation of the colon; SCP: spontaneous colonic perforation; HSP: histopathology of stercoral perforation; HIP: histopathology of idiopathic perforation.
According to the diagnostic criteria reported by Maurer et al., 8 SPC were listed as follows: (1) A round or oval antimesenteric perforation was larger than 1cm in diameter; (2) there were fecalomas in the colon, protruding through the perforation site or lying within the abdominal cavity; (3) Histological evidence of multiple pressure ulcers and acute inflammatory reaction around the perforation; and (4) There was no external injury, diverticulitis or obstruction due to neoplasm or adhesions. Compared to SPC, IPC has the following features: (1) A linear or snatchy antimesenteric colonic perforation was less than 1cm in diameter; (2) Feculent ulcer did not be seen at microscopic examination. The mucosal edge was clear and did not extend to the serosa; (3) The broken ends of the muscular layer were neat 49 ; The condition’s definition depended on the absence of any detectable pathology in the bowel wall that could be responsible for the perforation, in light of the review reported by Losanoff et al. 7 For research purposes, the histopathological features of the above two conditions were referred to as histopathology of stercoral perforation (HSP) and histopathology of idiopathic perforation (HIP), respectively. According to the criteria, these seven cases are attributed to our case series known as SCP (Table 2). In addition, some clinicopathologic characteristics and outcomes of 175 patients with SCPA in four case series were listed separately (Table 3). This study was approved by the Ethics Committee of Cangzhou Clinical College of Integrated Traditional Chinese and Western Medicine of Hebei Medical University (IRB: CZ-KY-2018-033), and written informed consent was obtained from the seven patients in our hospitals.
Clinicopathological characteristics and outcomes of seven patients with SCP in our case series.
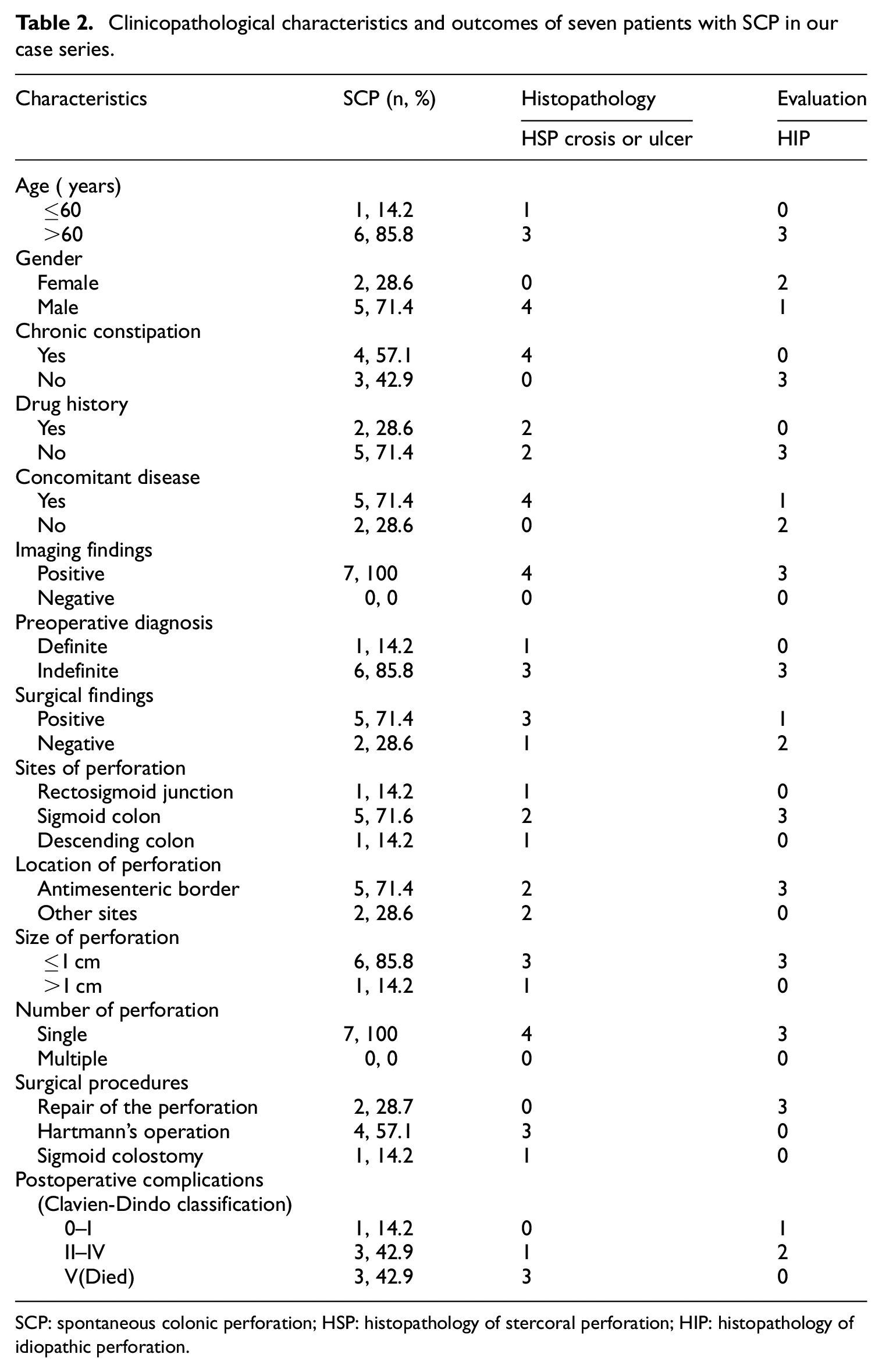
SCP: spontaneous colonic perforation; HSP: histopathology of stercoral perforation; HIP: histopathology of idiopathic perforation.
Clinicopathological characteristics and outcomes of 175 patients with SCPA in four clinical studies.

SCPA: spontaneous colonic perforation in adults; SPC: stercoral perforation of the colon; IPC: idiopathic perforation of the colon; SCP: spontaneous colonic perforation; ys: years.
Clinicopathologic data, including age, sex, symptoms, history of constipation, drug history, comorbidity, imaging findings (preoperative X-ray, CT), preoperative diagnosis, surgical findings, lesion size, location of perforation, sites of perforation, number of perforation, surgical procedures, histopathologic findings, postoperative complications, and clinical outcomes were recorded from hospital medical documents or extracted from published reports and studies.
All statistical analyses were performed with the statistical package IBM SPSS statistics version 22.0 software. Discrete variables were analyzed using Chi-square test or Fisher exact test. Numerical variables were expressed as the mean SD unless otherwise stated. Significant related factors for SCPA identified by univariate analysis were further assessed by multivariate analysis using the logistic regression analysis. The related factors for histopathology, postoperative complication and mortality among patients with SCPA were analysed using Cox regression models. In addition, Clavien-Dindo Classification was used in surgical outcome assessment. 50 A p value of less than 0.05 was considered to indicate statistical significance.
Results
Descriptive and clinicopathologic data of extracted SCPA cases are given in Table 1. Overall, a total of 228 cases of SCPA were identified. All of the cases in the present series presented with unexplained abdominal pain and localized or generalized peritonitis. About 76.8% of them had a history of chronic constipation. The median age was 62.5 years (range from 27 to 86). No intergroup (SPC, IPC, and SCP) difference was found in clinical data. The number of reports by SPC was approximately 76.7%. The majority of SCPA patients had positive imaging findings (209/228, 91.7%), but the preoperative diagnosis rate was only 20.6% (13/63). They all underwent surgery. The most common location of SCPA was sigmoid colon (124/228, 54.1%), followed by rectosigmoid junction (49/228, 21.5%), descending colon (31/228, 13.6%), transverse colon (22/228, 9.6%), cecum (9/228, 3.9%) and ascending colon (3/228, 1.3%). Fifty-four patients underwent Hartmann’s operation (54/91, 59.3%), twenty-three patients underwent perforation repair or colectomy (23/91, 25.3%), colostomy (13/91, 14.3%), and one patient treated with hemicolectomy (1/91, 1.1%). According to Clavien-Dindo classification, the incidence of postoperative complications was 67.7% (44/65) and the postoperative mortality rate was 31.1% (71/228).
Histopathological data included our cases of 91 patients were eventually selected for analysis (Table 1). Among them, 36 patients showed almost normal pathological manifestations (HIP), accounting for 39.6%. Interestingly, another 13 patients with SPC or SCP rather than IPC cases revealed normal mucous membrane (HIP). According to histopathological features, our cases were showed in Table 2. We found that there was a difference in histopathology, including the HSP in four cases and HIP in three cases (Figure 2).

(a) Histopathology of stercoral perforation (HSP): Superficial ulcer. There was numerous neutrophil infiltration at the edge of the ulcer. (b) Histopathology of idiopathic perforation (HIP): Normal mucous membrane of the colon. There was no inflammatory sphacelus and abundant neutrophil infiltration around the perforation.
Related factors for 53 patients with SCPA were shown in Table 4. Age was associated with postoperative complication (p = 0.012, p = 0.044) and mortality (p = 0.013, p = 0.034) of SCPA. Chronic Constipation was an independent risk factor for histopathological features (HR:0.056, CI:0.012–0.255, p≤0.001; HR:0.001, CI:0.000–0.133, p = 0.005). In addition, univariate analysis showed that HSP appeared to be associated with postoperative complications of SCPA (HR: 0.204, CI:0.027–0.734, p = 0.015) and thus influenced mortality. In other words, chronic constipation patients are more likely to develop HSP, and it may lead to higher complication rate and mortality rate.
Related factors for histopathology, postoperative complication and mortality among 53 patients with SCPA using univariate and multivariate cox regression models.

SCPA: spontaneous colonic perforation in adults; CI: confidence interval; HSP: histopathology of stercoral perforation; HIP: histopathology of idiopathic perforation; vs.: versus. The bold values indicate that the value is statistically significant.
Discussion
Clinicopathologic features and outcomes of SCPA are limited due to the extremely low incidence. It is scarcely feasible to design prospective clinical trials for an infrequent disease often requiring emergency treatment. Therefore, we evaluated data of 228-pooled SCPA from our center and from literatures with regard to clinicopathologic features, risk factors, treatment and outcome. This study represents the largest analysis of SCPA and indicates some characteristics that are significantly related to SCPA.
Up to now, the largest cases of SCPA (described as SPC) was reported by Chakravartty et al., 2 which contained 137 cases. The distribution of age, chronic constipation, imaging findings and mortality were similar to the present study. However, a few highlights with respect to clinicopathological characteristics were revealed and the outcomes of SCPA were analyzed in-depth in our study.
In the present study, we found that SCPA commonly occured in patiens over 60 years old and there was no difference in gender. About 76.8% of them had a history of chronic constipation. This was consistent with the report by Tsutomu Namikawa et al. 5 No intergroup difference was found in clinical data though the number of reports by SPC was approximately 76.7%. Perhaps this is the reason why SPC has so many names. Imaging findings were positive in the vast majority of patients, but the preoperative diagnosis rate was 20.6%. In light of the work of Serpell and Nicholls, 3 only 11% of SCPA were correctly diagnosed before operation. Apparently, the preoperative diagnosis rate of SCPA in our study was relatively higher than that previously reported.
Our results showed that the most common location of SCPA was sigmoid colon and Hartmann’s operation accounted for 59.3%; and the incidence of postoperative complications was 67.7% and the mortality rate was 31.1%. According to univariate and multivariate analyses, chronic constipation was an independent risk factor for histopathological features, and Age was associated with both postoperative complication and mortality of SCPA. Our findings are consistent with at least a couple of several other studies.1,3,19,33,34
An early diagnosis is crucial to reduce complication rate and mortality of SCPA patients. Unfortunately, the diagnosis of SCPA before surgery is very difficult. First, due to the extremely rare incidence, the disease is not yet known. In addition, the imaging manifestations of SCPA are not specific. They usually have unexplained abdominal pain, which show no differences with other senile acute abdomen. According to the review reported by Chakravartty et al., 2 an early CT scan will easily diagnose the condition and shorten the interval to surgery, which is the most important factor in reducing mortality. Indeed, CT images provide useful findings such as free air, dirty mass, dirty fat sign, extraluminal fluid collection and bowel wall thickening around the perforation site.51,52 Nevertheless, it is very difficult to specify the cause of perforation. About 91.7% of the cases in the present series had imaging findings of either free air or dirty mass. Of them, only 13 patients were diagnosed preoperatively.
Here, we also discuss the incidental finding of free air on imaging and its relationship to SCPA. In clinical practice, the radiographic presence of intraperitoneal air often is believed to be a diagnostic finding one. Multiple signs of free intraperitoneal air can be found on plain films, especially in supine abdominal radiographs, and on CT examinations, but is less likely to determine the exact etiology. 53 According to the literature,53–55 pneumoperitoneum reflects visceral perforation, including SCPA, in 85% to 95% of all occurrences. In 5% to 15% of cases, however, pneumoperitoneum does not reflect perforation and results from another source that does not require emergency surgery. It belongs to the nonsurgical pneumoperitoneum and may be derived from the following four categories: abdominal, thoracic, gynecologic, and idiopathic. 55 It is characterized by absence of clinical symptoms and signs, such as abdominal pain, abdominal distension, and signs of peritonitis. According to Richard A et al., when abdominal pain and distension are minimal, and peritoneal signs, fever, and leukocytosis are absent, nonsurgical causes of pneumoperitoneum should be considered for subsequent conservative management. 55 Obviously, the incidental finding of free air on imaging cannot qualify as SCPA. In fact, SCPA patients may present with a variety of symptoms, but infrequently are asymptomatic.
In terms of treatment, due to the extreme rarity of SCPA, there are no guidelines related to SCPA in the literature. In general, the disease is treated using similar strategies as those used to treat traumatic bowel perforation. At present, early surgical intervention is considered to be the optimal treatment. In the present study, we collected the surgery data of 91 cases of SCPA, and showed the Hartmann’s operation and perforation repair or colectomy were 58.9% and 25.6%, respectively. Furthermore, in our study, we found that the surgical procedures of SCPA had no relationship with postoperative outcomes, which may indicate that surgical intervention is in full force and effect on patients with SCPA. On the contrary, the mortality rate after Hartmann’s procedure were lower than that of other operations, in light of the work of Serpell and Nicholls 3 To sum up, timely diagnosis and treatment is the best way to prevent an unfavorable outcome in SCPA patients, and it begins with clinical suspicion. As mentioned above, the open Hartmann’s procedure was the most commonly performed operation in these patients. With the development of laparoscopic surgery, however, alternative approaches to perforated peritonitis have been adopted increasingly, including colonic resection with primary anastomosis with or without defunctioning stoma, and nonresectional strategies such as laparoscopic lavage and drainage. 56 Several recently published studies suggest that laparoscopic lavage has a good prognosis. The 12-month results of the DILALA trial57,58 showed laparoscopic lavage to be feasible and safe in patients with purulent peritonitis. A recently published study by A. Kohl et al. shows that laparoscopic lavage is a better option for perforated diverticulitis with purulent peritonitis than open resection and colostomy. 59 Based on the above discussion, laparoscopic lavage has been suggested as an alternative treatment for traditional surgery in patients with perforated peritonitis. Although there are no such procedures used in our case series, we believe that laparoscopic lavage may be therapeutic options for SCPA patients.
Currently, there are no studies in the literature focusing on risk factors for SCPA. The available evidence is mainly supported by retrospective series. Our findings suggested that chronic constipation was an independent risk factor for histopathological features (HSP vs. HIP), and the elderly with unexplained abdominal pain and chronic constipation were high-risk category for SCPA. Additionally, there are no studies in the English literature focusing specifically on comparing the different types of histopathology (HSP vs. HIP) for SCPA. In the present study, we performed this pooled study and compared differences between the two types. As a result, the prognosis of patients with HIP appears to be better than that of patients with HSP.
To date, the precise etiology of SCPA remains unclear. Some theories have been proposed to explain its pathogenesis including ischemia, high intraabdominal or intraluminal pressure, colonic implosion, attenuation of the bowel wall, or laceration of the latter from hard feces, but these factors have not been supported by existing evidence.60,61 The limited number of studies so far support that early recognition and treatment lead to a favorable outcome for most patients with SCPA. Further research into the ultrastructure of the colon is expected to yield more information about SCPA. 7
This study has certain limitations. First of all, our research is a retrospective analysis. The lack of systematic prospective data acquisition has limited the integrity of some data. This may affect the analysis of clinicopathological features and clinical outcomes. Second, the heterogeneity of data selection based on registry data, case reports and small case series does not preclude some selection bias. However, our work provides important information of the largest cohort of SCPA to date.
Conclusion
Our findings from the analysis of data pertaining to SCPA confirm those from previous studies, supporting the uniform definition that SCPA is an infrequent, hard to diagnose preoperatively and life-threatening disease requiring early surgical intervention. The most frequent location for SCPA was the sigmoid colon, followed by rectosigmoid junction. Chronic constipation was an independent risk factor for SCPA. The elderly with chronic constipation was a high-risk category. Clinical outcomes of patients with HIP might be better than that of patients with HSP.
Footnotes
Acknowledgements
The authors would like to thank all our participants in this study.
Author contributions
Ren Chongxi designed and instructed this study. Ren Chongxi and Ji Jinggang drafted the manusript. Ji Jinggang, Shi Yan, Liu yan and Yang Fengshuo searched literatures. Ji Jinggang, Shi Yan, Wang Hongqiao and Yang Fengshuo input the data; Ren Chongxi, Ji Jinggang and Yang Fengshuo analyzed the data. Ren Chongxi, Wang Hongqiao and Liu yan revised the manusript. All authors reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Ethics Committee of Cangzhou Clinical College of Integrated Traditional Chinese and Western Medicine of Hebei Medical University (IRB:CZ-KY-2018-033).
Informed consent
Written informed consent was obtained from the seven patients in our hospitals.